Anti-Inflammatory Diet: Omega-3 Rich Foods
Marine omega-3 fatty acids (EPA and DHA) are not just "heart-healthy fats" — they are the substrate the body uses to build resolvins, protectins, and maresins, an entire family of specialized pro-resolving mediators (SPMs) that actively terminate inflammation. Charles Serhan's lab at Harvard discovered these molecules in 2000–2007 and demonstrated they are the missing link between dietary fat composition and the body's ability to switch off an inflammatory episode cleanly. Without sufficient EPA and DHA in cell membranes, inflammation persists in a smoldering, unresolved state — the cellular signature of nearly every chronic disease. This deep-dive covers the SMASH fish, the omega-6 to omega-3 ratio problem, why plant ALA from flax and chia is a poor substitute for marine EPA/DHA, the REDUCE-IT trial of pharmaceutical-grade EPA, and a practical weekly plan to reach 2 g per day of combined EPA + DHA.
Table of Contents
- Resolvins, Protectins, and Maresins (SPMs)
- The SMASH Fish — Sardines, Mackerel, Anchovies, Salmon, Herring
- The Omega-6 to Omega-3 Ratio Problem
- ALA from Flax and Chia (and Why It Falls Short)
- REDUCE-IT and the Case for Pharmaceutical EPA
- Fish Oil, Krill Oil, and Algal DHA
- Mercury, Sustainability, and Practical Sourcing
- Reaching 2 g EPA+DHA per Day — A Practical Plan
- Key Research Papers
- Connections
- Featured Videos
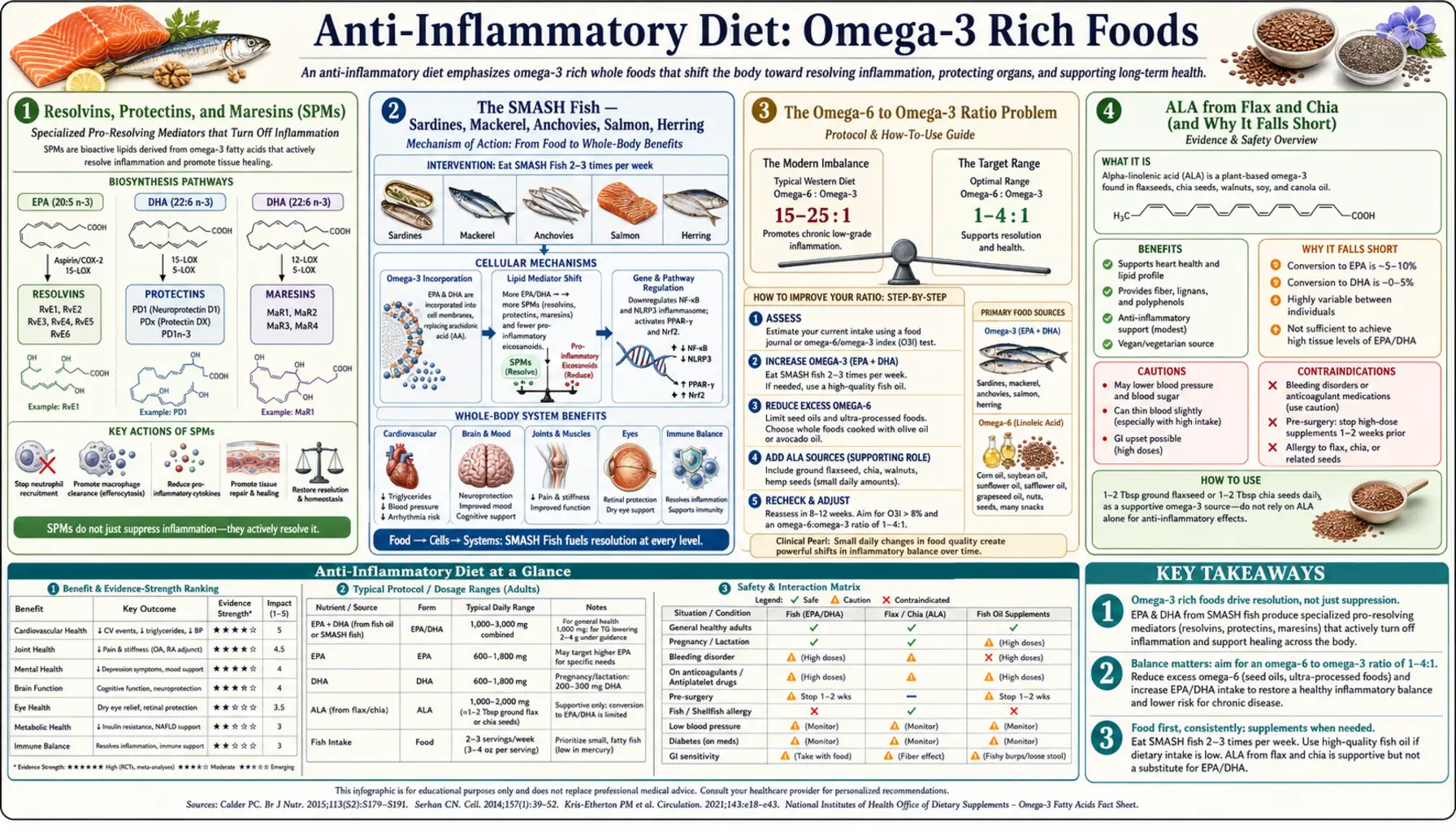
Resolvins, Protectins, and Maresins (SPMs)
For most of the 20th century, inflammation was thought to resolve passively — pro-inflammatory mediators simply got diluted, broken down, or cleared, and the tissue returned to baseline. The discovery of specialized pro-resolving mediators (SPMs) by Charles Serhan and colleagues at Harvard, in a series of papers from 2000 to 2007, overturned that view. Resolution of inflammation is an active, enzymatically-driven program. Its substrates are EPA and DHA.
