Whole30 — Structured 30-Day Elimination Reset
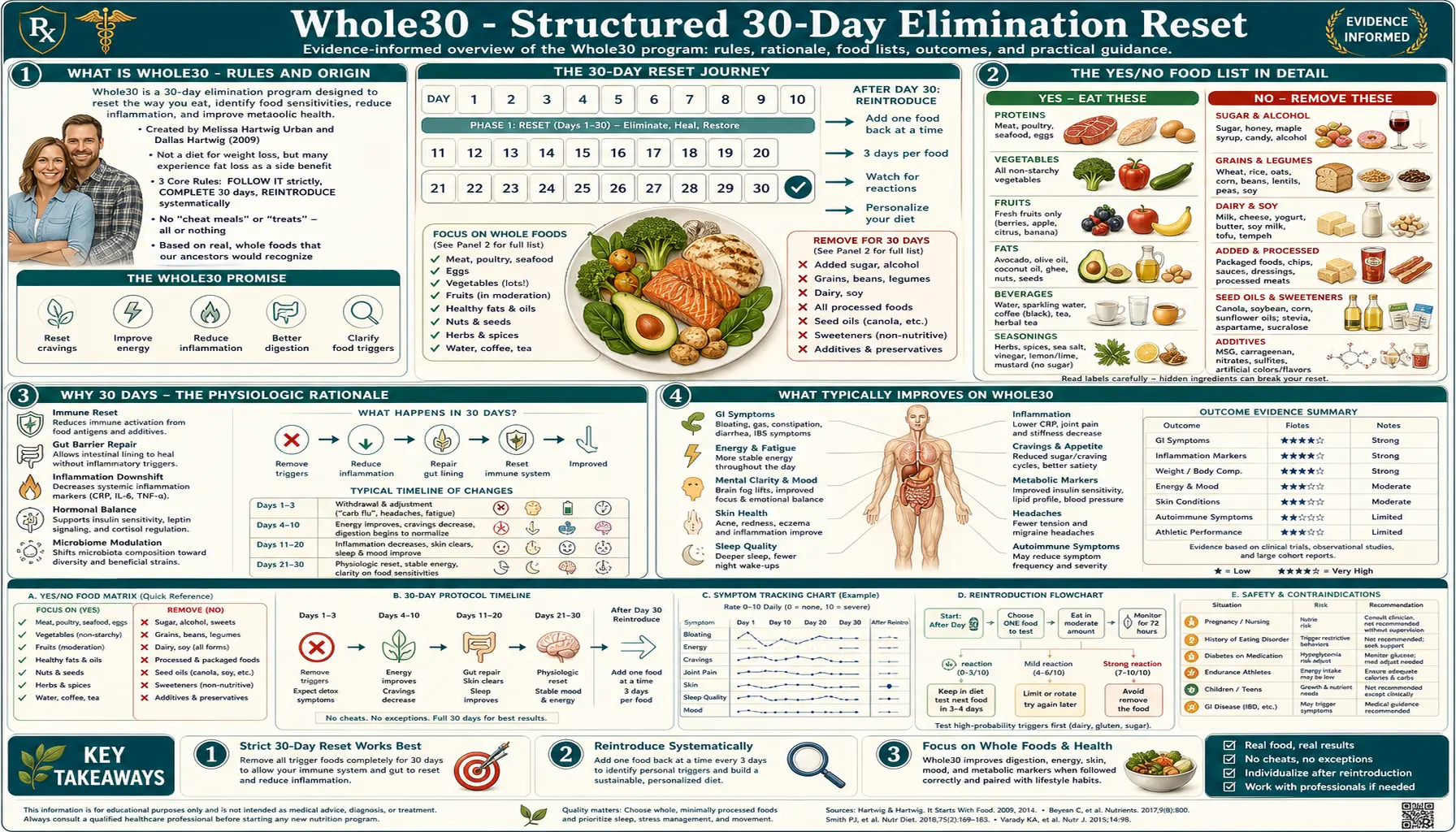
Whole30, created by Melissa Hartwig-Urban and Dallas Hartwig in 2009, is the most widely adopted structured elimination program in the United States. For 30 consecutive days, participants eliminate grains, legumes, dairy, all added sugars and most non-caloric sweeteners, alcohol, and processed seed oils — eating only whole, unprocessed meat, seafood, eggs, vegetables, fruit, and natural fats. The program's strength is its simplicity (a clear yes/no food list, no calorie counting, abundant published recipes) and the community infrastructure that supports adherence. Its weakness is the lack of a built-in reintroduction protocol — participants who skip the post-Whole30 reintroduction phase miss most of the diagnostic value. This page walks through how Whole30 works, who benefits most, the documented physiologic effects, the formal reintroduction steps that turn the 30-day reset into actual elimination-diet methodology, and the common pitfalls to avoid.
