Kale Oxalates, Goitrogens, and Cooking Decisions
Kale carries two anti-nutrient categories that periodically generate online controversy and clinical questions — oxalates (the precursor to calcium-oxalate kidney stones) and goitrogenic glucosinolate metabolites (thiocyanates that compete with iodine for thyroid uptake). The headline numbers are reassuring on both fronts: kale's oxalate content is approximately 20 mg per 100 g raw, dramatically lower than spinach (~750 mg per 100 g raw) and well within the safe range for the vast majority of consumers including most calcium-oxalate stone formers. The goitrogenic effect is similarly modest, clinically significant only in individuals with concurrent iodine deficiency — a vanishingly rare condition in the United States given universal salt iodization. The interesting practical question is not "is kale safe?" but "how should I cook it to optimize the trade-off between bioactive yield (preserve glucosinolates, enable myrosinase activation) and anti-nutrient reduction (lower oxalate leaching, mineral preservation)?" This deep-dive walks through the oxalate quantitation, the kidney-stone literature, the goitrogen biochemistry, the cooking-method comparison (raw vs blanched vs steamed vs sauteed vs boiled), and the practical raw-vs-cooked decision tree for different clinical contexts.
Table of Contents
- Kale Oxalate Content vs Other Greens
- How Dietary Oxalate Becomes a Kidney Stone
- Who Should Limit Kale (and Who Should Not)
- The Goitrogen Mechanism: Thiocyanate and Iodine Competition
- Clinical Relevance for Thyroid Health
- Cooking Method Effects: Raw vs Blanched vs Steamed vs Sauteed vs Boiled
- Nutrient Preservation Across Cooking Methods
- The Daily Green Smoothie Question
- Raw vs Cooked Decision Tree
- Cautions and Special Populations
- Key Research Papers
- Connections
- Featured Videos
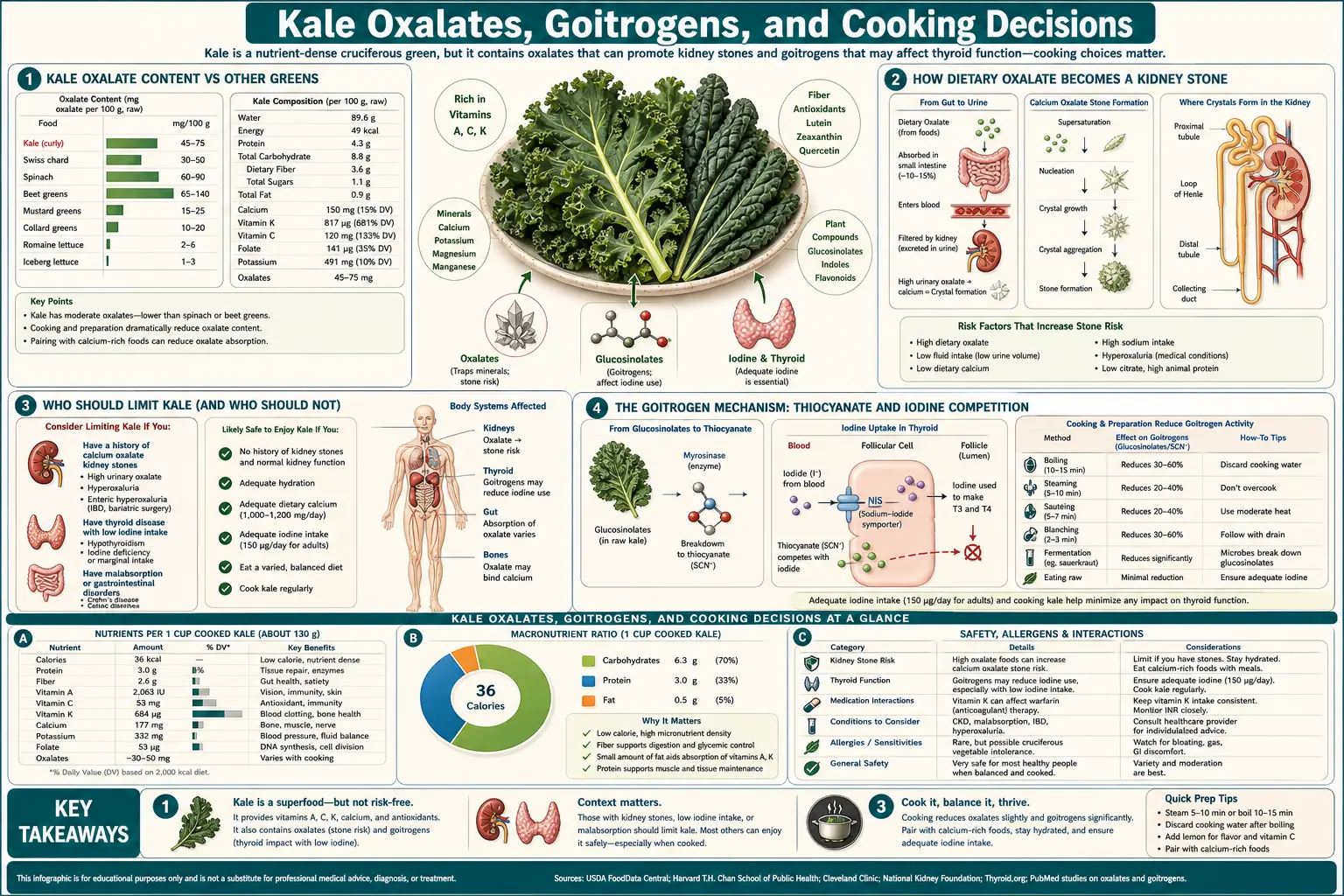
Kale Oxalate Content vs Other Greens
Oxalate (also written as oxalic acid in its protonated form) is a small dicarboxylic acid that occurs naturally in many plant foods, where it functions as a calcium-regulation molecule, a calcium-storage form (as insoluble calcium oxalate crystals in plant vacuoles), and a herbivore-deterrent (the gritty mouthfeel of high-oxalate plants). The dietary oxalate content varies dramatically across plant foods:
- Spinach, raw: 750 mg per 100 g (the dietary champion)
- Swiss chard, raw: 645 mg per 100 g
- Beet greens, raw: 610 mg per 100 g
