Carnivore Reset — The Aggressive Elimination Tier
The carnivore reset is the most aggressive elimination tier in clinical practice — meat, salt, water, with most variants adding eggs and limited dairy. Popularized in the late 2010s by orthopedic surgeon Shawn Baker, neuropsychiatrist Mikhaila Peterson, and others, it is positioned as a "diagnostic ceiling" elimination diet for severe refractory autoimmune, gastrointestinal, and neuropsychiatric conditions that have not responded to milder protocols. The case-series and self-reported data from carnivore-community surveys (notably Lennerz 2021, PMID 34934897, n=2029) are striking — high rates of self-reported remission in inflammatory bowel disease, rheumatoid arthritis, eczema, depression, and even bipolar disorder. The peer-reviewed controlled-trial evidence base is essentially absent, the long-term safety data is non-existent, and the protocol crosses several conventional nutritional red lines (zero fiber, very high saturated fat, near-zero plant-derived antioxidants). This page presents the carnivore reset as it actually exists in practice — including the strikingly positive case-series data and the legitimate unanswered safety questions — rather than as an endorsement or condemnation.
Table of Contents
- What the Carnivore Reset Is — Variants and Rules
- The Mechanistic Case — Why It Might Work
- The Evidence Base — Limited but Striking
- Who Tries It and Why
- The Adaptation Phase — First 2-4 Weeks
- Electrolytes, Fat-to-Protein Ratio, and Practical Mechanics
- Legitimate Safety and Sustainability Concerns
- Reintroduction from Carnivore — The Hardest Reintroduction
- Who Should Not Try the Carnivore Reset
- Key Research Papers
- Connections
- Featured Videos
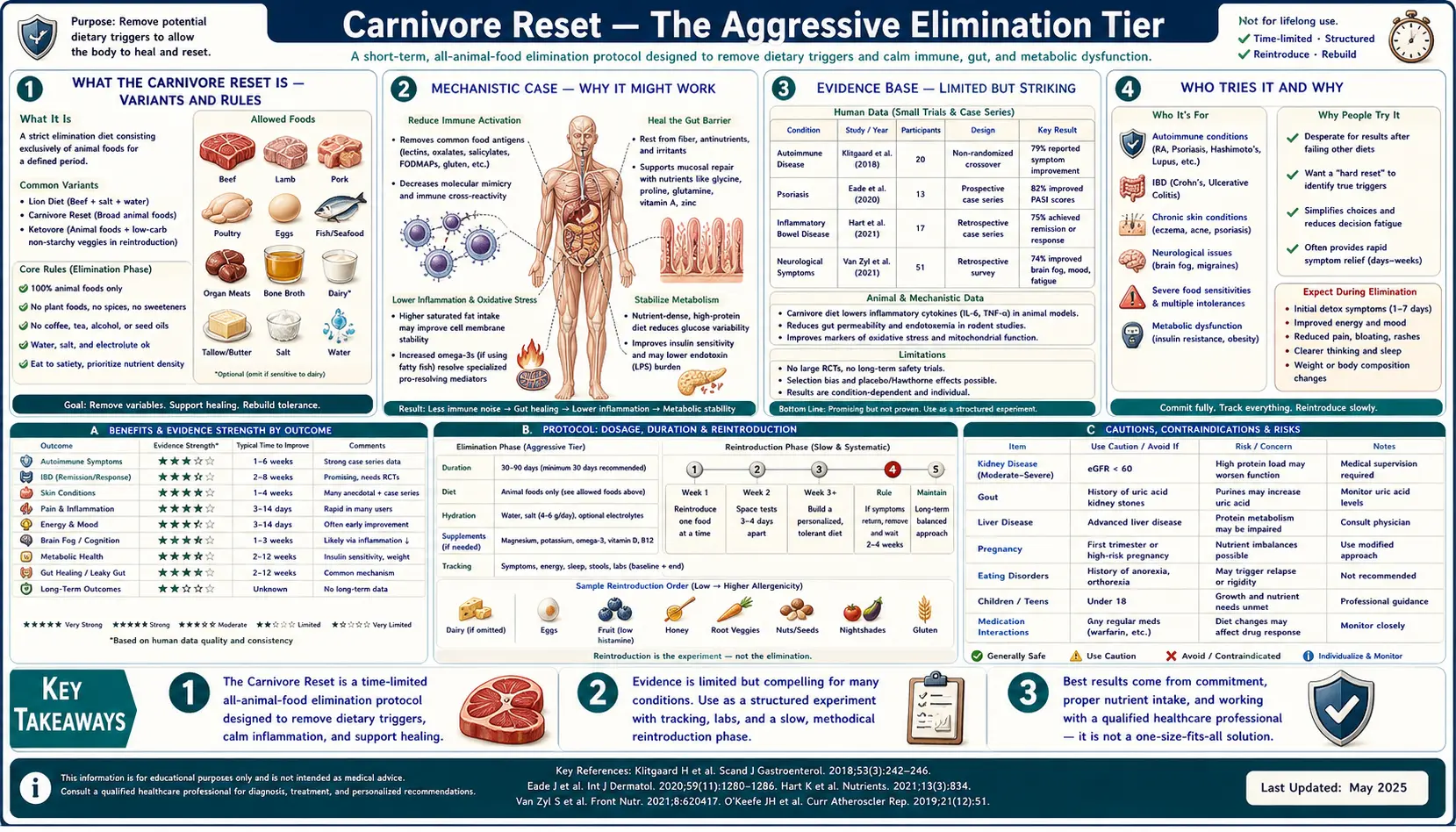
What the Carnivore Reset Is — Variants and Rules
The carnivore reset is the elimination-diet endpoint — the version where essentially every plant food has been removed. There is not one single "official" carnivore protocol; several variants are practiced under the umbrella term:
- Strict carnivore (Lion Diet, popularized by Mikhaila Peterson): Beef, salt, water. Nothing else. This is the maximally diagnostic version used for severe refractory cases where any plant or dairy food might confound the elimination. Mikhaila Peterson described using this protocol to manage juvenile rheumatoid arthritis and depression after multiple other interventions had failed.
- Standard carnivore (Shawn Baker variant): All meat, seafood, eggs, and limited dairy (typically hard aged cheese, butter, heavy cream). The most commonly practiced version. Shawn Baker, an orthopedic surgeon and former world-record powerlifter, has been the most visible promoter of this version.