The three SPM families are: (1) Resolvins — E-series resolvins (RvE1, RvE2, RvE3) derived from EPA, and D-series resolvins (RvD1 through RvD6) derived from DHA. They suppress neutrophil infiltration, promote macrophage clearance of apoptotic cells (efferocytosis), and stimulate antimicrobial defense without escalating inflammation. (2) Protectins — protectin D1 (PD1, also called neuroprotectin D1 in the CNS) derived from DHA. It protects neurons from oxidative stress and is reduced in Alzheimer's brain tissue. (3) Maresins — macrophage-derived from DHA, MaR1 and MaR2. They drive the macrophage phenotype switch from pro-inflammatory M1 to pro-resolving M2.
The clinical implication: without dietary EPA and DHA, the body cannot synthesize SPMs in adequate amounts, and inflammation does not resolve cleanly. The result is the smoldering, low-grade inflammation that drives atherosclerosis, insulin resistance, neurodegeneration, and the inflammatory tone of autoimmune disease. Restoring EPA/DHA intake within 6–12 weeks measurably increases circulating SPM levels and reduces the persistence of inflammatory episodes.
The SMASH Fish — Sardines, Mackerel, Anchovies, Salmon, Herring
The mnemonic SMASH covers the five categories of fatty cold-water fish with the highest EPA + DHA per serving and the lowest mercury and microplastic contamination (because they are small, short-lived, and feed low on the food chain). Per 100 g cooked serving:
- Sardines (Atlantic, canned in oil or water): ~1,500–2,000 mg EPA + DHA. Bone-in, skin-on; also delivers calcium, vitamin D, vitamin K2, selenium, B12. Mercury essentially undetectable.
- Mackerel (Atlantic): ~2,500–3,000 mg EPA + DHA. Note: King mackerel is high-mercury and should be avoided — Atlantic, Pacific chub, and Spanish mackerel are safe.
- Anchovies (canned in oil): ~1,000–1,500 mg per 50 g serving. Excellent flavor enhancer for sauces, dressings, and pasta.