- Rhubarb stalks: 500 mg per 100 g
- Star fruit (carambola): 380 mg per 100 g
- Almonds (whole, with skin): 122 mg per 100 g (high per gram but small typical portion)
- Cashews: 49 mg per 100 g
- Sweet potato: 30 mg per 100 g
- Kale, raw: 20 mg per 100 g — the headline number
- Collards: 17 mg per 100 g
- Broccoli, raw: 15 mg per 100 g
- Lettuces (romaine, iceberg, butter): 5-10 mg per 100 g
Kale is therefore in the low-oxalate-greens category, not the high-oxalate category. A typical one-cup raw serving of chopped kale (~67 g) delivers approximately 13 mg of oxalate — well below the 40-50 mg per meal threshold that constitutes a "high-oxalate meal" for risk-stratification in the kidney-stone literature.
The widespread idea that kale is a high-oxalate vegetable to be avoided is a misclassification carried over from spinach and Swiss chard concerns. The chemistry is genuinely different.
How Dietary Oxalate Becomes a Kidney Stone
The pathway from dietary oxalate to calcium-oxalate kidney stone involves several discrete steps, each with its own variability:
- Absorption — dietary oxalate is absorbed in the small intestine via specific oxalate transporters and by paracellular diffusion. Absorption ranges from less than 5% in the presence of high dietary calcium (which forms insoluble calcium oxalate in the gut and prevents absorption) to over 50% in low-calcium diets, dehydration, and certain gut conditions
- Plasma transport — absorbed oxalate enters the bloodstream and is filtered by the kidney glomerulus, with most filtered oxalate excreted into the urine
- Urinary supersaturation — if urinary oxalate concentration is high (typically >40 mg/day urinary oxalate) and urinary calcium is also high (typically >200 mg/day), the urine becomes supersaturated with respect to calcium oxalate, and crystallization becomes thermodynamically favored
- Crystal nucleation and growth — initial crystals form and grow into stones, particularly in regions of urinary stasis (renal calyces, ureteropelvic junction)
The classic risk-modification advice from the urology literature emphasizes step 1 (gut absorption) more than dietary intake reduction. Adequate dietary calcium (800-1200 mg/day) consumed with oxalate-containing meals reduces oxalate absorption by 30-50%. Adequate hydration (urine output >2.5 L/day) reduces urinary supersaturation. Magnesium and citrate intake reduce crystal formation. These factors are much more important than dietary oxalate restriction for most stone formers.