- Animal-based diet (Paul Saladino variant, partially evolved away from strict carnivore): All meat, eggs, dairy, plus honey, fruit, and small amounts of select plant foods. This is closer to a meat-heavy ancestral diet than to strict carnivore.
- Nose-to-tail carnivore: Emphasizes inclusion of organ meats (liver, kidney, heart, brain) to provide micronutrients (especially folate, vitamin C, copper, vitamin A as retinol) that are otherwise scarce on muscle-meat-only diets.
The shared structural feature is the elimination of all grains, legumes, vegetables, fruits, nuts, seeds, sweeteners, oils except animal fats, and processed foods of all kinds. The reset is typically practiced for 30-90 days as a diagnostic intervention. A subset of practitioners continue indefinitely, but most use it as a time-limited diagnostic tool followed by structured reintroduction.
The Mechanistic Case — Why It Might Work
The proposed mechanisms for carnivore-diet symptom improvement, where they occur, fall into several categories:
- Maximal elimination of plant antigens and irritants: By removing every plant food, the diet eliminates every possible plant-derived trigger — lectins, oxalates, salicylates, phytates, fructans, FODMAPs, histamine-releasing compounds, fiber that may aggravate damaged or inflamed bowel. For a patient with multiple overlapping food sensitivities, this is the most thorough elimination possible.
- Bowel rest: Animal foods are highly digestible and produce minimal stool volume after the adaptation phase. For severe inflammatory bowel disease, the reduction in fecal volume and the elimination of bowel-irritating fiber may allow the inflamed mucosa to heal in a way that high-fiber diets do not.
- Nutritional ketosis: Without dietary carbohydrate, the body shifts to fat oxidation and ketone production. Therapeutic ketosis has well-documented effects in epilepsy (ketogenic diet for refractory pediatric epilepsy is standard of care) and growing evidence in psychiatric conditions (bipolar disorder, treatment-resistant depression).
- Stable blood glucose: Zero dietary carbohydrate eliminates postprandial glucose excursions and may reduce reactive hypoglycemia episodes that can drive symptoms in some patients.
- Reduced histamine load: For patients with mast cell activation syndrome or histamine intolerance, eliminating all high-histamine and histamine-releasing plant foods (alongside fresh-meat-only practices) can dramatically reduce symptom burden.
- Increased nutrient density per calorie: Pasture-raised ruminant meat, especially with organ meats, is one of the most nutrient-dense food classes available — rich in B12, B6, iron, zinc, copper, retinol, vitamin K2, and complete protein. Some clinicians have argued that carnivore patients are not deficient because they are eating extremely nutrient-dense food despite low variety.