- Salmon (wild Pacific or Atlantic farmed): ~1,500–2,200 mg per 100 g. Wild Pacific (sockeye, coho, pink) is leaner and has slightly less omega-3 by weight than farmed Atlantic, but with a more favorable omega-6 to omega-3 ratio and no contaminant concerns.
- Herring (pickled or smoked): ~1,800–2,300 mg per 100 g. A Scandinavian and central European staple.
Two servings per week of SMASH fish (~200 g cooked weight) supplies roughly 3–5 g of EPA + DHA per week, or ~500 mg per day averaged — the floor recommendation from the American Heart Association for cardiovascular prevention. To reach the 2 g per day used in PREDIMED-style trials and the REDUCE-IT pharmaceutical dose (4 g/day), most people need fish 3–4 times per week plus supplementation.
The Omega-6 to Omega-3 Ratio Problem
Ancestral human diets had an omega-6 to omega-3 ratio of roughly 1:1 to 4:1. Modern American and Western European diets typically run 15:1 to 25:1, dominated by linoleic acid from soybean, corn, sunflower, safflower, and cottonseed oils. The Simopoulos hypothesis (Artemis Simopoulos, Center for Genetics, Nutrition and Health) is that this dramatic ratio shift is the single largest dietary change underlying the rise in chronic inflammatory diseases since 1960.
The mechanism is competitive: omega-6 arachidonic acid and omega-3 EPA both compete for the same delta-5 and delta-6 desaturase enzymes, the same COX and LOX enzymes, and the same membrane phospholipid incorporation sites. When dietary linoleic acid swamps the system, arachidonic acid wins the competition, producing pro-inflammatory 2-series prostaglandins (PGE2), 4-series leukotrienes (LTB4), and pro-aggregatory thromboxane A2. When EPA wins, the system shifts to 3-series prostaglandins, 5-series leukotrienes (10 to 100 times less inflammatory), and the SPM family.
The practical lever has two arms: (1) reduce omega-6 by switching from seed oils to extra-virgin olive oil for cooking and dressings (see the foods to avoid page); and (2) increase omega-3 by eating SMASH fish 2–4 times per week and supplementing with fish, krill, or algal oil. Either lever moves the ratio toward 4:1; both levers together can reach 2:1 within 6 months.
ALA from Flax and Chia (and Why It Falls Short)
Plant omega-3 comes as alpha-linolenic acid (ALA, 18:3 n-3) from flaxseed, chia, walnuts, hemp, and some leafy greens. The body can elongate and desaturate ALA to EPA and then to DHA — but the conversion is poor and highly variable. Multiple human tracer studies (Brenna 2002, Burdge & Wootton 2002) show conversion of ALA to EPA in the range of 5–10%, and conversion to DHA in the range of 0.5–5%. Women generally convert more efficiently than men because estrogen upregulates the delta-6 desaturase, but even at the upper end, dietary ALA cannot reliably substitute for direct marine EPA and DHA.
The bottleneck is the elongase and desaturase enzymes (FADS1, FADS2, ELOVL5), which are saturable, competitive with omega-6 substrates, and modulated by polymorphisms. A 2017 study by Lankinen et al. found that an FADS1 minor allele present in roughly 30% of European populations reduces EPA/DHA synthesis from ALA by an additional 30–50%.
This does not mean flax, chia, hemp, and walnuts are useless — they deliver fiber, lignans, magnesium, and a baseline of ALA that contributes to overall omega-3 status. But strict vegetarians and vegans cannot rely on ALA alone for adequate EPA and DHA; algal oil supplementation (which provides direct DHA and a small amount of EPA) is the appropriate substitute. Two tablespoons of ground flaxseed daily plus an algal DHA capsule (typically 300–500 mg DHA) is the standard plant-based regimen.