The Harvard cohort studies (Nurses' Health Study II, Health Professionals Follow-up Study) showed that dietary oxalate intake was only weakly associated with kidney stone risk, and the association disappeared after adjustment for calcium intake. Total intake matters less than the calcium-to-oxalate ratio at the level of individual meals.
Who Should Limit Kale (and Who Should Not)
Who can eat kale freely:
- Anyone without a history of calcium-oxalate kidney stones (the vast majority of the population)
- Calcium-oxalate stone formers consuming adequate dietary calcium (800-1200 mg/day) with meals, drinking 2.5+ liters of fluid daily, and consuming kale in normal portion sizes (one cup raw or cooked per meal)
- Patients with uric acid stones, cystine stones, or struvite stones — oxalate is not the issue for these stone types
Who should exercise moderation:
- Calcium-oxalate stone formers consuming low-calcium diets — they should fix the calcium gap first (with calcium-rich foods or calcium citrate supplementation taken with meals), not necessarily restrict oxalate
- Patients with active hyperoxaluria (urinary oxalate >40 mg/day) — comprehensive dietary oxalate evaluation with a renal dietitian is appropriate; this is the indication where kale portion size may need limits
- Patients with enteric hyperoxaluria from fat malabsorption (Crohn's disease, post-bariatric, short-bowel syndrome) — fat malabsorption produces excess intestinal free fatty acids that bind calcium and leave oxalate unbound and available for absorption. These patients can develop severe hyperoxaluria and benefit from oxalate restriction. The greens to limit are spinach, Swiss chard, and beet greens, not kale
- Patients with primary hyperoxaluria (rare genetic disorders of glyoxylate metabolism) — comprehensive oxalate restriction is part of standard management
For the typical health-conscious adult adding a daily cup of cooked kale to the diet, oxalate concerns are not relevant. The benefits from Vitamin K, lutein, glucosinolates, and the broader nutritional package vastly outweigh the modest oxalate load.
The Goitrogen Mechanism: Thiocyanate and Iodine Competition
The "goitrogen" label applied to cruciferous vegetables refers to the thiocyanate ion (SCN−) and the related compound goitrin (5-vinyl-2-oxazolidinethione), both of which are products of glucosinolate hydrolysis. Thiocyanate is a competitive inhibitor of the sodium-iodide symporter (NIS) at the thyroid follicular cell membrane — the transporter responsible for concentrating iodide from the blood into the thyroid for thyroid hormone synthesis. By competing with iodide for transport, thiocyanate reduces iodide uptake and, if sustained over long periods in iodine-deficient individuals, can produce goiter.
The historical context is important. Goiter from cruciferous-vegetable intake was documented in 19th and early 20th century European and Latin American populations consuming brassicas (cabbage, kale, kohlrabi) as a dietary staple in iodine-deficient soil regions. The condition resolved with iodine supplementation, not with cruciferous-vegetable restriction. Modern iodine sufficiency through universal salt iodization in the United States, Canada, and most developed countries has effectively eliminated dietary goiter as a public-health concern.
Goitrin (the thiouracil-like compound from progoitrin) is a more potent thyroid inhibitor than thiocyanate — it directly inhibits thyroid peroxidase (TPO), the enzyme that organifies iodide into thyroglobulin. Goitrin concentrations are high in rapeseed and certain wild brassicas but low in cultivated kale, broccoli, and brussels sprouts. Kale's contribution to dietary goitrin is minimal.
Clinical Relevance for Thyroid Health
For iodine-replete adults (most Americans): normal cruciferous-vegetable intake including daily kale has no measurable effect on thyroid function. Multiple randomized trials of high-dose cruciferous intake in iodine-sufficient subjects have shown no significant changes in TSH, free T3, free T4, or thyroid autoantibodies. The iodine sufficiency provides enough substrate that thiocyanate-mediated NIS inhibition is clinically irrelevant.
