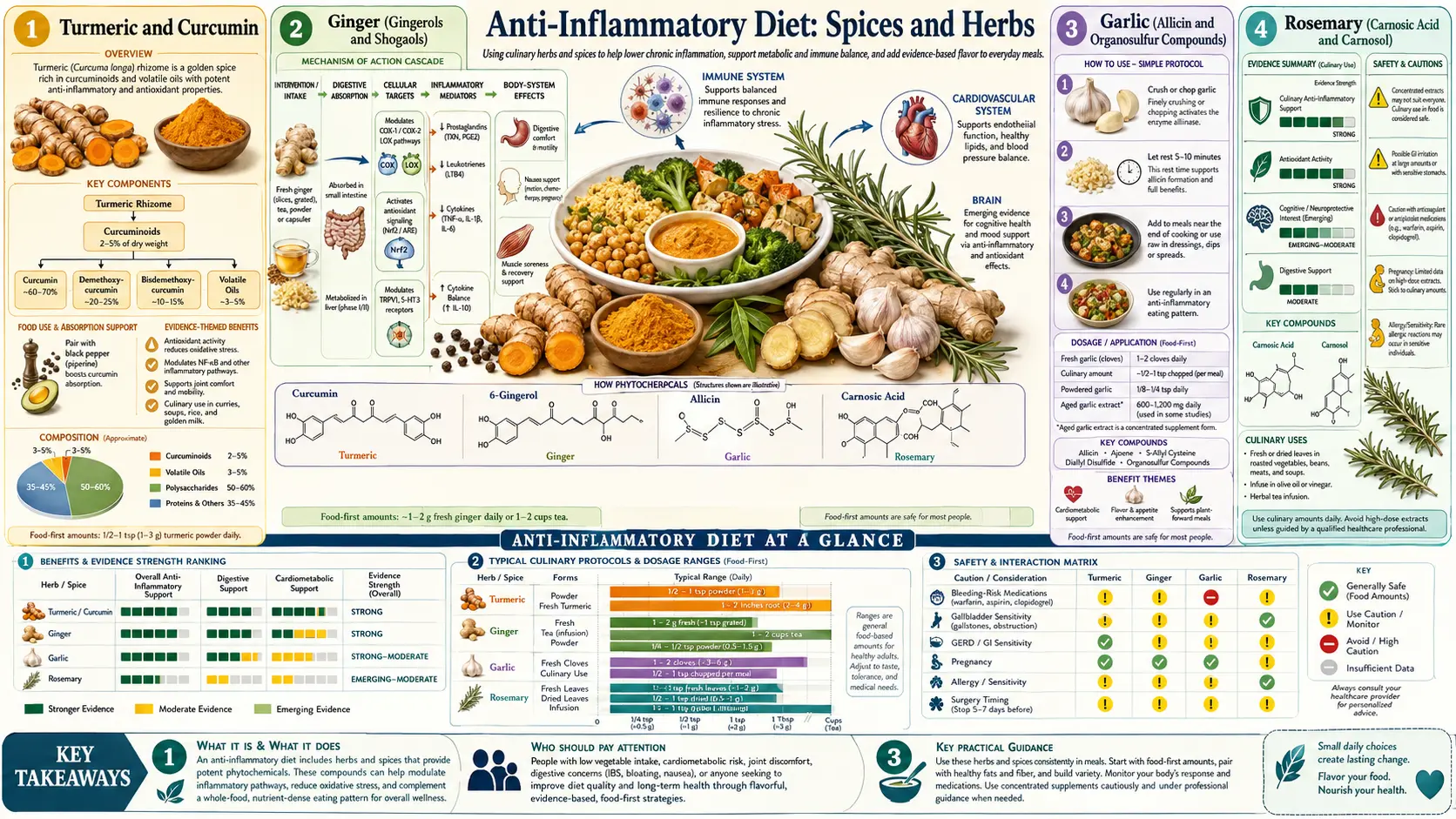
Anti-Inflammatory Diet: Spices and Herbs
Gram for gram, dried culinary spices and fresh herbs are the most concentrated source of anti-inflammatory polyphenols in the human diet. The USDA database of antioxidant capacity (ORAC) lists ground cloves at 314,000 micromol Trolox equivalents per 100 g, ground turmeric at 102,000, dried oregano at 175,000, and rosemary at 165,000 — figures 10 to 100 times the density of even the most polyphenol-rich vegetables and fruits. Eight key spice families — turmeric, ginger, garlic, rosemary, oregano, cinnamon, saffron, and clove — have moved beyond traditional kitchen use into rigorous clinical evaluation. This deep-dive maps each spice to its principal active compound, the inflammatory pathway it modulates, the trial-grade evidence for clinical effect, and the practical kitchen pairings (curcumin with piperine and fat; rosemary in EVOO; garlic crushed and rested) that translate gram-scale spice doses into bioavailable, biologically active intakes.
