Iodine Deficiency: Pregnancy and Brain Development
Of all the harms that come from running low on iodine, the one that matters most cannot be felt, seen, or undone — it happens silently, inside a developing baby's brain, before the child is ever born. Iodine is the raw material the body uses to build thyroid hormone, and thyroid hormone is the signal that tells a growing brain how and when to wire itself. When a pregnant woman doesn't get enough iodine, her baby may be born with a brain that was built on a quieter signal — and the result, on average, is a small but permanent loss of IQ. At the severe end, lifelong iodine starvation in pregnancy causes cretinism: profound, irreversible intellectual disability. This is why iodine deficiency is, worldwide, the leading preventable cause of intellectual disability — and why the few months around conception and pregnancy are the moment when getting iodine right matters more than at any other time of life.
Table of Contents
- What This Looks Like — Often Nothing at All
- The Mechanism: How Iodine Builds a Brain
- The Spectrum: From a Few IQ Points to Cretinism
- Being Honest: Many Things Affect a Child's Brain
- When to Suspect Iodine Is the Problem
- Why Pregnant Women Run Low
- Getting Tested: A Hard Thing to Measure
- Getting Enough — Before and During Pregnancy
- When to Seek Care
- Key Research Papers
- Connections
- Featured Videos
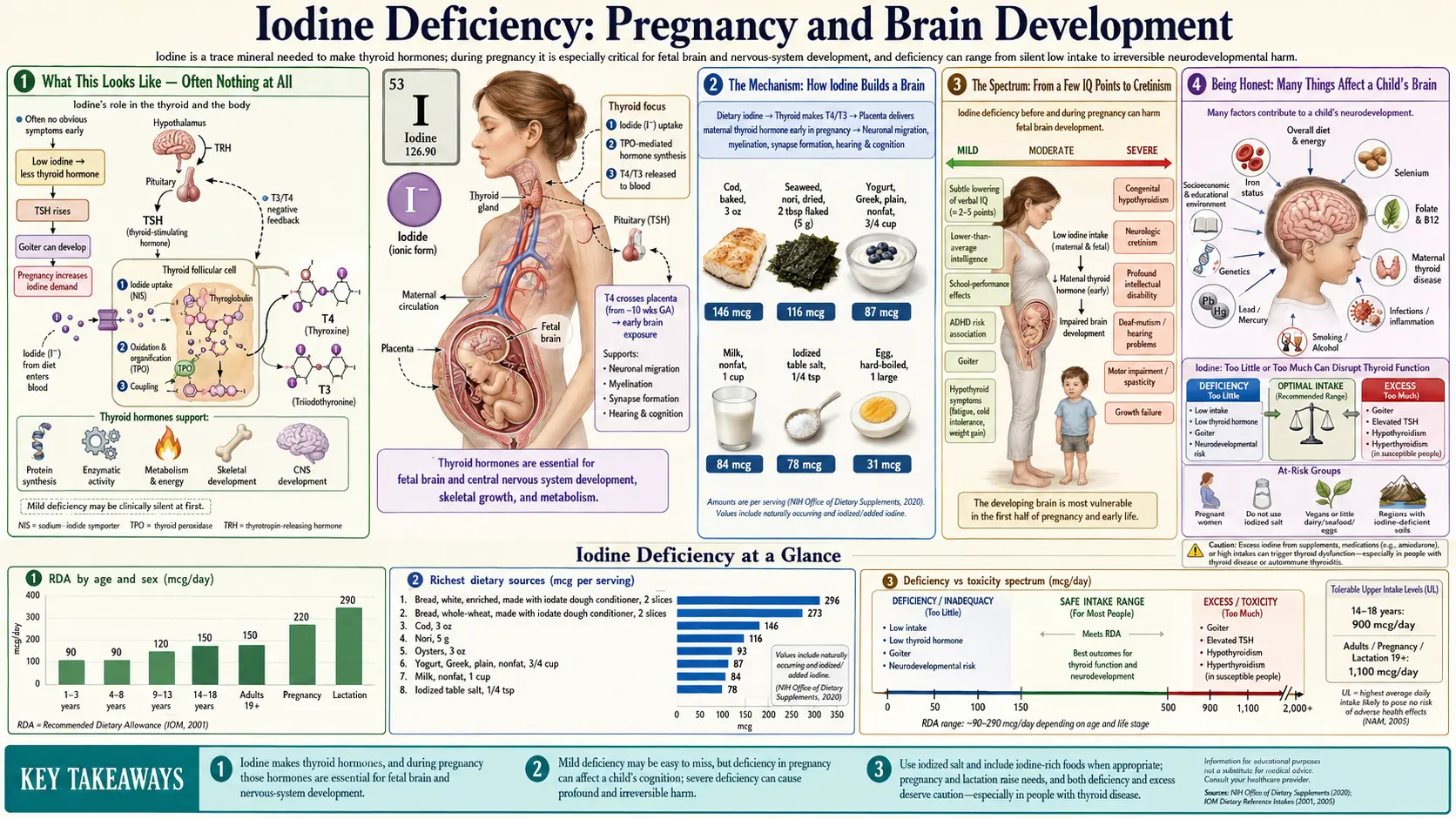
What This Looks Like — Often Nothing at All
This page is different from the other deficiency symptom pages, and it is important to say so plainly: mild iodine deficiency in pregnancy usually produces no symptom the mother can feel. She is not in pain. She is not unusually tired. Her baby's brain development is being quietly shaped, but nothing announces it. This is the cruelty of the problem — the harm is invisible while it is happening, and by the time anything could be noticed in the child, the window to prevent it has already closed.
What a mother might notice are the more general signs of low thyroid function that can accompany deficiency: a swelling at the front of the neck (a goiter), fatigue, feeling cold, or sluggishness (see hypothyroidism and fatigue and weight gain and cold sensitivity). But many women with mild-to-moderate iodine deficiency have none of these and feel completely well. Their thyroid is quietly working harder to squeeze enough hormone out of a limited iodine supply, and it often manages — for her. The shortfall shows up instead in the baby, whose brain is being built on whatever thyroid signal her body can spare.