Table of Contents
- What Is Whole30 — Rules and Origin
- The Yes/No Food List in Detail
- Why 30 Days — The Physiologic Rationale
- What Typically Improves on Whole30
- The Formal 10-Day Reintroduction (Often Skipped)
- Who Benefits Most — and Who Should Not Try It
- Common Pitfalls and Failure Modes
- Whole30 vs Paleo vs AIP — Where It Sits
- Practical Meal Planning
- Key Research Papers
- Connections
- Featured Videos
What Is Whole30 — Rules and Origin
Whole30 was launched in 2009 by Melissa Hartwig (now Hartwig-Urban) and her then-husband Dallas Hartwig as a blog-based 30-day nutritional reset within the broader Paleo movement. The flagship book, The Whole30: The 30-Day Guide to Total Health and Food Freedom, was published in 2015 and reached #1 on the New York Times bestseller list. As of the mid-2020s the program has produced multiple companion cookbooks, a certified coach training program, branded grocery-store products, and an active social-media community of millions.
The rules are intentionally simple and unambiguous — what the founders call the "tough love" framing. For 30 consecutive days you eat:
- Yes: Whole, unprocessed meat, seafood, and eggs. All vegetables. Most fruit. Natural fats (avocado, olive oil, ghee, coconut oil, nuts and seeds in moderation). Herbs, spices, vinegars (except those with added sugar).
- No: All grains (wheat, rice, corn, oats, quinoa, etc.). All legumes (beans, lentils, peanuts, soy in all forms including tofu, tempeh, edamame, soy sauce). All dairy (milk, cheese, butter, yogurt — ghee is allowed). All added sugar and most non-caloric sweeteners (cane sugar, honey, maple syrup, stevia, monk fruit, agave, etc.). All alcohol, including for cooking. Most processed seed oils (canola, soybean, sunflower, safflower, corn). Carrageenan, sulfites, and MSG.
- No "Paleo treats": A distinctive rule is the prohibition on Paleo-compliant recreations of off-limits foods — no pancakes made from coconut flour and banana, no almond-flour pizza crust, no Paleo "ice cream" from blended frozen banana. The reasoning is psychological — the program aims to break the cookie-cake-bread-pasta craving cycle, and ostensibly-compliant baked goods reinforce it.
- No weighing yourself: Stepping on a scale or taking body measurements during the 30 days is prohibited. The program is explicitly not framed as a weight-loss diet — the founders argue that the scale fixation undermines the broader behavioral and metabolic goals.
- No tracking calories or macros: Participants eat to appetite from the approved food list, without measurement. The rationale is that fiber-, protein-, and fat-rich whole foods are inherently more satiating than processed foods, so portion control becomes automatic.
- One slip restarts the clock: A documented single conscious off-protocol bite resets the count to day 1. This zero-tolerance rule is the most controversial feature of the program and the one most often modified in practice.
The program was designed to be a structured behavioral and dietary reset, not a long-term eating pattern. Hartwig has been explicit that Whole30 is not meant to be done indefinitely — the value is in the 30-day intervention followed by an informed return to a personalized diet, not in permanent restriction.
The Yes/No Food List in Detail
The Whole30 food list is the program's defining feature. Compared to general "Paleo" diets, Whole30 is somewhat more restrictive on sweeteners (no honey or maple syrup, which most Paleo variants allow), more restrictive on alcohol (none vs occasional wine in Paleo), and identically restrictive on grains, legumes, and dairy. A practical breakdown:
Approved categories:
- Animal protein: Beef, lamb, pork, poultry, fish, shellfish, eggs, organ meats. Bacon and sausage are allowed only if they contain no sugar, no soy, no carrageenan — in practice, this rules out about 90% of commercial brands. Whole30-compliant bacon and sausage exist but require label-reading.