Table of Contents
- Turmeric and Curcumin
- Ginger (Gingerols and Shogaols)
- Garlic (Allicin and Organosulfur Compounds)
- Rosemary (Carnosic Acid and Carnosol)
- Oregano (Carvacrol and Thymol)
- Cinnamon (Cinnamaldehyde)
- Saffron (Crocin and Safranal)
- Bioavailability and Kitchen Pairings
- Key Research Papers
- Connections
- Featured Videos
Turmeric and Curcumin
Turmeric (Curcuma longa) is the dried, ground rhizome of the curcuma plant, the principal yellow pigment in Indian cuisine and the source of about 2–5% by weight of curcuminoids — curcumin, demethoxycurcumin, and bisdemethoxycurcumin. Curcumin is the most studied; it inhibits NF-kappaB translocation, COX-2 expression, 5-lipoxygenase activity, and a long list of other inflammatory mediators (IL-1, IL-6, TNF-alpha, IFN-gamma).
The Hewlings & Kalman 2017 comprehensive review in Foods summarizes the human-trial evidence: in randomized trials, supplementation with curcumin (typically 500–2,000 mg/day of a bioavailability-enhanced formulation) reduces hs-CRP, IL-6, and pain scores in osteoarthritis to a degree comparable to NSAIDs, with a far better gastrointestinal safety profile. The 2016 meta-analysis by Daily et al. of 8 randomized trials in osteoarthritis found curcumin produced pain relief and functional improvement statistically indistinguishable from ibuprofen 1,200 mg/day.
The bioavailability problem: free curcumin is poorly absorbed and rapidly conjugated by the liver. Three formulation strategies overcome this: (1) piperine pairing — 5–20 mg of black-pepper-derived piperine inhibits hepatic glucuronidation and increases curcumin absorption 20-fold (Shoba 1998 Planta Medica); (2) phospholipid complexes — Meriva and similar formulations bind curcumin to soy lecithin, increasing absorption ~30 fold; (3) nanoparticle/micelle formulations — Theracurmin, NovaSol, and similar, with 27 to 185-fold absorption improvements. The kitchen analog: ground turmeric cooked in oil with a generous grind of black pepper (the standard South Indian and Sri Lankan technique) approximates the piperine + fat absorption enhancement.
Practical dose: 1 tsp ground turmeric daily (~3 g, supplying ~100 mg curcuminoids) in cooked food is the dietary baseline. For an inflammatory condition (osteoarthritis, IBD, RA), a standardized curcumin extract at 500–1,000 mg twice daily with food is the trial-grade dose. Cautions: high-dose curcumin can interact with anticoagulants (additive antiplatelet effect), and chronic use may worsen gallstones (curcumin stimulates gallbladder contraction).
Ginger (Gingerols and Shogaols)
Ginger (Zingiber officinale) contains two main bioactive families: gingerols (predominant in fresh ginger, especially 6-gingerol) and shogaols (formed by dehydration during drying or cooking, especially 6-shogaol, which is more potent). Both inhibit COX-1, COX-2, and 5-LOX — the same enzyme triad targeted by NSAIDs — without the gastric mucosal toxicity of NSAIDs (in fact, ginger has been shown to be gastroprotective).