In the child, the effects are equally undramatic in the mild range. There is no birthmark, no obvious sign in infancy. The difference — on average, a few IQ points, slightly slower acquisition of language, modestly lower reading or spelling scores at school age — is real at the level of populations but invisible in any one child. It is only when researchers measure thousands of children whose mothers' iodine status was recorded in pregnancy that the pattern becomes unmistakable. At the severe end, by contrast, the harm is anything but subtle, as the section on the spectrum below describes.
The Mechanism: How Iodine Builds a Brain
To understand why iodine in pregnancy matters so much, you have to follow a short chain. Iodine has essentially one job in the human body: it is the irreplaceable ingredient of thyroid hormone. The thyroid gland traps iodine from the blood and attaches it to a protein scaffold to make two hormones — thyroxine (T4), which carries four iodine atoms, and triiodothyronine (T3), which carries three. The numbers in the names are the iodine atoms. No iodine, no hormone. (For the full biochemistry, see iodine and thyroid function.)
Thyroid hormone, in turn, is one of the master regulators of brain development. In the growing fetal brain it controls a remarkable list of jobs: the multiplication of nerve cells, their migration to the right places, the growth of the branches (axons and dendrites) that let neurons talk to one another, the formation of synapses, and myelination — the wrapping of nerve fibers in the fatty insulation that lets signals travel fast and cleanly. Thyroid hormone is, in effect, the conductor that keeps this construction project on schedule. When the hormone signal is weak, the timing slips, and because brain development runs on a strict biological calendar, steps that are missed or muffled at the right moment cannot simply be made up later.
An analogy. Think of building the brain as constructing a vast highway network on a fixed deadline. Thyroid hormone is the supervisor radioing instructions to every crew — lay this road now, connect that junction, insulate these wires. Iodine is the battery in the supervisor's radio. With a full battery, every crew hears every instruction and the network is built correctly and on time. With a weak battery, the instructions come through faint and garbled; the crews do their best, but some roads end up narrower, some junctions never quite connect, and some wiring is left poorly insulated. The highway still opens — the child is born and grows up — but it never carries traffic quite as efficiently as it should have. And because the construction deadline has passed, you cannot go back and rebuild the missed junctions.
