Anti-Inflammatory Diet: Mediterranean Foundations
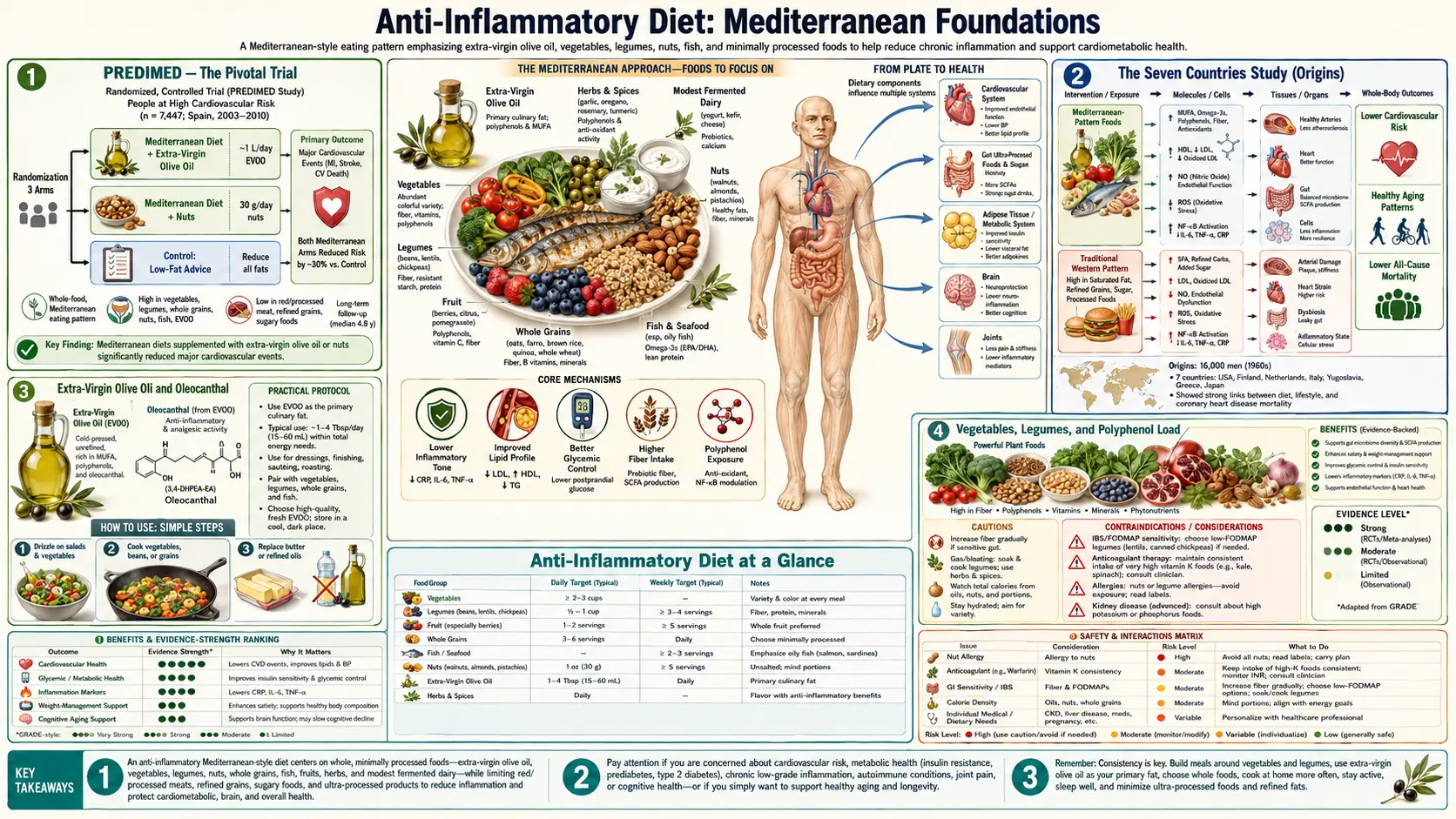
The Mediterranean diet is the most rigorously studied dietary pattern in human nutrition. It is the only eating pattern with a successfully completed, primary-prevention, hard-endpoint randomized controlled trial (PREDIMED) showing a roughly 30% reduction in major cardiovascular events versus a low-fat control diet. Its anti-inflammatory effect is not driven by any single hero ingredient — it is the cumulative result of extra-virgin olive oil as the principal fat source, a daily floor of vegetables and legumes, moderate fish and poultry, very limited red and processed meat, and red wine in moderation with meals. This page maps the seven foundational food categories of the Mediterranean pattern to the specific inflammatory pathways each modulates, then translates the science into a practical pantry and weekly meal blueprint.