The clinical evidence: a 2015 meta-analysis (Daily et al.) of 7 randomized trials in osteoarthritis found ginger extract (typically 500–1,000 mg/day of a 4:1 to 10:1 extract) produced a modest but statistically significant reduction in pain. Ginger has the strongest evidence base of any oral antiemetic for pregnancy-related nausea (Cochrane Review 2014 and 2016 ACOG guideline) and for chemotherapy-induced nausea (NCI-sponsored Ryan 2012 trial). For migraine, a 2014 randomized trial showed ginger powder 250 mg sublingual was non-inferior to sumatriptan 50 mg for acute attack relief.
Practical use: 1–3 g of fresh ginger root per day (a thumb-sized piece, sliced or grated into stir-fries, soups, tea, or smoothies) supplies clinically meaningful doses. Dried ginger powder (1/2 to 1 tsp) is more concentrated in shogaols. For acute nausea or migraine, 250–500 mg of a standardized extract every 4 hours. Cautions: anticoagulant interaction (similar to curcumin), and high doses can lower blood glucose in diabetics on hypoglycemic medication.
Garlic (Allicin and Organosulfur Compounds)
Garlic (Allium sativum) acts through a sequential chemistry. Intact garlic cloves contain alliin (a sulfur-containing amino acid) and the enzyme alliinase, kept in separate cellular compartments. Crushing, chopping, or chewing brings the two together; alliinase converts alliin to allicin in seconds. Allicin then degrades within minutes into a family of organosulfur compounds (diallyl sulfide, diallyl disulfide, ajoene, S-allyl cysteine), each with distinct biological activity. Cooking heat inactivates alliinase — the key practical tip is to crush garlic and let it rest 10 minutes before cooking, allowing allicin to form and partially stabilize before heat exposure.
The clinical evidence is strongest for cardiovascular outcomes. The 2016 meta-analysis by Ried et al. of 39 trials and 4,083 participants found garlic supplementation produced an average reduction of 8–9 mm Hg systolic and 5–6 mm Hg diastolic blood pressure in hypertensive patients — comparable to a low-dose first-line antihypertensive. A separate meta-analysis (Sun 2018) of 22 trials found garlic reduced total cholesterol by ~17 mg/dL and LDL by ~9 mg/dL. The Kyolic aged-garlic-extract trials have additionally demonstrated reductions in coronary artery calcium progression on serial CT.
The inflammatory mechanism overlaps with cardiovascular: garlic organosulfurs inhibit NF-kappaB activation, reduce hs-CRP, reduce platelet aggregation (an additive antiplatelet effect important for anticoagulant interactions), and increase endothelial nitric oxide production. Garlic also has documented antimicrobial activity (the WWII "Russian penicillin" story) against gram-positive bacteria, candida, and several enveloped viruses.
Practical dose: 1–2 raw cloves per day (~3–6 g) crushed and rested for 10 minutes is the dietary therapeutic dose. Aged garlic extract (Kyolic) at 600–1,200 mg per day standardizes the dose and removes the breath odor concern; raw garlic enthusiasts can chew fresh parsley after meals to reduce odor.
Rosemary (Carnosic Acid and Carnosol)
Rosemary (Rosmarinus officinalis) is dominated by two diterpenes — carnosic acid and carnosol — and a small amount of rosmarinic acid. Carnosic acid is one of the most potent natural activators of the Nrf2 / Keap1 antioxidant response pathway, which upregulates endogenous antioxidant enzymes (glutathione peroxidase, superoxide dismutase, catalase, heme oxygenase-1) at the transcriptional level. This is a fundamentally different mechanism from direct radical scavenging by vitamin C or vitamin E — Nrf2 activation produces a sustained, amplified, enzymatic defense.
One particularly elegant practical application: marinating beef, lamb, or chicken in a rosemary-and-EVOO blend before high-temperature grilling reduces the formation of heterocyclic amines (HCAs) by 50–90% in laboratory studies (Smith 2008; Puangsombat 2011). The carnosic acid and carnosol act as radical scavengers during cooking, preventing the radical-mediated condensation reactions that produce HCAs from amino acids and creatine. If grilled meat is unavoidable, a 30-minute rosemary marinade is the single best harm-reduction step.
Practical use: 1–2 tsp fresh chopped rosemary (or 1/2 tsp dried) added to roasted vegetables, marinades, soups, breads, and pan sauces several times per week. Rosemary essential oil is concentrated and should not be taken orally without practitioner guidance; topical aromatherapy use has small evidence for memory enhancement.