The timing detail is what makes pregnancy uniquely important. In the first trimester, the fetal thyroid is not yet working — it cannot make its own hormone until roughly week 18–20. During those critical early weeks, the fetus depends entirely on thyroid hormone crossing the placenta from the mother. So a mother's iodine supply in early pregnancy — and indeed in the weeks before conception, when her thyroid stores are being set — directly determines the hormone signal reaching her baby's brain at the very stage when the brain's basic architecture is being laid down. To meet this demand, a healthy thyroid increases its hormone output by about 50% in pregnancy, which raises the body's iodine requirement well above the non-pregnant level. If iodine is in short supply, the mother simply cannot ramp up production, and the fetal brain develops on a quieter signal.
The Spectrum: From a Few IQ Points to Cretinism
The damage from iodine deficiency in pregnancy is not all-or-nothing. It runs along a continuous spectrum, and where a child lands on it depends largely on how severe and how early the mother's deficiency was.
Severe deficiency — cretinism. At the extreme end, when a mother is profoundly iodine-deficient throughout pregnancy (historically common in remote, mountainous, iodine-poor regions far from the sea), the result can be cretinism — a syndrome of severe, permanent intellectual disability. The older medical term endures because the condition is so distinct. Two forms are described. Neurological cretinism — the more common form — features profound intellectual disability, deaf-mutism, and a spastic, stiff gait, and is thought to arise from thyroid hormone deficiency during the first half of pregnancy, when the mother is the only source. Myxedematous cretinism features stunted growth and the signs of severe lifelong hypothyroidism, and is linked to thyroid damage continuing later in pregnancy and after birth. Crucially, cretinism is almost entirely preventable — correcting a population's iodine supply before and during pregnancy abolishes it — but once a child is born with it, the brain injury cannot be reversed by giving iodine afterward. The damage was done during construction.
Mild-to-moderate deficiency — lost IQ points. For most of the world, the relevant question today is not cretinism but the far subtler effect of mild-to-moderate deficiency, which is still surprisingly common even in wealthy countries. Here the harm is a modest, population-wide downward shift in cognitive ability. The landmark evidence comes from large birth-cohort studies. In the UK ALSPAC study (Bath and colleagues, 2013), the children of women who had been mildly-to-moderately iodine-deficient in the first trimester were significantly more likely to score in the bottom quartile for verbal IQ, reading accuracy, and reading comprehension at ages 8–9, even after accounting for many other influences. Norway's large MoBa cohort (Abel and colleagues, 2017) similarly linked a low maternal iodine intake to poorer language, fine-motor, and behavioral development in three-year-olds. Reviews and meta-analyses (Bougma 2013; Skeaff 2011) estimate that chronic iodine deficiency is associated with a loss on the order of 10–15 IQ points at the level of affected populations.
A few lost IQ points may sound trivial for one child. Across an entire population it is not. A downward shift of the whole bell curve means many more children at the low-functioning end who struggle in school, and fewer at the high end — a quiet, collective loss of human potential that, unlike cretinism, never produces a single dramatic case to point to. That diffuse, invisible quality is exactly why public-health authorities take mild deficiency so seriously despite its lack of obvious victims.
Being Honest: Many Things Affect a Child's Brain
It would be misleading to suggest that a child's intelligence, language, or school performance comes down to a single nutrient. It does not, and a page on this site would be doing a disservice to imply otherwise. A child's cognitive development is shaped by a long list of factors, and iodine is only one thread in a large weave:
- Genetics — inherited factors are among the strongest influences on measured cognitive ability.
- Other nutrients — iron deficiency (the most common nutritional deficiency worldwide) impairs early cognitive development; folate around conception, vitamin B12, choline, zinc, and omega-3 fatty acids (DHA) all matter for the developing brain.
- The mother's own thyroid health — overt or even subclinical maternal hypothyroidism, or thyroid autoimmunity such as Hashimoto's thyroiditis, can lower the hormone signal to the fetus independently of iodine.
- Exposures in pregnancy — alcohol, smoking, lead, and certain other toxins are established causes of impaired neurodevelopment.
- Prematurity and birth weight, infections, and complications of pregnancy.
- The early environment after birth — nutrition, stimulation, language exposure, schooling, and socioeconomic circumstances powerfully shape measured ability, and these are easy to confuse with the effect of any one prenatal factor.