REDUCE-IT and the Case for Pharmaceutical EPA
The Reduction of Cardiovascular Events with Icosapent Ethyl Intervention Trial (REDUCE-IT, Bhatt et al. NEJM 2019) enrolled 8,179 statin-treated patients with elevated triglycerides (135–499 mg/dL) and high cardiovascular risk. They were randomized to 4 g per day of icosapent ethyl (a purified ethyl ester of EPA only, no DHA) or mineral oil placebo, with a median follow-up of 4.9 years. The primary endpoint was a composite of cardiovascular death, nonfatal MI, nonfatal stroke, coronary revascularization, or unstable angina.
The result was a 25% relative risk reduction in the primary endpoint (17.2% vs 22.0%, p<0.001) and a 20% reduction in cardiovascular death. The benefit emerged early (visible by 1 year) and persisted throughout follow-up. It was independent of LDL lowering and only partly explained by triglyceride reduction — suggesting a direct anti-inflammatory and plaque-stabilizing effect of EPA at the 4 g/day dose.
The clinical interpretation has been controversial because the mineral oil placebo may have raised hs-CRP and LDL in the control arm, exaggerating the apparent benefit. The subsequent STRENGTH trial (Nicholls et al. JAMA 2020), which tested a combined EPA + DHA preparation against a corn oil placebo, did not show benefit — but its dose, formulation, and patient population differed. The current pragmatic position: in statin-treated patients with residual triglyceride elevation and high cardiovascular risk, prescription icosapent ethyl at 4 g/day has the strongest evidence. For the general anti-inflammatory diet, 1–2 g/day of combined EPA + DHA from food plus a modest supplement is the more conservative approach.
Fish Oil, Krill Oil, and Algal DHA
For supplementation beyond dietary fish, the three principal options are:
- Standard fish oil (triglyceride or ethyl ester form): the most studied and lowest-cost option. Look for IFOS or USP third-party certification for purity (mercury, PCBs, oxidation). Typical concentration is 30% EPA + DHA in a 1000 mg softgel, so a 2 g/day target requires 6–7 softgels; concentrated formulations (60–80%) reduce that to 2–3 softgels.
- Krill oil: phospholipid-bound EPA and DHA from Antarctic krill, plus astaxanthin (a potent carotenoid antioxidant). The phospholipid form may have modestly better absorption per mg of EPA/DHA than triglyceride fish oil, though head-to-head trials are mixed. More expensive and lower total EPA+DHA per capsule.
- Algal DHA (and EPA): derived directly from microalgae (Schizochytrium), the same source from which the fish originally acquired their omega-3s. Provides 300–500 mg DHA per capsule (some formulations now add EPA). Vegan, no fishy taste, no ocean-contaminant exposure. The default choice for plant-based eaters.
Oxidation is a real concern with fish oil — rancid product produces lipid peroxides that are themselves pro-inflammatory. Buy from reputable brands, refrigerate after opening, and discard if the capsules smell strongly fishy or the oil tastes burnt. The IFOS certification specifically tests for oxidation as well as contaminants.
Mercury, Sustainability, and Practical Sourcing
Mercury bioaccumulates up the food chain, so the largest predatory fish carry the highest body burdens. The FDA/EPA "avoid" list (especially for pregnancy and young children) is: king mackerel, marlin, orange roughy, shark, swordfish, tilefish from the Gulf of Mexico, bigeye tuna. The "eat 1 serving per week" list is canned albacore (white) tuna, halibut, snapper, grouper. The "eat 2–3 servings per week" list is canned light tuna, salmon, shrimp, sardines, mackerel (Atlantic/Pacific chub), anchovies, herring, trout, tilapia.
Sustainability matters because overfishing of small forage fish (anchovies, sardines, herring) destabilizes the entire ocean food web. The Monterey Bay Aquarium Seafood Watch (seafoodwatch.org) provides species-by-species sustainability guidance. For most North American consumers, the highest-EPA, lowest-mercury, sustainable picks are wild Alaskan sockeye salmon, Atlantic and Pacific sardines, Pacific anchovies, and small Atlantic herring.