Oregano (Carvacrol and Thymol)
Oregano (Origanum vulgare) and its close cousin thyme (Thymus vulgaris) share two principal phenolic monoterpenes — carvacrol and thymol. Both have well-characterized broad-spectrum antimicrobial activity (against gram-positive and gram-negative bacteria including MRSA in vitro, candida, dermatophytes, several enveloped viruses, and gut parasites including Giardia and Blastocystis). Both also inhibit COX-2 and 5-LOX, with carvacrol additionally suppressing TNF-alpha and IL-6 production by activated macrophages.
The clinical evidence base for oral oregano oil is mostly small trials in functional gastrointestinal conditions (SIBO, candida overgrowth, blastocystis), where it functions as a botanical antimicrobial. The 2014 Logan and Beaulieu pilot trial in SIBO showed eradication rates comparable to rifaximin in a small cohort. Oregano oil at 50–200 mg per day in enteric-coated capsules is the typical clinical dose; high doses can be gastric-irritating without enteric coating.
Practical culinary use is more accessible and lower-risk: 1–2 tsp fresh chopped oregano or 1/2 tsp dried, added to Mediterranean tomato sauces, pizza, roasted vegetables, salad dressings, and bean dishes. The polyphenol content of dried oregano is unusually preserved on storage compared with most herbs, so a 6-month-old jar still delivers meaningful carvacrol.
Cinnamon (Cinnamaldehyde)
Cinnamon comes in two principal forms: Ceylon cinnamon (Cinnamomum verum), the "true" cinnamon, and cassia (Cinnamomum cassia or Cinnamomum aromaticum), the cheaper and more common supermarket variety. Both deliver cinnamaldehyde, the principal flavor and bioactive compound. The critical difference: cassia is high in coumarin (~5–7 mg per teaspoon), a compound with hepatotoxic potential at chronic high intake. Ceylon cinnamon contains less than 0.1 mg coumarin per teaspoon. For daily medicinal use, Ceylon is the safer choice.
Cinnamon's best-documented benefit is glycemic. A 2012 Cochrane review (Leach & Kumar) and a 2013 meta-analysis (Allen et al.) of 10 randomized trials found cinnamon supplementation (typically 1–6 g/day) produced average reductions of ~25 mg/dL fasting glucose, ~16 mg/dL LDL, and ~10 mg/dL total cholesterol in patients with type 2 diabetes, with a smaller effect on HbA1c (~0.3%). The mechanism appears to involve insulin receptor signaling (cinnamaldehyde modulates insulin receptor phosphorylation) and inhibition of intestinal alpha-glucosidase.
Practical use: 1/2 to 1 tsp Ceylon cinnamon daily (3–6 g) on oatmeal, yogurt, in coffee or tea, or in baking. For type 2 diabetes adjunct treatment, capsule supplements at 1–3 g per day standardize dose. Cautions: cassia coumarin at high chronic intake (above ~6 g/day) can cause liver enzyme elevation in sensitive individuals; switch to Ceylon for daily medicinal use.
Saffron (Crocin and Safranal)
Saffron (Crocus sativus) — the dried stigma of the saffron crocus, the world's most expensive spice by weight — contains the carotenoid glycoside crocin (giving the deep yellow color), picrocrocin (the bitter principle), and safranal (the volatile aroma compound). All three have demonstrated anti-inflammatory activity, but saffron's most striking clinical evidence is in mood and cognition.
A 2019 meta-analysis (Toth et al.) of 23 randomized trials found saffron extract (typically 28–30 mg/day standardized to 2% safranal) produced antidepressant effects equivalent to fluoxetine 20 mg or imipramine 100 mg for mild-to-moderate major depressive disorder, with a substantially better side-effect profile. The active mechanism appears to be a combination of mild serotonin reuptake inhibition, dopaminergic modulation, BDNF upregulation, and reduction of neuroinflammatory cytokines.
Practical use: a generous pinch (~20 strands, roughly 50–100 mg) in paella, risotto Milanese, bouillabaisse, or rice pilaf 1–2 times per week. For depression adjunct treatment, a 30 mg standardized capsule daily, typically taken in two divided doses. Saffron is safe at culinary doses; doses above 1.5 g/day have caused toxicity, and doses above 5 g/day are potentially fatal — the therapeutic window is wide for capsule use, but powdered "saffron supplements" of unknown standardization should be avoided.