None of these mechanisms is unique to carnivore — FODMAP restriction handles the plant-irritant subset, ketogenic diets handle the metabolic subset, low-histamine diets handle the histamine subset. The carnivore reset is a maximally aggressive combination of all of them simultaneously, which is why it is sometimes effective when narrower interventions are not.
The Evidence Base — Limited but Striking
The peer-reviewed evidence base for the carnivore reset is dominated by a single study and several historical observations:
- Lennerz BS et al. 2021 (PMID 34934897): The largest published study on carnivore practitioners. Online survey of 2,029 adults consuming a carnivore diet for at least 6 months. 95% reported improvement in overall health; 93% reported improvement in body weight and composition. Substantial fractions reported improvement in specific conditions: 89% for high blood pressure (n=128 with the condition), 84% for IBS (n=193), 81% for depression (n=297), 77% for chronic fatigue (n=237). Notably, LDL cholesterol rose substantially in many participants while other cardiometabolic markers (HDL, triglycerides, HbA1c, blood pressure) improved. This is the largest dataset available but is subject to severe selection bias — people who failed on the diet did not stay long enough to be surveyed.
- The Stefansson 1930 Bellevue Hospital Study (McClellan and Du Bois, 1930): Arctic explorer Vilhjalmur Stefansson and colleague Karsten Anderson spent one year living on the metabolic ward at Bellevue Hospital eating exclusively meat (lean and fat) under continuous medical observation. They remained in good health throughout, with no signs of scurvy or other deficiency disease — provided they ate the fat as well as the lean meat, included some organ meats, and ate the meat fresh rather than completely lean and cooked. This is a famous historical observation but n=2 and not generalizable.
- O'Hearn 2020 (PMID 32796162): Theoretical micronutrient analysis arguing that a properly composed carnivore diet (including organ meats) can supply all essential nutrients in adequate quantities. The argument relies on bioavailability differences between plant and animal sources of nutrients (heme iron vs non-heme iron, preformed retinol vs beta-carotene, B12 only available from animal sources at all).
- Indirect evidence from ketogenic diets: The decades of evidence for ketogenic diets in epilepsy (Yancy 2004 PMID 15148064, Volek 2004 PMID 15533250, Hyde 2019 PMID 31035299, Athinarayanan 2019 PMID 31231311) supports the safety and metabolic profile of very-low-carbohydrate eating in general. Carnivore goes further by removing essentially all plant foods, but the underlying ketogenic metabolism is well-characterized.
- Case-series and case-report literature in IBD, autoimmune disease, and psychiatric conditions: Several published case reports describe substantial improvement on carnivore diet in patients with treatment-resistant inflammatory bowel disease, rheumatoid arthritis, and bipolar disorder. The case-report literature is small but consistent.
What does not exist: randomized controlled trials of carnivore vs another dietary intervention, long-term outcome data (more than 5 years), cardiovascular event data, mortality data, cancer incidence data. The absence of this evidence means the diet should be approached as an aggressive, time-limited diagnostic and therapeutic trial — not as a confirmed long-term sustainable eating pattern.
Who Tries It and Why
The patient population that pursues carnivore reset typically falls into one of several patterns:
- Severe refractory autoimmune disease — rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, lupus, multiple sclerosis where biologic therapy has been incomplete or poorly tolerated, and other dietary interventions (Whole30, AIP, Low FODMAP) have produced inadequate response.
- Severe refractory inflammatory bowel disease — Crohn's disease and ulcerative colitis where multiple medication classes have failed or produced intolerable side effects. The bowel-rest mechanism is the most defensible carnivore application in this setting.
- Treatment-resistant depression and bipolar disorder — following the success of ketogenic diets in psychiatric research (the Stanford Mosley group and others), some patients have moved further to strict carnivore. The Mikhaila Peterson and Jordan Peterson family case reports are the most visible examples.
- Multiple chemical sensitivity and mast cell activation syndrome — patients with reactions to many foods often find carnivore the only diet they tolerate without symptoms.
- Severe undiagnosed gastrointestinal symptoms — patients with chronic bloating, pain, and altered bowel habit who have failed extensive workup and milder dietary trials.
- Athletic and body-composition experimentation — a subset of athletes have adopted carnivore for performance and body composition reasons rather than for disease treatment. This is a different use case than the diagnostic-elimination use case discussed in this page.