- Vegetables: All vegetables, including starchy ones (white potato, sweet potato, plantain, winter squash). Notable: white potatoes were excluded from the original Whole30 but were added back in 2014.
- Fruit: Permitted but limited in spirit. Fruit smoothies are discouraged because they bypass chewing-based satiety. Dried fruit is allowed but discouraged.
- Fats: Avocado, olives, olive oil, ghee, coconut oil, coconut milk (full-fat, no carrageenan), nut and seed butters (no added sugar), animal fats from approved sources.
- Nuts and seeds: Allowed but considered a "minor characters" category — the program advises against making them a meal centerpiece. Peanuts are excluded as legumes.
Excluded categories with rationale:
- Grains: The Paleo/Whole30 argument is that grain proteins (gluten, gliadin, lectins) can drive low-grade inflammation in susceptible individuals. The evidence for this in non-celiac populations is mixed; the elimination is a diagnostic intervention more than a confirmed therapeutic one.
- Legumes: Excluded for the lectin/phytate content and because most processed legume products (especially soy) are heavily refined. The exclusion of green beans and snap peas was a frequently-asked-about edge case — they were added to the allowed list in 2014.
- Dairy: The most common single trigger food the elimination identifies. Lactose intolerance, casein sensitivity, and whey allergy are all common and largely undiagnosed.
- Added sugar and sweeteners: The most behaviorally consequential rule. Most processed and packaged foods contain sugar in some form — reading labels for the 30 days reveals just how pervasive it is.
- Alcohol: Removed for the metabolic effects, the empty calories, and because alcohol-consumption decisions tend to drag along food-quality compromises.
- Industrial seed oils: Canola, soybean, sunflower, safflower, corn, cottonseed, grapeseed oil. The argument is the high omega-6 content, the heat-and-deodorization processing, and the formation of oxidation products.
Why 30 Days — The Physiologic Rationale
The 30-day duration is a compromise between two competing constraints. Long enough that most acute inflammatory and gut-mediated symptoms have time to settle. Short enough that participants can commit to it without it becoming a permanent lifestyle change. The Hartwigs argue that:
- Gut epithelial turnover is approximately 3-5 days for the enterocytes lining the small intestine. After 30 days, the entire intestinal epithelium has turned over multiple times in the absence of any potentially-irritating dietary inputs.
- Inflammatory cytokine clearance from chronic dietary triggers happens over weeks to months. 30 days is enough to see meaningful improvement in inflammation-driven symptoms (joint pain, skin conditions, brain fog) in most responders.
- Habit formation and taste recalibration — the often-cited "21 days to form a habit" figure is mostly folklore (the actual research average is closer to 66 days), but 30 days is enough for most people to recalibrate sugar tolerance and develop new cooking and shopping patterns.
- Insulin sensitivity — even modest improvements in insulin sensitivity from carbohydrate-quality changes can be measured within 1-2 weeks; 30 days is well within the window for meaningful HOMA-IR improvement in insulin-resistant participants.
The 30-day figure is also a marketing-friendly round number — a calendar month is psychologically discrete and concrete. This is not a trivial consideration; adherence is the rate-limiting step of any dietary intervention.
What Typically Improves on Whole30
The reported benefits of completed Whole30 cycles fall into several clusters. The community-reported (and modestly-research-supported) effects include:
- Gastrointestinal symptom relief: Bloating, irregular bowel habits, post-meal discomfort, and reflux often improve substantially. For patients whose IBS is FODMAP-driven, Whole30 is partially overlapping with Low FODMAP (grains and legumes are major FODMAP sources), which may explain part of the effect — though Whole30 still includes onions and garlic, two of the worst FODMAP offenders.
- Skin clearing: Acne, rosacea, eczema, and psoriasis often respond. Dairy elimination alone is a well-documented acne trigger removal; the inflammatory effects of seed oils and refined sugars on skin are less well-characterized but consistent with experience.
- Sleep quality: Self-reported improvements in sleep duration, depth, and morning energy are common. Removal of alcohol (a well-documented REM-sleep disruptor) is the most likely single mechanism.