Bioavailability and Kitchen Pairings
Three principles maximize the biological effect of dietary spices:
- Pair fat-soluble actives with fat. Curcumin, carnosic acid, capsaicin, and astaxanthin are all lipophilic and require fat for absorption. The traditional Indian tadka technique (blooming spices in hot ghee or oil before adding to a dish) is the kitchen embodiment of this principle. EVOO is the appropriate Western analog.
- Use bioavailability enhancers when the science supports them. Piperine from freshly ground black pepper increases curcumin absorption ~20-fold. Quercetin (from onions and apples) inhibits curcumin glucuronidation by a different mechanism. A pinch of black pepper at the end of a turmeric-containing dish is a no-cost intervention.
- Time enzyme-dependent reactions correctly. Crushed garlic needs 10 minutes of bench rest for alliinase to convert alliin to allicin before cooking. Fresh ginger's 6-gingerol converts to more potent 6-shogaol during heating — both forms are useful, but raw ginger and cooked ginger have different active profiles.
A daily anti-inflammatory spice rotation does not require culinary expertise. A practical target: turmeric and black pepper in at least one cooked dish daily; fresh ginger 3–4 times per week; 1–2 cloves of garlic daily; fresh or dried oregano or rosemary in any savory cooking; Ceylon cinnamon in coffee, oatmeal, or yogurt daily; saffron in a weekly rice or fish dish. This pattern, cumulative across a year, supplies far more total polyphenol than any supplement regimen.
Key Research Papers
- Hewlings SJ, Kalman DS, Curcumin: A Review of Its Effects on Human Health (Foods 2017;6:92) — PubMed 29065496
- Shoba G et al., Influence of piperine on the pharmacokinetics of curcumin in animals and human volunteers (Planta Medica 1998;64:353-356) — PubMed 9619120
- Daily JW et al., Efficacy of Turmeric Extracts and Curcumin for Alleviating the Symptoms of Joint Arthritis (J Med Food 2016) — PubMed 27533649
- Ried K, Garlic Lowers Blood Pressure in Hypertensive Subjects: an Updated Meta-analysis and Review (J Nutr 2016) — PubMed 26764326
- Daily JW et al., Efficacy of Ginger for Alleviating the Symptoms of Primary Dysmenorrhea (Pain Med 2015) — PubMed 26177393
- Allen RW et al., Cinnamon use in type 2 diabetes: an updated systematic review and meta-analysis (Ann Fam Med 2013) — PubMed 24019277
- Toth B et al., The Efficacy of Saffron in the Treatment of Mild to Moderate Depression: A Meta-analysis (Planta Med 2019) — Search PubMed
- Puangsombat K et al., Inhibitory activity of asian spices on heterocyclic amines formation in cooked beef patties (J Food Sci 2011) — Search PubMed
- Sun YE et al., Effect of garlic powder intervention on blood cholesterol and triglyceride: meta-analysis (Asia Pac J Clin Nutr 2018) — Search PubMed
- Maggini V et al., Anti-inflammatory and antimicrobial activity of essential oils from Origanum vulgare (Oregano) PubMed: Oregano carvacrol
- Maridonneau-Parini I, Rosemary carnosic acid Nrf2 activation review PubMed: Rosemary Nrf2
- Ryan JL et al., Ginger (Zingiber officinale) reduces acute chemotherapy-induced nausea (Support Care Cancer 2012) — PubMed 21818642
Live PubMed Topic Searches
- PubMed: Curcumin clinical
- PubMed: Ginger
- PubMed: Garlic BP
- PubMed: Cinnamon diabetes
- PubMed: Saffron depression
- PubMed: Rosemary HCA reduction
Connections
- Benefits Hub
- Anti-Inflammatory Diet
- Mediterranean Foundations
- Omega-3 Rich Foods
- Foods to Avoid
- Turmeric
- Ginger
- Garlic
- Rosemary
- Oregano
- Cinnamon
- Saffron
- Rheumatology
- All Remedies