Table of Contents
- PREDIMED — The Pivotal Trial
- The Seven Countries Study (Origins)
- Extra-Virgin Olive Oil and Oleocanthal
- Vegetables, Legumes, and Polyphenol Load
- Whole Grains, Nuts, and Seeds
- Fish and the Animal-Protein Hierarchy
- Red Wine in Moderation (and the Caveats)
- A Practical Weekly Pantry and Plate
- Key Research Papers
- Connections
- Featured Videos
PREDIMED — The Pivotal Trial
The Prevención con Dieta Mediterránea (PREDIMED) trial enrolled 7,447 Spanish adults aged 55–80 at high cardiovascular risk (with type 2 diabetes or at least three risk factors) and randomized them to one of three diets: (1) a Mediterranean diet supplemented with about one liter per week of extra-virgin olive oil, (2) a Mediterranean diet supplemented with about 30 grams per day of mixed nuts (walnuts, almonds, hazelnuts), or (3) a low-fat control diet. Participants were followed for a median 4.8 years, and the primary endpoint was a composite of myocardial infarction, stroke, and cardiovascular death.
The trial was stopped early for efficacy. The 2018 reanalysis (Estruch et al. NEJM 2018, after the original 2013 paper was reanalyzed for randomization concerns) confirmed a relative risk reduction of approximately 30% for the primary composite endpoint in both Mediterranean diet arms versus the low-fat control, with a number needed to treat of about 60 over five years. Stroke risk in particular was reduced by 35–45%. Critically, both Mediterranean arms achieved the benefit despite no significant weight loss compared with the control diet — demonstrating that the inflammatory and cardiovascular benefit comes from food composition, not calorie restriction.
The mechanistic substudies of PREDIMED, in subsets of 500–1,000 participants, documented reductions in high-sensitivity C-reactive protein, interleukin-6, soluble intercellular adhesion molecule 1 (sICAM-1), and oxidized LDL within 12 months. These markers all sit on the pathway from chronic inflammation to atherosclerotic plaque rupture, and their reduction is the most plausible mechanism for the observed event reduction.
The Seven Countries Study (Origins)
The Mediterranean diet entered scientific consciousness through Ancel Keys' Seven Countries Study, launched in 1958. Keys compared diet and coronary heart disease rates in 12,763 middle-aged men across Finland, the Netherlands, Italy, Greece (Crete and Corfu), Yugoslavia, the United States, and Japan. The Cretan cohort had the lowest 10-year and 25-year coronary mortality — far below Finland and the United States — despite a total fat intake of approximately 37% of calories. The fat composition, however, was dominated by extra-virgin olive oil (monounsaturated) and contained little saturated fat from meat or dairy.
The study also documented that the protective Cretan pattern depended on a complete food environment: daily vegetables and legumes, moderate fish and goat dairy, infrequent meat (often only on Sundays), wine with meals, and high physical activity from walking and farming. Subsequent decades of work (Trichopoulou's 2003 NEJM paper on the Mediterranean adherence score, then PREDIMED in 2013/2018) translated this observation into a quantifiable, reproducible dietary pattern.
Extra-Virgin Olive Oil and Oleocanthal
Extra-virgin olive oil (EVOO) is the keystone fat of the Mediterranean pattern. PREDIMED used roughly one liter per week per household, or about 40–50 mL per person per day — far more than most Americans consume. The anti-inflammatory effect comes from three components: (1) approximately 73% oleic acid (monounsaturated 18:1), which is metabolically neutral or slightly anti-inflammatory; (2) approximately 200–500 mg/kg of polyphenols, dominated by hydroxytyrosol, tyrosol, and oleuropein, all potent free-radical scavengers and modulators of NF-kappaB; and (3) oleocanthal, a phenolic compound that produces the characteristic peppery throat-burn of high-quality EVOO.
The 2005 Nature paper by Beauchamp and colleagues demonstrated that oleocanthal is a natural, dose-dependent inhibitor of cyclooxygenase-1 and cyclooxygenase-2 — the same enzymes blocked by ibuprofen and aspirin. A typical 50 mL serving of robust EVOO contains roughly 9 mg of oleocanthal, equivalent in COX inhibition to about 10% of a single 200 mg ibuprofen dose. Cumulative daily exposure produces a small but durable shift in eicosanoid synthesis.
Practical buying notes: look for "extra-virgin" on the label (a defined chemical standard, not a marketing term), a harvest date (polyphenols degrade over 12–18 months), a dark glass bottle (light degrades polyphenols), and a country of origin you trust (single-country Italian, Greek, or Spanish typically better than multi-country blends). Cooking does not destroy the oleic acid (EVOO is stable to 405°F / 207°C), and high-polyphenol oils remain protective during typical sauteing.