Reaching 2 g EPA+DHA per Day — A Practical Plan
A reasonable weekly target for active anti-inflammatory benefit (not just deficiency prevention) is roughly 14 g of EPA + DHA per week, or 2 g per day averaged. One pragmatic combination:
- Monday: 1 can sardines (~120 g) on whole-grain toast for lunch — ~2,200 mg EPA+DHA
- Wednesday: 150 g wild salmon for dinner — ~2,500 mg EPA+DHA
- Friday: Anchovy-puttanesca pasta (50 g anchovies in sauce) — ~1,000 mg EPA+DHA
- Sunday: Mackerel pate or smoked mackerel salad (100 g) — ~2,700 mg EPA+DHA
- Daily supplement: 2 softgels of concentrated fish oil (60%) providing ~700 mg EPA+DHA per day, or 4 softgels of standard fish oil (30%) providing similar — ~5,000 mg per week
Total: roughly 13,000–14,000 mg EPA+DHA per week, or ~1,900–2,000 mg per day. Vegan equivalent: 1 algal DHA+EPA capsule (~500 mg DHA + 100 mg EPA) daily plus 2 tablespoons of ground flaxseed and 30 g walnuts daily, totaling about 4,500–5,500 mg combined EPA + DHA + ALA per week.
The biomarker to follow is the Omega-3 Index (a Holman blood test measuring EPA+DHA as percent of total red blood cell fatty acids). The protective range is ≥8%; the deficient range (associated with sudden cardiac death and cognitive decline) is <4%. Most untreated Americans run at 4–6%; the plan above will typically raise the index to 8–12% within 4–6 months.
Key Research Papers
- Bhatt DL et al., Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia (REDUCE-IT, NEJM 2019;380:11-22) — PubMed 30415628
- Serhan CN, Pro-resolving lipid mediators are leads for resolution physiology (Nature 2014;510:92-101) — PubMed 24899309
- GISSI-Prevenzione Investigators, Dietary supplementation with n-3 polyunsaturated fatty acids after myocardial infarction (Lancet 1999) — PubMed 10465168
- Calder PC, Omega-3 fatty acids and inflammatory processes: from molecules to man — PubMed 28900017
- Brenna JT, Efficiency of conversion of alpha-linolenic acid to long chain n-3 fatty acids in man Search PubMed
- Nicholls SJ et al., Effect of High-Dose Omega-3 Fatty Acids vs Corn Oil on Major Adverse Cardiovascular Events (STRENGTH, JAMA 2020) — PubMed 33190147
- Harris WS, Von Schacky C, The Omega-3 Index: a new risk factor for death from coronary heart disease? — PubMed 15208005
- Mozaffarian D, Rimm EB, Fish intake, contaminants, and human health: evaluating the risks and the benefits (JAMA 2006) — PubMed 17047219
- Simopoulos AP, The importance of the ratio of omega-6/omega-3 essential fatty acids — PubMed 12442909
- Goldberg RJ, Katz J, A meta-analysis of the analgesic effects of omega-3 polyunsaturated fatty acid supplementation for inflammatory joint pain — PubMed 17335973
- Liao Y et al., Efficacy of omega-3 PUFAs in depression: a meta-analysis (Transl Psychiatry 2019) — PubMed 31383846
- Burdge GC, Calder PC, Conversion of alpha-linolenic acid to longer-chain polyunsaturated fatty acids in human adults — PubMed 16188209
Live PubMed Topic Searches
- PubMed: SPM family
- PubMed: EPA/DHA cardiovascular
- PubMed: Omega-3 RA
- PubMed: Omega-3 Index
- PubMed: Algal DHA
- PubMed: Fish oil and depression
Connections
- Benefits Hub
- Anti-Inflammatory Diet
- Mediterranean Foundations
- Spices and Herbs
- Foods to Avoid
- Salmon
- Sardines
- Herring
- Cod
- Fish Oil
- Cardiology
- Rheumatology
- All Remedies