For iodine-deficient individuals: the calculation changes. Iodine deficiency is rare in the United States (CDC NHANES data show median urinary iodine concentration well above the WHO sufficiency threshold), but it can occur in specific populations:
- Strict vegans who avoid iodized salt, seaweed, dairy, and eggs (the major dietary iodine sources)
- Individuals on low-sodium or salt-restricted diets using non-iodized salt
- Pregnant women, who have approximately 50% higher iodine requirements than non-pregnant adults
- Some areas of mountainous interior regions globally where iodine deficiency persists despite supplementation programs
For these populations, ensuring adequate iodine intake (150 mcg/day for adults, 220 mcg/day in pregnancy, 290 mcg/day in lactation) is the appropriate intervention — not avoidance of cruciferous vegetables. A daily multivitamin containing 150 mcg of iodine, or routine use of iodized salt, or modest intake of iodine-rich foods (seaweed, dairy, eggs, fish), provides ample buffer against any cruciferous thiocyanate effect.
For patients with autoimmune thyroid disease (Hashimoto's thyroiditis, Graves' disease): normal cruciferous intake is safe. There is no evidence that cruciferous vegetables exacerbate autoimmune thyroid disease in iodine-sufficient populations. Some integrative-medicine clinicians have historically recommended cruciferous restriction for Hashimoto's patients, but this is not supported by rigorous evidence and may deprive the patient of meaningful nutritional benefit.
For patients on levothyroxine: consistent intake is more important than total amount. Take levothyroxine on an empty stomach 30-60 minutes before any food including kale; cruciferous vegetables do not specifically interfere with levothyroxine absorption beyond the general food-absorption interaction that applies to all foods.
For more on thyroid health, see our Hashimoto's Thyroiditis page.
Cooking Method Effects: Raw vs Blanched vs Steamed vs Sauteed vs Boiled
The cooking method substantially changes the nutrient and anti-nutrient profile of kale. Empirical data from multiple analytical chemistry studies (summarized in Conn-Goeke 2017, Vermeulen 2009, Verkerk 2009) yield approximate retention percentages relative to fresh raw:
- Raw chopped (control) — 100% vitamins, 100% minerals, 100% glucosinolates, 100% oxalates, 100% myrosinase activity, minimal carotenoid bioavailability (cell walls intact)
- Massaged raw (with oil and lemon) — 95-100% nutrient retention, plus partial cell-wall disruption increasing carotenoid bioavailability 2-3x. Glucosinolate hydrolysis begins immediately. Excellent compromise between palatability and bioactive yield
- Steamed 3-5 min — 85-95% Vitamin C retention, 80-90% B vitamin retention, 60-80% myrosinase activity (some thermal inactivation), 80-90% glucosinolate retention, minimal oxalate change, increased carotenoid bioavailability 3-4x. The pragmatic best-of-both-worlds method
- Sauteed 2-3 min with fat — 70-90% Vitamin C retention, 60-80% myrosinase inactivation but brief chopping-to-pan window allows isothiocyanate formation, 80-90% glucosinolate retention, increased carotenoid and lutein bioavailability 4-5x (fat boost). Excellent for lutein-focused use
- Boiled 5-10 min — 50-70% Vitamin C retention (substantial loss to water), 40-60% glucosinolate retention (substantial leaching), 30-50% myrosinase inactivation, 30-50% oxalate reduction (oxalate leaches into cooking water), 60-80% Vitamin K retention. Use the cooking water if possible (soup) to capture leached nutrients; discard the water for oxalate reduction in stone-formers
- Microwaved 1-2 min — comparable to brief steaming if covered with a small amount of water; longer microwaving inactivates myrosinase but preserves water-soluble nutrients better than boiling
- Slow-cooked or stewed (long duration) — minimal myrosinase activity, substantial glucosinolate loss to extended thermal exposure. Vitamin K largely preserved (heat-stable). Acceptable for soups and stews where the kale is one of several ingredients
For the typical eater optimizing across all the benefits, brief steaming or quick sauteing with a teaspoon of olive oil represents the best compromise: substantial nutrient retention, partial myrosinase preservation, dramatically improved carotenoid absorption, and a manageable cooking time.