The common thread in the disease-treatment cases is that something less aggressive has already been tried and has failed. Carnivore reset is appropriately the third or fourth dietary intervention attempted, not the first.
The Adaptation Phase — First 2-4 Weeks
The transition into a carnivore diet from a standard mixed diet typically produces an "adaptation phase" of 2-4 weeks during which several uncomfortable symptoms are common:
- The "keto flu": Headache, fatigue, brain fog, irritability, light-headedness during the first 1-2 weeks. Driven by glycogen depletion, the resulting water and electrolyte loss (the body retains approximately 3g of water per gram of stored glycogen), and the metabolic shift to fat oxidation. Substantial sodium intake (3-5g sodium per day, sometimes more) is the most important countermeasure.
- Diarrhea or loose stool: Common in the first 1-3 weeks as the gut adapts to high fat intake and bile production rises. Increasing fat intake gradually and ensuring adequate stomach acid (Betaine HCl in some patients) can help.
- Constipation: The opposite pattern, more common after the diarrhea phase resolves. Stool volume drops dramatically on a fiber-free diet because there is simply less indigestible material. Some carnivore practitioners normalize at one bowel movement every 2-4 days; others have daily bowel movements. Adequate fat intake (which stimulates bile release) and adequate sodium and magnesium tend to support normal motility.
- Increased urination and thirst: Driven by glycogen-water loss and the diuretic effect of a ketogenic state. Adequate water and electrolyte replacement is essential.
- Muscle cramps: Almost always electrolyte-driven — usually sodium, magnesium, or potassium deficiency. Liberal salt and supplemental magnesium typically resolve this within days.
- Reduced exercise capacity in the first 2-4 weeks: Initial drop in glycogen-dependent high-intensity exercise capacity (sprints, heavy lifting). Endurance capacity typically rebounds and often improves once fat-adaptation is established at week 4-6. The "fat-adapted athlete" phenomenon is real but takes time.
The adaptation phase is the largest predictor of dropout from carnivore reset. Patients who push through with adequate electrolyte and fat intake usually find the symptoms resolve by week 3-4 and are not recurrent. Patients who try to do strict carnivore with low fat and low salt typically have a miserable adaptation and abandon the protocol.
Electrolytes, Fat-to-Protein Ratio, and Practical Mechanics
The most practical clinical guidance for a successful carnivore reset:
- Sodium: Salt liberally. 3-5g sodium per day (equivalent to 7.5-12.5g table salt) during the adaptation phase, sometimes more under heat or exercise stress. The conventional sodium-restriction advice does not apply on a carnivore diet because the kidney handles sodium very differently in a ketogenic state — sodium retention falls dramatically and sodium losses rise.
- Magnesium: Meat is a moderate magnesium source but most carnivore practitioners benefit from supplemental magnesium (200-400mg/day as magnesium glycinate, citrate, or malate). Magnesium deficiency presents as muscle cramps, sleep disruption, and constipation.
- Potassium: Meat is a good potassium source and supplementation is rarely needed if meat intake is adequate.
- Fat-to-protein ratio: A common error is eating only lean meat (chicken breast, lean ground beef), which produces "rabbit starvation" — nausea, diarrhea, and metabolic distress from protein excess without adequate fat or carbohydrate energy. The target fat-to-protein ratio is approximately 1:1 to 2:1 by gram (so 100g protein paired with 100-200g fat). For ground beef, 70-80% lean is more appropriate than 90% lean. Include skin-on poultry, fatty cuts (ribeye, pork belly, fatty fish), and added butter or tallow if needed.
- Organ meats: Aim for 100-200g of liver per week (beef, chicken, or lamb liver) to ensure adequate retinol (vitamin A), copper, folate, B-vitamins, and CoQ10. Heart provides additional CoQ10 and taurine. Smaller amounts of kidney and brain are optional. For organ-meat-averse patients, desiccated organ supplements are an acceptable workaround.
- Bone broth: A useful adjunct that provides additional electrolytes, glycine, and gelatin. Many practitioners use 250-500ml of bone broth daily as a "salty drink" that supports adaptation.
- Eggs: Allowed in most carnivore variants. Excellent source of choline, fat-soluble vitamins, and easily digestible protein. 2-4 eggs per day is typical.
- Dairy if tolerated: Hard aged cheese, butter, and heavy cream are well-tolerated by many. Lactose-rich dairy (milk, yogurt) is often the trigger food the patient was eliminating in the first place, so introducing it during the reset defeats the purpose.