Because so many of these travel together — a disadvantaged pregnancy may involve poorer diet, more stress, and more exposures all at once — untangling the specific contribution of iodine is genuinely hard, which is why the best studies work so carefully to adjust for the others. So the honest framing is this: a slightly delayed talker or a child who struggles with reading is not evidence that the mother was iodine-deficient. The vast majority of such children have nothing to do with iodine. What the evidence does show is that, across populations, ensuring adequate iodine removes one preventable cause from that long list — and it happens to be one of the cheapest and easiest to fix.
When to Suspect Iodine Is the Problem
Because the effect on a child is invisible and non-specific, iodine deficiency in pregnancy is almost never identified by spotting a symptom in the baby. Instead, it is anticipated and prevented based on the mother's circumstances. The situations that should raise concern — and prompt attention to iodine intake ideally before conception — include:
- A diet low in iodine's main sources. Iodine in the food supply comes largely from dairy, eggs, seafood, and iodized salt. Women who consume little or no dairy and seafood are at clear risk — which is why strict vegan and most plant-based diets are a recognized risk factor unless iodine is deliberately supplemented.
- Not using iodized salt. Much of the salt people actually eat today comes from processed and restaurant food, which generally is not made with iodized salt; and fashionable specialty salts (sea salt, Himalayan pink salt, kosher salt) typically contain little or no iodine. A diet built on these can leave a real gap.
- Pregnancy or breastfeeding itself — both sharply raise iodine requirements, so a borderline-adequate intake that was fine before can become inadequate.
- Living in a historically iodine-poor region — inland and mountainous areas with iodine-depleted soils, where iodized salt programs are weak, still harbor genuine deficiency.
- Signs of low thyroid function in the mother — a new goiter, or symptoms of hypothyroidism, can be a clue, though deficiency frequently exists without them.
The practical takeaway is that the right time to act is not when a worry arises about the child — it is before and during pregnancy, by making sure iodine intake is adequate. Prevention is the only effective tool, because there is no treatment after the fact.
Why Pregnant Women Run Low
Iodine deficiency in pregnancy is fundamentally a mismatch between a sharply increased need and an often-shrinking supply. Several forces push in that direction:
- The demand jumps. A pregnant woman's thyroid must make roughly 50% more hormone, and the kidneys excrete more iodine in pregnancy, and the fetus and placenta take their share. International guidance therefore sets the recommended iodine intake higher in pregnancy (about 220–250 µg per day, versus roughly 150 µg for other adults).
- The supply has quietly fallen in some places. In several wealthy countries iodine intakes have drifted down over recent decades — partly because of reduced use of iodized salt at home, partly because the food industry largely uses non-iodized salt, and partly through changes in dairy practices that once incidentally boosted milk's iodine content. The result is that mild deficiency has re-emerged in populations that had been considered iodine-sufficient.
- Specialty salts and processed food. As noted above, the move toward sea salt and gourmet salts — which are not iodized — and the fact that most dietary salt is now hidden in processed foods made without iodized salt, both erode a source people assume is covering them.
- Restrictive diets. Vegan, dairy-free, and some low-salt eating patterns can leave a substantial iodine gap during pregnancy unless intake is planned.
- Goitrogens, in context. Certain foods (raw cruciferous vegetables, soy, cassava) contain compounds that can mildly interfere with iodine uptake. In a well-nourished person eating normal amounts this is not a real concern; it matters mainly when iodine intake is already marginal.
It is worth underscoring that this is rarely a problem of one missed meal. It reflects a habitual pattern of low intake colliding with the extra demand of pregnancy — which is precisely why it is best addressed by establishing good iodine intake as a steady habit before conception rather than reacting once pregnant.
Getting Tested: A Hard Thing to Measure
One of the frustrations of iodine status is that it is genuinely difficult to measure in an individual. Iodine is not stored the way iron or vitamin D is, and there is no simple, reliable blood test that tells one pregnant woman whether her iodine intake is adequate. This surprises people, but it shapes everything about how the problem is managed.