Vegetables, Legumes, and Polyphenol Load
The Mediterranean pattern targets approximately 5–7 servings of vegetables per day plus 3–4 servings per week of legumes (chickpeas, lentils, white beans, fava beans). Three benefits operate in parallel:
- Soluble and insoluble fiber — legumes deliver 6–8 g of fiber per half-cup serving, half soluble. Soluble fiber is fermented by colonic bacteria into short-chain fatty acids (butyrate, propionate, acetate), which strengthen intestinal epithelial tight junctions, reduce LPS translocation, and provide the principal energy source for colonocytes.
- Polyphenol diversity — deeply colored vegetables (red cabbage, beets, eggplant, dark leafy greens, tomatoes) and pulses each contribute distinct polyphenol classes (anthocyanins, flavonols, isoflavones, betalains). The diversity matters because each class modulates a different set of inflammatory targets; cumulative exposure across 20–30 plant species per week is the goal.
- Plant protein substitution — legumes replace some of the red meat protein in the diet without sacrificing satiety, reducing total saturated fat, heme iron load, and AGE exposure from high-temperature cooking.
The minimum effective dose to produce a measurable hs-CRP reduction in randomized trials is roughly 400 g (about 5 servings) of vegetables per day. Cooking method matters: steaming, sauteing in EVOO, and raw all preserve polyphenols; high-temperature deep-frying and prolonged boiling (especially of polyphenol-rich vegetables) lose 30–70% of phenolic content to the cooking water.
Whole Grains, Nuts, and Seeds
The PREDIMED nut arm provided 15 g of walnuts, 7.5 g of almonds, and 7.5 g of hazelnuts daily (~30 g total, roughly a handful). The nut arm achieved the same approximately 30% cardiovascular event reduction as the EVOO arm. The contributing components are (1) alpha-linolenic acid (the plant omega-3, particularly concentrated in walnuts at about 2.5 g per ounce), (2) magnesium and potassium, (3) plant sterols, (4) arginine (an NO precursor that improves endothelial function), and (5) polyphenol load from the skins.
Whole grains contribute fiber, magnesium, B vitamins, and lignans. The traditional Mediterranean staples are bulgur, farro, barley, oats, and stone-ground whole-wheat pasta — not refined white bread or white pasta. The shift from refined to whole grains lowers postprandial glucose excursions, reduces glycation pressure, and feeds the same fiber-fermenting colonic bacteria that legumes do. The PURE study (Dehghan et al. Lancet 2017) and a 2016 BMJ meta-analysis both link 3 servings per day of whole grains to a roughly 20% reduction in all-cause and cardiovascular mortality.
Seeds — flax, chia, hemp, sesame, sunflower — add additional ALA, lignans, and minerals. Two tablespoons of ground flaxseed daily delivers about 3 g of ALA plus the SDG lignan that is converted by gut bacteria to mammalian lignans with weak estrogenic and anti-inflammatory activity.
Fish and the Animal-Protein Hierarchy
The traditional Mediterranean diet places fish at the top of the animal-protein hierarchy (2–3 times per week), poultry in the middle (1–2 times per week), and red and processed meat at the bottom (no more than a few times per month). The fish recommendation specifically targets fatty cold-water species — sardines, anchovies, herring, mackerel, salmon — because these supply the marine omega-3s (EPA and DHA) that drive the resolvin and protectin pathways covered on the omega-3 deep-dive page.
The case for restricting red and processed meat in an anti-inflammatory pattern rests on three observations: (1) the 2015 IARC Monograph 114 classified processed meat as Group 1 (carcinogenic to humans) for colorectal cancer and red meat as Group 2A (probably carcinogenic); (2) heme iron from red meat increases gut lipid peroxidation and circulating N-nitroso compounds; and (3) the Maillard browning that develops on charred, grilled, or pan-seared meat produces advanced glycation end products (AGEs) and heterocyclic amines that activate the RAGE receptor and drive systemic inflammation.
For patients who eat meat, the harm-reduction Mediterranean approach is (1) shift from beef and pork toward poultry and fish; (2) prefer braised, stewed, or low-temperature preparations over grilled and charred; (3) marinate with acidic herb mixes (rosemary, lemon, vinegar) which reduce heterocyclic amine formation; and (4) keep portion size to roughly the palm of the hand, with the rest of the plate occupied by vegetables and legumes.
Red Wine in Moderation (and the Caveats)
The traditional Cretan diet included red wine with meals (typically 1–2 small glasses per day), and PREDIMED's Mediterranean diet score gave a half-point for moderate wine consumption. Red wine delivers resveratrol, anthocyanins, and proanthocyanidins that show anti-inflammatory and endothelial-protective effects in mechanistic studies.