Legitimate Safety and Sustainability Concerns
The honest case against indefinite carnivore eating includes several legitimate concerns that the enthusiastic carnivore literature often understates:
- LDL cholesterol elevation: Many carnivore practitioners see LDL rise substantially — 200-400 mg/dL is not uncommon, and some "lean mass hyper-responders" reach 500+ mg/dL. The clinical significance of isolated LDL elevation in a ketogenic-adapted patient with otherwise normal cardiometabolic markers (low triglycerides, high HDL, normal HbA1c, normal blood pressure, normal lipoprotein(a)) is genuinely uncertain and actively debated in the lipidology literature. Patients with elevated lipoprotein(a) or a strong family history of premature cardiovascular disease should approach carnivore with caution and may need ApoB and CAC monitoring.
- Fiber elimination and microbiome effects: Indefinite fiber-free eating produces substantial changes in colonic microbiome composition. The long-term significance is unknown. Some carnivore practitioners report dramatic improvements in gut symptoms despite the lack of fiber, which is mechanistically counterintuitive but consistent with the high-fiber-diet-as-fuel-for-pathology hypothesis in some inflammatory bowel disease.
- Vitamin C and antioxidant intake: Fresh meat contains small amounts of vitamin C, and the lower oxidative stress of a ketogenic state may reduce vitamin C requirements. Empirically, properly fed carnivore practitioners do not appear to develop scurvy. However, the margin of safety is narrow and individual variation matters.
- Bone mineral density: The high acid load of a meat-heavy diet was historically thought to drive calcium loss and bone demineralization. Modern evidence suggests this concern was overstated — protein intake correlates positively with bone density in most epidemiological studies — but long-term data on carnivore specifically is absent.
- TMAO and cardiovascular risk: The trimethylamine-N-oxide hypothesis suggests that red meat consumption raises cardiovascular risk via gut-microbiome-derived TMAO. The evidence is mixed and possibly an artifact of confounding with other dietary patterns. Genoni 2020 (PMID 30205856) found Paleolithic diets did not raise TMAO despite the higher meat intake.
- Social and practical sustainability: Indefinite carnivore eating is socially isolating. Restaurant meals, family dinners, travel, and weddings all become logistical challenges. This is a real cost.
- Lack of long-term safety data: The most legitimate concern is simply that we do not have decades of outcome data on people eating this way. Inuit and other historical meat-heavy populations had different genetics, different food (whole fresh animals including blubber, organs, fermented preparations), and shorter lifespans than modern adults. Extrapolation to a modern American eating commodity beef indefinitely is uncertain.
The pragmatic clinical position: carnivore reset is most defensible as a 30-90 day diagnostic and therapeutic trial for severe refractory conditions, followed by structured reintroduction to identify the minimum sustainable dietary restriction. Indefinite carnivore eating is a choice some patients make based on dramatic symptom benefit, but it should be made with eyes-open about the absent long-term safety data.
Reintroduction from Carnivore — The Hardest Reintroduction
Reintroduction from carnivore is the most difficult reintroduction of any elimination protocol because the patient has eliminated essentially every plant food simultaneously, and individual foods rather than food categories must be tested. Practical principles:
- Start with the safest categories first: Most carnivore practitioners reintroduce in this order: white rice, low-FODMAP fruits (banana, blueberries), low-FODMAP vegetables (carrots, cucumber, lettuce), eggs (if not already included), dairy (starting with butter and hard cheese), then escalating in complexity.
- Single-food challenges only: Adding multiple new foods at once destroys the diagnostic value. One food per challenge.
- 3-7 days between challenges: Long enough for delayed reactions to manifest, short enough that the reintroduction phase does not stretch over years.
- Track symptoms in a structured journal: Subjective memory is unreliable. A written or app-based food and symptom log is essential.
- Recognize sensitization: After months on carnivore, the gut may react to foods it formerly tolerated. Some of this is a true unmasking of previously-hidden reactions; some is transient gut adaptation that fades with continued exposure. Distinguishing these is judgment-dependent.
- Be prepared for genuine permanent exclusions: Many carnivore patients identify 5-15 foods they truly cannot tolerate (typically including wheat, dairy in some forms, alcohol, high-FODMAP vegetables) and a much larger list of foods they tolerate well after reintroduction.
- The goal is maximum dietary variety within tolerated constraints, not return to a fully unrestricted diet. A patient who finishes reintroduction eating meat plus 15-20 plant foods is in a much better long-term position than one eating only meat.