- Urinary iodine is the standard measure — most iodine eaten is excreted in the urine, so urinary iodine concentration reflects recent intake. But it varies enormously from day to day and even hour to hour depending on the last meal. For that reason, urinary iodine is excellent for assessing the iodine status of populations (using the median value from many people) but unreliable for judging a single individual from a single sample.
- Thyroid function tests — TSH, free T4, and sometimes thyroglobulin — do not measure iodine directly, but they assess how well the thyroid is keeping up, which is ultimately what matters for the baby. A thyroid panel is the practical test that a clinician will use in pregnancy to detect overt or subclinical hypothyroidism that needs treatment, and thyroid antibodies can identify autoimmune thyroid disease such as Hashimoto's. (A routine comprehensive metabolic panel does not include thyroid or iodine measures, so it does not address this question.)
The bottom line is that, because individual iodine testing is impractical, the medical approach is not to test-then-treat but to ensure adequate intake for everyone who is pregnant or planning pregnancy — the same logic that underlies recommending folic acid universally rather than testing each woman's folate. Thyroid function testing is used to catch and treat the thyroid problems that genuinely respond to treatment in pregnancy, following guidelines such as the American Thyroid Association's.
Getting Enough — Before and During Pregnancy
The encouraging part of this otherwise sobering subject is that prevention is cheap, simple, and highly effective. The goal is steady, adequate iodine intake established before conception and maintained through pregnancy and breastfeeding — not a last-minute correction.
Food first. For most people, ordinary foods can supply enough iodine:
- Dairy — milk and yogurt are among the most reliable everyday sources in many countries.
- Eggs — eggs (the yolk) provide a useful amount.
- Seafood — ocean fish such as cod and other white fish are rich in iodine; shellfish too. (See also the broader list on salmon and other fish pages.)
- Iodized salt — using iodized table salt (rather than non-iodized specialty salts) at home is a simple way to close the gap. Note that pregnancy is not the time to eat large amounts of salt for iodine's sake — the point is to choose iodized when you do use salt.
- Seaweed — a caution, not a recommendation. Seaweed (especially kelp) is extraordinarily iodine-rich, so much so that its content is wildly variable and a single serving can deliver many times the safe upper limit. Because too much iodine can itself disturb the thyroid, kelp and high-dose seaweed are best avoided as a deliberate iodine source in pregnancy.
Supplements — the practical safety net. Because so many women fall short, several professional bodies (including the American Thyroid Association) recommend that women who are pregnant, breastfeeding, or planning pregnancy take a daily supplement containing iodine — commonly 150 µg of iodine, usually as potassium iodide, as part of a prenatal vitamin. A few important caveats: not all prenatal vitamins actually contain iodine, so it is worth checking the label; the supplement should be a modest physiologic dose, since megadoses are harmful; and women with known thyroid disease should coordinate iodine intake with the clinician managing their thyroid, because the right amount can differ.
What cannot be done. The hard truth that runs through this whole topic bears repeating here: this is about prevention, not repair. Iodine given to a child after birth does not undo brain development that was shaped by a deficient pregnancy. That is exactly why the emphasis falls so heavily on getting it right ahead of time. For more on iodine's role in the developing brain, see iodine for brain development.
When to Seek Care
This is a topic best handled proactively with a clinician rather than urgently, but some situations clearly warrant a conversation with a doctor or midwife — ideally before or early in pregnancy:
- You are pregnant, breastfeeding, or planning pregnancy and are unsure whether your diet and prenatal vitamin provide enough iodine — ask, and check whether your prenatal contains iodine.
- You follow a vegan, dairy-free, or seafood-free diet, or do not use iodized salt — flag this specifically, as it is a recognized risk factor that is easy to address.
- You have a known thyroid condition — including hypothyroidism, Hashimoto's thyroiditis, Graves' disease, a goiter, or a past thyroid surgery — because your iodine and thyroid-hormone needs in pregnancy require individual management.
- You develop new neck swelling, marked fatigue, or other symptoms of an underactive thyroid in pregnancy — these deserve a thyroid panel, since treatable maternal hypothyroidism (from any cause) also affects the baby.
- Do not self-prescribe high-dose iodine or kelp/seaweed supplements in pregnancy. More is not better — excess iodine can suppress the fetal thyroid and cause harm. Stick to the recommended ~150 µg physiologic dose unless a clinician advises otherwise.