- Energy stability: The "afternoon crash" pattern often resolves, attributable to better glycemic control from removed refined carbohydrates and added sugars.
- Reduced food cravings: Sugar cravings in particular often diminish substantially by week 2-3. This is a behavioral as much as a metabolic change.
- Joint and muscle pain reduction: Inflammatory arthritis symptoms often improve; the mechanism likely involves the removed inflammatory dietary triggers (gluten in susceptible individuals, certain dairy proteins, refined sugar).
- Weight loss as side effect: Despite the "no scale" rule, most participants who finish a Whole30 cycle lose 5-15 pounds. The mechanism is almost entirely caloric — the food rules dramatically reduce caloric density and increase satiety, so participants spontaneously eat less.
- Mood and brain fog: Improvements in mental clarity and mood stability are commonly reported. The mechanisms are speculative (stable glycemic control, reduced inflammation, removed potentially-sensitive foods) but the pattern is consistent.
The peer-reviewed evidence base specifically for Whole30 is thin — the program has not been the subject of large randomized controlled trials. Most evidence is extrapolated from research on Paleolithic-style eating patterns more broadly (Frassetto 2009, Lindeberg 2007, Manheimer 2015 meta-analysis), which consistently show favorable effects on metabolic syndrome markers, glycemic control, and inflammation in short-term trials.
The Formal 10-Day Reintroduction (Often Skipped)
The single most under-utilized feature of the official Whole30 program is the post-30-day reintroduction protocol. The published Hartwig protocol calls for a "Fast Track Reintroduction" or a "Slow Roll Reintroduction" after the initial 30 days, but in practice most participants either (a) end the program and immediately resume eating everything, losing all diagnostic value, or (b) extend the elimination indefinitely, which is not what the program was designed for.
The formal Fast Track Reintroduction:
- Day 31: Reintroduce legumes (peanuts, soy, beans) at one meal. Continue otherwise-Whole30 for days 32-33. Track symptoms.
- Day 34: Reintroduce non-gluten grains (rice, corn, quinoa, oats). Track symptoms days 34-36.
- Day 37: Reintroduce dairy (start with butter and cheese, then yogurt, then milk). Track symptoms days 37-39.
- Day 40: Reintroduce gluten-containing grains (wheat-based bread, pasta, cereal). Track symptoms days 40-42.
The slow-roll variant spaces the reintroductions over weeks or months, with the participant returning to baseline Whole30 between each challenge. This is closer to the methodology used in clinical elimination diets and generally produces more reliable diagnostic information at the cost of taking longer.
Critical guidance often missed: a reintroduction "challenge" means actually eating a meaningful quantity of the food (a full serving of pasta, a normal portion of cheese), not a polite bite. Half-measures produce ambiguous results. See our Reintroduction Phase deep dive for a more thorough treatment of challenge methodology, symptom-tracking, and the common interpretation errors.
Who Benefits Most — and Who Should Not Try It
Likely to benefit:
- Adults with non-specific GI complaints (bloating, irregular bowel habits, post-meal discomfort) without an established diagnosis
- Adults with adult-onset acne, rosacea, or unexplained eczema flares
- Adults with chronic low-energy patterns who suspect dietary contributors
- Adults with inflammatory joint symptoms (early rheumatoid arthritis, undiagnosed seronegative arthropathy)
- Adults using Whole30 as a structured break from problem eating patterns (binge cycles, alcohol overuse, sugar dependence)
- Adults whose habitual diet is heavy in processed food and who want a structured reset to whole-food eating
Should approach with caution or avoid:
- History of eating disorder: The rigid rules, "no slip allowed" framing, and elaborate food categorization can be triggering for participants with anorexia, bulimia, or orthorexia. Whole30 is contraindicated in active disordered eating.
- Pregnancy and breastfeeding: Not a contraindication per se, but caloric requirements rise substantially and dietary restriction can be problematic. If undertaking Whole30 in this setting, coordinate with an obstetric provider and ensure adequate calorie and micronutrient intake.
- Type 1 diabetes: Insulin requirements can change rapidly with significant carbohydrate reduction. Should be undertaken only with close endocrinology supervision and frequent glucose monitoring.
- Already-restrictive eating patterns: A participant who already follows a vegetarian, vegan, or kosher diet may find that additional restriction leaves an inadequate food repertoire. Vegetarian Whole30 is theoretically possible but exceptionally difficult given the legume exclusion.