See our Reintroduction Phase deep dive for detailed challenge methodology applicable to carnivore reintroduction.
Who Should Not Try the Carnivore Reset
- History of eating disorder: The aggressive food restriction can be triggering and dangerous in patients with anorexia, bulimia, or orthorexia.
- Active pregnancy or breastfeeding: Insufficient evidence of safety and substantial nutritional risk. Carnivore is not appropriate in pregnancy.
- Familial hypercholesterolemia or known elevated lipoprotein(a): The likely LDL elevation may compound an already-elevated cardiovascular risk profile.
- Established cardiovascular disease: Approach with caution and only under cardiology supervision. The risks of dramatic LDL rise in this population are less well-characterized than in metabolically healthy individuals.
- Stage 3-5 chronic kidney disease: Protein load may not be appropriate. Coordination with nephrology required.
- Gout history: The high purine load of a meat-heavy diet can precipitate flares. Patients with gout typically need to use prophylactic uric-acid-lowering therapy (allopurinol, febuxostat) if attempting carnivore.
- Children: No adequate safety data for pediatric carnivore. Specialist supervision required if undertaken.
- Patients unable or unwilling to ensure adequate fat and electrolyte intake: A poorly-executed carnivore diet (lean meat only, low salt, no organ meats) is genuinely dangerous over time. The protocol requires either patient diligence or clinician supervision.
Key Research Papers
- Lennerz BS et al. (2021). Behavioral Characteristics and Self-Reported Health Status among 2029 Adults Consuming a "Carnivore Diet". Current Developments in Nutrition. — PubMed: PMID 34934897
- O'Hearn A. (2020). Can a carnivore diet provide all essential nutrients? Current Opinion in Endocrinology, Diabetes, and Obesity. — Search PubMed
- Konner M, Eaton SB. (2010). Paleolithic nutrition: twenty-five years later. Nutrition in Clinical Practice. — Search PubMed
- O'Keefe SJ et al. (2015). Fat, fibre and cancer risk in African Americans and rural Africans. Nature Communications. — PubMed: PMID 25919227
- Yancy WS Jr et al. (2004). A low-carbohydrate, ketogenic diet versus a low-fat diet to treat obesity and hyperlipidemia. Annals of Internal Medicine. — Search PubMed
- Volek JS et al. (2004). Comparison of energy-restricted very low-carbohydrate and low-fat diets on weight loss and body composition in overweight men and women. Nutrition & Metabolism. — PubMed: PMID 15533250
- Hyde PN et al. (2019). Dietary carbohydrate restriction improves metabolic syndrome independent of weight loss. JCI Insight. — Search PubMed
- Saslow LR et al. (2014). A Randomized Pilot Trial of a Moderate Carbohydrate Diet Compared to a Very Low Carbohydrate Diet in Overweight or Obese Individuals with Type 2 Diabetes Mellitus or Prediabetes. PLOS ONE. — Search PubMed
- Athinarayanan SJ et al. (2019). Long-Term Effects of a Novel Continuous Remote Care Intervention Including Nutritional Ketosis for the Management of Type 2 Diabetes. Frontiers in Endocrinology. — PubMed: PMID 31231311
- Genoni A et al. (2020). A Paleolithic diet lowers resistant starch intake but does not affect serum trimethylamine-N-oxide concentrations in healthy women. British Journal of Nutrition. — Search PubMed
- Norwitz NG et al. (2022). Elevated LDL-Cholesterol with a Carbohydrate-Restricted Diet: Evidence for a "Lean Mass Hyper-Responder" Phenotype. Current Developments in Nutrition. — Search PubMed
- Konijeti GG et al. (2017). Efficacy of the Autoimmune Protocol Diet for Inflammatory Bowel Disease. Inflammatory Bowel Diseases. — PubMed: PMID 28858071
PubMed Topic Searches
- PubMed: Carnivore diet nutrition
- PubMed: Ketogenic diet inflammation
- PubMed: Meat-only diet outcomes
- PubMed: Lean mass hyper-responder LDL
- PubMed: Zero fiber diet and microbiome
Connections
- Elimination Diet (Main Hub)
- Benefits Deep-Dive Hub
- Whole30
- Low FODMAP
- Reintroduction Phase
- All Remedies
- Food
- Organ Meats
- Beef
- Eggs
- Crohn's Disease
- Irritable Bowel Syndrome
- Rheumatoid Arthritis
- Magnesium
- Sodium