The clinical caveat is significant. The 2018 Lancet Global Burden of Disease alcohol analysis found that the safest level of alcohol consumption for overall health is zero, once cancer (especially breast, head/neck, esophagus, colorectum), liver disease, and accidents are factored in. The cardiovascular benefit of light drinking does not offset the cancer risk in modern populations, and the J-shaped curve of earlier observational studies has been challenged by Mendelian randomization analyses showing dose-dependent harm at all levels.
The practical take: if a patient already drinks wine in moderation (1 glass per day for women, 1–2 for men) and has no personal or family history of breast cancer or alcohol use disorder, the Mediterranean pattern is compatible with continuing that habit. Recommending wine to a non-drinker for health is not supported by the evidence. The polyphenol and resveratrol load can be obtained more safely from concord grape juice, berries, dark chocolate, and tea.
A Practical Weekly Pantry and Plate
A reproducible Mediterranean shopping list for one adult per week looks roughly like this:
- Olive oil: 250–350 mL of robust extra-virgin olive oil (single-origin, harvest date within 12 months).
- Vegetables: 2 kg total — tomatoes, cucumbers, peppers, onions, garlic, leafy greens, eggplant, zucchini, cruciferous (broccoli, cauliflower), one root vegetable.
- Legumes: 400 g dried (or 3–4 cans) of chickpeas, lentils, white beans, or fava beans.
- Whole grains: 500 g of bulgur, farro, oats, barley, or stone-ground whole-wheat pasta.
- Fruit: 1 kg mixed — citrus, berries, apples, melon, figs, pomegranate when in season.
- Nuts and seeds: 250 g mixed — walnuts, almonds, hazelnuts, pumpkin seeds, ground flaxseed.
- Fish: 400–600 g per week, mostly fatty cold-water species (canned sardines, frozen mackerel, fresh or frozen salmon).
- Poultry, eggs, dairy: 1–2 servings of chicken or turkey, 6–7 eggs, 200–400 g of yogurt or feta.
- Herbs and spices: rotating rosemary, oregano, thyme, basil, parsley, mint, turmeric, ginger, garlic, cinnamon, black pepper — see the spices page.
- Limit or skip: red and processed meat, refined grains, sugar-sweetened beverages, ultra-processed snack foods, industrial seed oils — see the foods to avoid page.
The plate model: half the plate vegetables (cooked and raw), one quarter whole grains or legumes, one quarter protein (fish more often than poultry; legumes more often than meat), with extra-virgin olive oil drizzled liberally, herbs as the principal flavoring, and a piece of fruit for dessert. This pattern alone — without supplements, without calorie counting — reproduces the PREDIMED intervention.
Key Research Papers
- Estruch R et al., Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts (NEJM 2018, retracted-and-republished reanalysis of 2013) — PubMed 29897866
- Beauchamp GK et al., Phytochemistry: ibuprofen-like activity in extra-virgin olive oil (Nature 2005;437:45-46) — PubMed 16136122
- Trichopoulou A et al., Adherence to a Mediterranean diet and survival in a Greek population (NEJM 2003;348:2599-2608) — PubMed 12826634
- Salas-Salvado J et al., Prevention of Diabetes With Mediterranean Diets: A Subgroup Analysis of a Randomized Trial (Ann Intern Med 2014) — Search PubMed
- Casas R et al., The effects of the Mediterranean diet on biomarkers of vascular wall inflammation and plaque vulnerability in subjects with high risk for cardiovascular disease — PubMed 24925270
- Schwingshackl L, Hoffmann G, Mediterranean dietary pattern, inflammation and endothelial function: a systematic review and meta-analysis — PubMed 25149893
- Sofi F et al., Adherence to Mediterranean diet and health status: meta-analysis (BMJ 2008) — PubMed 18786971
- Dinu M et al., Mediterranean diet and multiple health outcomes: an umbrella review of meta-analyses — PubMed 28488692
- Keys A et al., The diet and 15-year death rate in the seven countries study — PubMed 3776973
- Scarmeas N et al., Mediterranean diet and risk for Alzheimer's disease (Ann Neurol 2006) — PubMed 16622828
- Toledo E et al., Mediterranean diet and invasive breast cancer risk among women at high cardiovascular risk in PREDIMED — PubMed 26365989
- Salas-Huetos A et al., The effect of nuts on markers of inflammation and oxidative stress: a systematic review Search PubMed
Live PubMed Topic Searches
- PubMed: PREDIMED cardiovascular
- PubMed: Olive oil oleocanthal
- PubMed: Mediterranean diet inflammation
- PubMed: Mediterranean metabolic syndrome
- PubMed: Mediterranean cognition
- PubMed: Legumes and CVD
Connections
- Benefits Hub
- Anti-Inflammatory Diet
- Omega-3 Rich Foods
- Spices and Herbs
- Foods to Avoid
- Olive Oil
- Salmon
- Sardines
- Lentils
- Cardiology
- Type 2 Diabetes
- All Remedies