- Active gout flare: A heavy-meat Whole30 can substantially increase purine load and trigger flares in patients with gout.
- Chronic kidney disease: The high protein load may not be appropriate in CKD stages 3-5.
For patients with established gastrointestinal diagnoses, more specific protocols may outperform Whole30. See our Low FODMAP page for IBS specifically, and our Carnivore Reset page for refractory autoimmune cases where milder eliminations have failed.
Common Pitfalls and Failure Modes
- Skipping reintroduction — the single most common failure. The participant "completes" 30 days, feels great, then either resumes everything immediately (losing diagnostic value) or continues indefinitely (turning a 30-day diagnostic into permanent restriction).
- Inadequate carbohydrate intake — especially common in active women. Whole30 is not inherently low-carb (potatoes, sweet potatoes, plantains, fruit are all allowed and encouraged), but many participants default toward very-low-carb eating, which can produce poor exercise tolerance, sleep disruption, and menstrual irregularity. Eat starchy vegetables daily.
- Inadequate fat intake — with grains, dairy, and most processed foods removed, fat becomes the primary energy source. Participants who unconsciously try to be "low fat" on Whole30 end up under-fueled. Include a meaningful fat source (avocado, olives, nuts, ghee, coconut oil) at each meal.
- Hidden sugar and seed oils — broth, deli meats, condiments, salad dressings, and sausages frequently contain sugar or non-compliant oils. The program's strict reading-of-labels practice is part of its educational value.
- The "30 days isn't long enough" trap — some participants experience initial worsening before improvement and conclude the program failed when in fact they did not give it long enough. For skin and autoimmune conditions, 60-90 days is sometimes needed. Most healthy participants will see meaningful improvement by day 14-21.
- Over-rigid social interpretation — declining a friend's homemade birthday dish to maintain Whole30 strict-letter compliance can damage relationships. The program founders explicitly support graceful exit strategies. The goal is information, not perfection.
- The "Tiger Blood" plateau — the Hartwigs' marketing-speak for the high-energy phase around day 16-25. Some participants never get there, which can be discouraging. The phase is not universal — absence of Tiger Blood does not mean the program is not working.
Whole30 vs Paleo vs AIP — Where It Sits
Whole30 sits in the middle of a spectrum of related elimination protocols, each with different scope:
- Paleo (broadest): Eliminates grains, legumes, dairy, refined sugar, and processed foods. Permits natural sweeteners (honey, maple syrup), occasional alcohol, and "Paleo treats" (almond-flour baked goods, etc.). Designed as a long-term eating pattern, not a structured elimination.
- Whole30 (middle): Tighter than Paleo on sweeteners (none allowed), alcohol (none), and Paleo recreations (none). 30-day duration with formal reintroduction. Structured as an n-of-1 diagnostic experiment.
- Autoimmune Protocol (AIP, tightest): Whole30 rules plus elimination of nightshades (tomato, potato, pepper, eggplant), eggs, nuts, seeds (including coffee), and most spices. Designed specifically for autoimmune disease (Hashimoto's, rheumatoid arthritis, lupus, multiple sclerosis, inflammatory bowel disease). Several small published studies suggest meaningful benefit in IBD (Konijeti 2017 PMID 28858071, Chandrasekaran 2019 PMID 31579890). Typically run for 4-12 weeks before reintroduction.
A patient unsure where to start typically does best with Whole30 first — it captures most of the diagnostic value with the least restriction. If symptoms partially improve but do not fully resolve, stepping down to AIP is the logical next move. Skipping straight to AIP or carnivore is reserved for severe presentations that have already failed milder eliminations.
Practical Meal Planning
The most consistent practical advice from Whole30 veterans is to plan and prep before day 1. A typical sustainable structure:
- Breakfast: 3-4 eggs cooked in ghee, half an avocado, sauteed greens (spinach, kale, or chard). Optional: a side of compliant breakfast sausage. Coffee black or with coconut milk.
- Lunch: Large salad with mixed greens, 4-6 ounces of protein (leftover chicken, salmon, tuna, or hard-boiled eggs), generous fat (olives, avocado, nuts), olive-oil-and-vinegar dressing. Or a "bowl" build with sweet potato base, protein, sauteed vegetables, and tahini drizzle.