The reassuring message is that the action here is gentle and entirely preventive: a suitable prenatal vitamin and a sensible diet handle it for the great majority of women. The reason to raise it early is simply that the one thing no one can do is fix it afterward.
Key Research Papers
- Zimmermann MB, Jooste PL, Pandav CS (2008). Iodine-deficiency disorders. The Lancet;372(9645):1251-1262. — DOI: 10.1016/S0140-6736(08)61005-3
- Zimmermann MB (2009). Iodine Deficiency. Endocrine Reviews;30(4):376-408. — DOI: 10.1210/er.2009-0011
- Zimmermann MB (2012). The Effects of Iodine Deficiency in Pregnancy and Infancy. Paediatric and Perinatal Epidemiology;26(Suppl 1):108-117. — DOI: 10.1111/j.1365-3016.2012.01275.x
- Bath SC, Steer CD, Golding J, Emmett P, Rayman MP (2013). Effect of inadequate iodine status in UK pregnant women on cognitive outcomes in their children: results from the Avon Longitudinal Study of Parents and Children (ALSPAC). The Lancet;382(9889):331-337. — DOI: 10.1016/S0140-6736(13)60436-5
- Lazarus JH, Bestwick JP, Channon S, et al. (2012). Antenatal Thyroid Screening and Childhood Cognitive Function. New England Journal of Medicine;366(6):493-501. — DOI: 10.1056/NEJMoa1106104
- Velasco I, Carreira M, Santiago P, et al. (2009). Effect of Iodine Prophylaxis during Pregnancy on Neurocognitive Development of Children during the First Two Years of Life. The Journal of Clinical Endocrinology & Metabolism;94(9):3234-3241. — DOI: 10.1210/jc.2008-2652
- Bougma K, Aboud FE, Harding KB, Marquis GS (2013). Iodine and Mental Development of Children 5 Years Old and Under: A Systematic Review and Meta-Analysis. Nutrients;5(4):1384-1416. — DOI: 10.3390/nu5041384
- Skeaff SA (2011). Iodine Deficiency in Pregnancy: The Effect on Neurodevelopment in the Child. Nutrients;3(2):265-273. — DOI: 10.3390/nu3020265
- Abel MH, Caspersen IH, Meltzer HM, et al. (2017). Suboptimal Maternal Iodine Intake Is Associated with Impaired Child Neurodevelopment at 3 Years of Age in the Norwegian Mother and Child Cohort Study. The Journal of Nutrition;147(7):1314-1324. — DOI: 10.3945/jn.117.250456
- Pearce EN, Lazarus JH, Moreno-Reyes R, Zimmermann MB (2016). Consequences of iodine deficiency and excess in pregnant women: an overview of current knowns and unknowns. The American Journal of Clinical Nutrition;104(Suppl 3):918S-923S. — DOI: 10.3945/ajcn.115.110429
- Glinoer D (2007). Clinical and Biological Consequences of Iodine Deficiency during Pregnancy. Endocrine Development;10:62-85. — DOI: 10.1159/000106820
- Alexander EK, Pearce EN, Brent GA, et al. (2017). 2017 Guidelines of the American Thyroid Association for the Diagnosis and Management of Thyroid Disease During Pregnancy and the Postpartum. Thyroid;27(3):315-389. — DOI: 10.1089/thy.2016.0457
PubMed Topic Searches
- PubMed — Maternal iodine deficiency and child IQ / cognition
- PubMed — Iodine deficiency in pregnancy and neurodevelopment
- PubMed — Endemic cretinism and iodine deficiency
- PubMed — Iodine supplementation in pregnancy and infant cognitive outcome
- PubMed — Urinary iodine status in pregnant women
Connections
- Iodine Deficiency Symptom Hub
- Iodine Deficiency and Goiter
- Iodine Deficiency: Hypothyroidism & Fatigue
- Iodine Deficiency: Weight Gain & Cold
- Iodine Overview
- Iodine for Brain Development
- Iodine and Thyroid Function
- Hashimoto's Thyroiditis
- Thyroid Panel
- Comprehensive Metabolic Panel
- Selenium
- Iron
- Milk
- Yogurt
- Eggs
- Cod