Nutrient Preservation Across Cooking Methods
- Vitamin K1 (phylloquinone) — heat-stable; most cooking methods retain 90%+ of phylloquinone. Boiling produces some leaching loss
- Vitamin C (ascorbate) — the most heat-labile and water-soluble nutrient. Steaming preserves 85-95%; boiling 50-70%; sauteing 70-90%
- Lutein and zeaxanthin — heat-stable; cooking releases them from cell walls and dramatically increases bioavailability when consumed with fat
- Beta-carotene — heat-stable in moderate cooking; bioavailability increases substantially with cooking and fat
- Folate — heat-labile and water-soluble; steaming preserves better than boiling
- Calcium, magnesium, iron, potassium — mineral content largely preserved across cooking methods, with some leaching to water
- Glucosinolates — partially heat-labile; substantial leaching loss in boiling. Steaming and quick sauteing preserve 70-90%
- Myrosinase — the most heat-labile component; substantial loss above ~70°C. Brief steaming or quick sauteing preserves more than longer cooking
- Fiber — structurally preserved across all cooking methods
The Daily Green Smoothie Question
A daily kale-based green smoothie has become a popular health practice. Some considerations specific to this preparation:
- Volume matters — a smoothie can easily incorporate 100-150 g of raw kale (one and a half to two full cups), 5-7x the per-meal serving from a salad or cooked side dish. The oxalate load per smoothie is approximately 20-30 mg — still below the high-oxalate-meal threshold, but worth tracking if multiple servings per day are consumed
- Blender mechanical disruption — the high-shear blending action fully ruptures plant cell walls and initiates complete glucosinolate-myrosinase contact. This yields more bioactive isothiocyanate per gram of kale than slow chewing of intact leaves. Excellent for sulforaphane delivery
- Combine with calcium — pairing the smoothie with a calcium source (Greek yogurt, milk, fortified plant milk) helps bind oxalate in the gut and reduce absorption
- Vary the greens — rotating kale with romaine, baby spinach, parsley, cilantro, or arugula provides phytochemical diversity and limits any single anti-nutrient load. Daily large-volume spinach smoothies are the more legitimate oxalate concern, not kale
- Add fat — a tablespoon of avocado, coconut oil, MCT oil, almond butter, or chia seeds dramatically improves carotenoid and Vitamin K absorption from the smoothie
- Pre-existing kidney-stone history — multi-cup daily green smoothies may not be appropriate. Discuss with the urology team and consider 24-hour urinary oxalate testing if there is concern
Raw vs Cooked Decision Tree
The pragmatic decision framework for the question "should I eat kale raw or cooked?":
- Optimizing for lutein and carotenoid absorption (eye health) → lightly cooked (steamed or sauteed) with a teaspoon of fat, ideally per the AREDS2 target of 10+ mg lutein per day
- Optimizing for Vitamin K and bone health → either raw or lightly cooked with fat; K is heat-stable and absorbs efficiently with dietary fat regardless of cooking. Consistency of intake matters more than method, especially on warfarin
- Optimizing for sulforaphane and glucosinolate-derived chemoprevention → raw (chopped and rested 5-10 min) OR briefly cooked with chopped raw added at the end OR cooked with a sprinkle of mustard seed powder to provide exogenous myrosinase
- Vitamin C and folate maximum retention → raw or briefly steamed; avoid prolonged boiling
- Reducing oxalate load (in stone-formers) → brief boiling and discarding the cooking water reduces oxalate by 30-50%. For typical consumers this trade-off is not necessary
- Digestive tolerance — some people experience bloating, gas, or gut discomfort with large raw kale portions due to the fiber and FODMAP content (kale contains modest levels of fructans). Lightly cooking softens fiber and may improve tolerance
- Children — cooked kale is generally more palatable and easier to chew than raw. The bioactive benefits remain substantial when prepared with fat
The single-best default for most adults: chop kale, let it sit 5-10 minutes, steam or quick-saute in olive oil for 3-5 minutes, dress with lemon juice and a pinch of salt. This captures most of the bioactive benefits across all the relevant pathways with minimal trade-offs.