- Dinner: 6-8 ounces of protein (steak, roast chicken, pork chop, salmon), one to two starchy vegetables (roasted potato, sweet potato, winter squash, plantain), one to two non-starchy vegetables (broccoli, brussels sprouts, asparagus, cauliflower). Fat source built into the cooking method.
- Snacks (optional, discouraged in spirit): Apple with almond butter. Hard-boiled eggs. Olives. Cucumber slices with guacamole. A handful of nuts. Compliant beef jerky.
Batch-cooking on a weekend is essential. A typical Sunday: roast a tray of chicken thighs, hard-boil a dozen eggs, roast two trays of mixed vegetables, prep a large container of salad greens, make a batch of compliant mayo or dressing, slice avocados or peppers for the week. This 90-minute investment prevents the day-3 collapse into "there's nothing I can eat" overwhelm.
Eating out on Whole30 is possible but requires confident substitution requests — "no rice, no beans, no cheese, no tortilla, no sauce on the side — just the meat, the guacamole, and the salad with oil and vinegar" is a manageable order at most restaurants. The Whole30 community maintains crowd-sourced lists of compliant menu options at major chains.
Key Research Papers
- Konijeti GG et al. (2017). Efficacy of the Autoimmune Protocol Diet for Inflammatory Bowel Disease. Inflammatory Bowel Diseases. — PubMed: PMID 28858071
- Chandrasekaran A et al. (2019). The Autoimmune Protocol Diet Modifies Intestinal RNA Expression in Inflammatory Bowel Disease. Crohn's & Colitis 360. — Search PubMed
- Manheimer EW et al. (2015). Paleolithic nutrition for metabolic syndrome: systematic review and meta-analysis. American Journal of Clinical Nutrition. — Search PubMed
- Frassetto LA et al. (2009). Metabolic and physiologic improvements from consuming a paleolithic, hunter-gatherer type diet. European Journal of Clinical Nutrition. — PubMed: PMID 19209185
- Lindeberg S et al. (2007). A Palaeolithic diet improves glucose tolerance more than a Mediterranean-like diet in individuals with ischaemic heart disease. Diabetologia. — PubMed: PMID 17583796
- Jonsson T et al. (2010). A Paleolithic diet is more satiating per calorie than a Mediterranean-like diet in individuals with ischemic heart disease. Nutrition & Metabolism. — PubMed: PMID 21118562
- Boers I et al. (2014). Favourable effects of consuming a Palaeolithic-type diet on characteristics of the metabolic syndrome. Lipids in Health and Disease. — PubMed: PMID 25304296
- Mellberg C et al. (2014). Long-term effects of a Palaeolithic-type diet in obese postmenopausal women. European Journal of Clinical Nutrition. — PubMed: PMID 24473459
- Otten J et al. (2017). A heterogeneous response of liver and skeletal muscle fat to the combination of a Paleolithic diet and exercise in obese individuals with type 2 diabetes. Diabetologia. — Search PubMed
- Konner M, Eaton SB. (2010). Paleolithic nutrition: twenty-five years later. Nutrition in Clinical Practice. — Search PubMed
- Whalen KA et al. (2016). Paleolithic and Mediterranean Diet Pattern Scores Are Inversely Associated with Biomarkers of Inflammation and Oxidative Balance in Adults. The Journal of Nutrition. — PubMed: PMID 27099230
- Genoni A et al. (2020). A Paleolithic diet lowers resistant starch intake but does not affect serum trimethylamine-N-oxide concentrations in healthy women. British Journal of Nutrition. — Search PubMed
PubMed Topic Searches
- PubMed: Paleolithic diet and metabolic syndrome
- PubMed: AIP diet for IBD
- PubMed: 30-day elimination diet
- PubMed: Whole30 nutrition intervention
- PubMed: Paleo diet inflammation biomarkers
Connections
- Elimination Diet (Main Hub)
- Benefits Deep-Dive Hub
- Low FODMAP
- Carnivore Reset
- Reintroduction Phase
- All Remedies
- Food
- IBS
- Acne
- Eczema
- Insulin Resistance
- Rheumatoid Arthritis
- Immune Boosting
- Vitamin D3