Cautions and Special Populations
- Active calcium-oxalate kidney stone disease — consult the urology team. In most cases, the recommendation is normal dietary calcium plus adequate hydration, not oxalate restriction. Kale is rarely the problem; spinach and beet greens more often are
- Hyperoxaluria from gut conditions (Crohn's, post-bariatric, short-bowel) — comprehensive oxalate management is appropriate; work with a renal dietitian. Kale's low oxalate makes it usually fine
- Iodine deficiency (rare in U.S.) — ensure 150 mcg/day iodine intake (iodized salt, multivitamin, seaweed, dairy); cruciferous restriction is not the answer
- Active hypothyroidism on levothyroxine — consistent kale intake is fine; take levothyroxine 30-60 min before food
- Warfarin therapy — covered on the Vitamin K page. Consistency, not avoidance
- Pregnancy — kale is appropriate in pregnancy; ensure adequate iodine intake (220 mcg/day recommended) through prenatal vitamin and iodized salt
- Pediatric population — cooked kale prepared with fat is appropriate from approximately 8-9 months of age (one of the later greens introduced due to texture). Avoid raw kale in young children due to choking and FODMAP concerns
- Brassica allergy — rare but real; mugwort-mustard cross-reactivity syndrome is the best-documented variant. Symptoms include oral itching, swelling, and (rarely) systemic reactions. Discontinue and consult an allergist if suspected
Key Research Papers
- Noonan SC, Savage GP (1999). Oxalate content of foods and its effect on humans. Asia Pacific Journal of Clinical Nutrition. PMID: 24393738 — PubMed 24393738
- Curhan GC, Willett WC, Knight EL, Stampfer MJ (2004). Dietary factors and the risk of incident kidney stones in younger women: Nurses' Health Study II. Archives of Internal Medicine. PMID: 15037495 — Search PubMed
- Taylor EN, Curhan GC (2007). Oxalate intake and the risk for nephrolithiasis. Journal of the American Society of Nephrology. PMID: 17715407 — Search PubMed
- Borghi L, Schianchi T, Meschi T, Guerra A, Allegri F, Maggiore U, Novarini A (2002). Comparison of two diets for the prevention of recurrent stones in idiopathic hypercalciuria. NEJM. PMID: 11784873 — PubMed 11784873
- Felker P, Bunch R, Leung AM (2016). Concentrations of thiocyanate and goitrin in human plasma, their precursor concentrations in brassica vegetables, and associated potential risk for hypothyroidism. Nutrition Reviews. PMID: 26946249 — PubMed 26946249
- Verkerk R, Schreiner M, Krumbein A, Ciska E, Holst B, Rowland I, De Schrijver R, Hansen M, Gerhauser C, Mithen R, Dekker M (2009). Glucosinolates in Brassica vegetables: the influence of the food supply chain on intake, bioavailability and human health. Molecular Nutrition & Food Research. PMID: 19035551 — Search PubMed
- Vermeulen M, Klopping-Ketelaars IW, van den Berg R, Vaes WH (2008). Bioavailability and kinetics of sulforaphane in humans after consumption of cooked versus raw broccoli. Journal of Agricultural and Food Chemistry. PMID: 18950181 — PubMed 18950181
- Conaway CC, Getahun SM, Liebes LL, Pusateri DJ, Topham DK, Botero-Omary M, Chung FL (2000). Disposition of glucosinolates and sulforaphane in humans after ingestion of steamed and fresh broccoli. Nutrition and Cancer. PMID: 11341044 — Search PubMed
- Leung AM, Pearce EN, Braverman LE (2011). Iodine nutrition in pregnancy and lactation. Endocrinology and Metabolism Clinics of North America. PMID: 22122876 — Search PubMed
- Holst B, Williamson G (2008). Nutrients and phytochemicals: from bioavailability to bioefficacy beyond antioxidants. Current Opinion in Biotechnology. PMID: 18387293 — Search PubMed
- Liebman M, Murphy S (2007). Low oxalate bioavailability from black tea. Nutrition Research. PubMed: Oxalate bioavailability
- Holmes RP, Goodman HO, Assimos DG (2001). Contribution of dietary oxalate to urinary oxalate excretion. Kidney International. PMID: 11231356 — Search PubMed
PubMed Topic Searches
- PubMed: Dietary oxalate and kidney stones
- PubMed: Cruciferous and thyroid
- PubMed: Cooking and vitamin retention
- PubMed: Myrosinase heat inactivation
- PubMed: Enteric hyperoxaluria
Connections
- Kale (Main Page)
- Kale Benefits Hub
- Kale, Vitamin K and Bone
- Kale, Lutein, and Eye Health
- Kale Glucosinolates and Cancer
- Kidney Stones
- Hashimoto's Thyroiditis
- Hypothyroidism
- Iodine
- Calcium
- Magnesium
- Spinach (Higher Oxalate)
- Broccoli
- Brussels Sprouts
- Sulforaphane
- Vitamin K