Spinach Iron Absorption and Oxalates
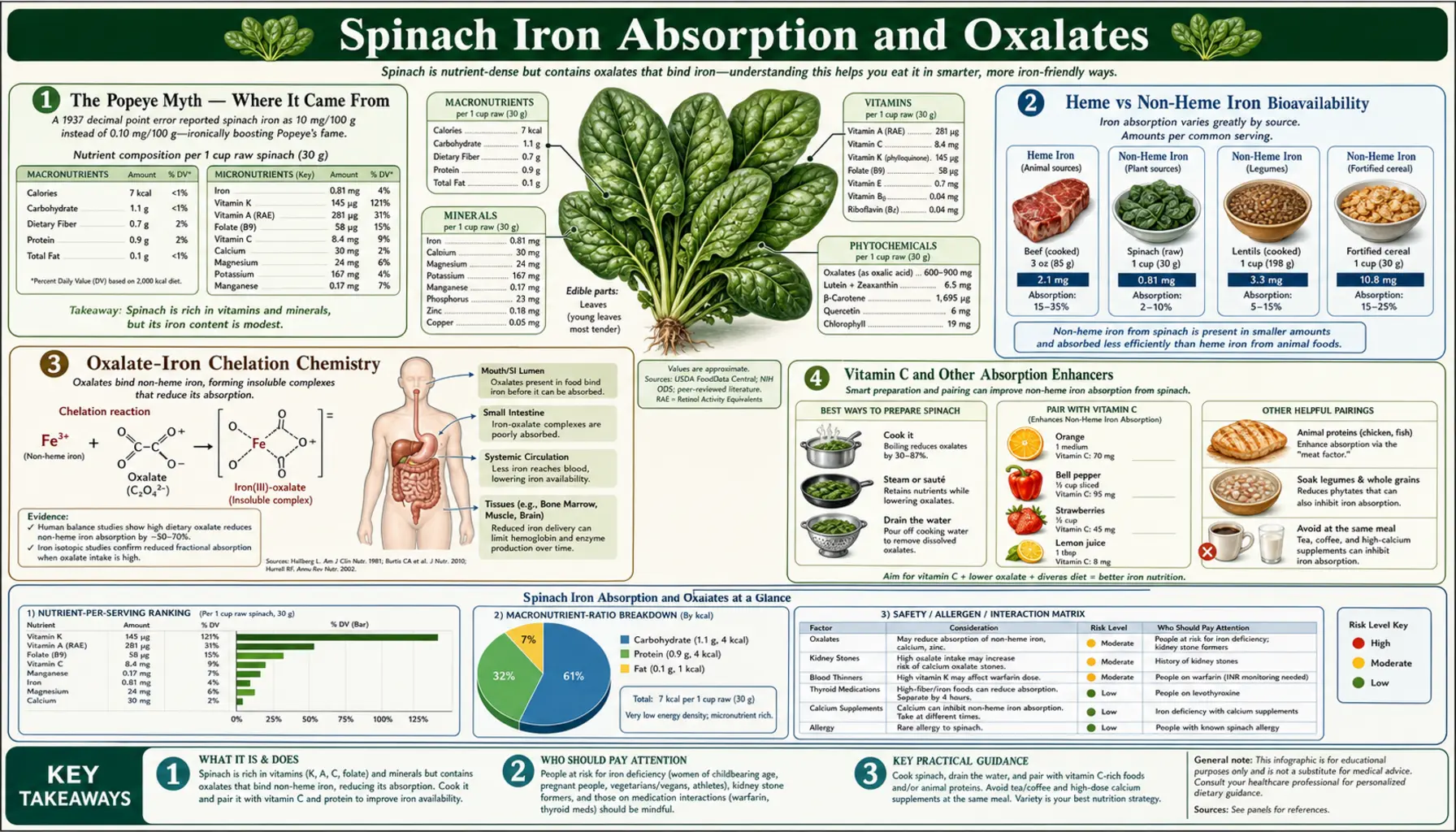
The Popeye image of spinach as iron-rich superfood is one of the most persistent nutrition myths. Spinach does contain non-heme iron at 2.7 mg per 100 g cooked — respectable in absolute terms — but the high oxalate content (750-1,500 mg per 100 g raw) chelates most of that iron into insoluble iron-oxalate complexes that pass through the gut unabsorbed. Real-world bioavailability is approximately 2%, compared to 15-35% for heme iron from red meat and 5-12% for non-heme iron from less-oxalate-rich foods. Vitamin C co-ingestion can roughly double spinach iron absorption by reducing ferric iron to the more absorbable ferrous form. Beyond the iron question, the same oxalate is the substrate for calcium oxalate kidney stones in susceptible individuals — the most common kidney stone type, affecting up to 10% of the population. This page covers the chemistry, the kidney stone risk, the cooking-based oxalate reduction strategies, and the practical implications for both iron-deficient patients and oxalate-sensitive patients.
Table of Contents
- The Popeye Myth — Where It Came From
- Heme vs Non-Heme Iron Bioavailability
- Oxalate-Iron Chelation Chemistry
- Vitamin C and Other Absorption Enhancers
- Kidney Stones — The Oxalate Concern
- Cooking Methods That Reduce Oxalate
- The Calcium-Oxalate Trade-Off
- If You Have Iron Deficiency
- If You Are Oxalate-Sensitive
- Key Research Papers
- Connections
- Featured Videos
The Popeye Myth — Where It Came From
The cultural image of spinach as iron-rich superfood dates to the 1929 Popeye cartoon strip, which made spinach the source of the sailor's super-strength. The Popeye character was credited by mid-century nutritionists with single-handedly increasing U.S. spinach consumption by 33% during the 1930s, an early case study in popular media influence on dietary habits.
The persistent (but largely apocryphal) story is that the 1870 Wolff analysis of spinach iron content contained a decimal-point error, reporting 35 mg iron per 100 g instead of the correct 3.5 mg, and that this exaggerated figure persisted in nutrition textbooks until the 1930s, was used by E.C. Segar in creating the Popeye character, and the myth survived even after the error was corrected. Subsequent historical detective work suggests the decimal-error story is itself partially a myth — the 35 mg figure may have referred to dry-weight rather than fresh-weight content (which would have been roughly correct), or to a different chemical analysis entirely.
The substantive truth, regardless of the origin myth, is that spinach iron content per gram is respectable but the iron is poorly absorbed. Per the USDA FoodData Central database:
- Spinach, raw — 2.7 mg iron per 100 g
- Spinach, cooked, boiled, drained — 3.6 mg iron per 100 g (concentrated because water is removed)
- Spinach, canned — 2.3 mg iron per 100 g
For comparison:
- Beef liver — 6.5 mg heme iron per 100 g (much higher bioavailability)
- Beef chuck — 2.8 mg heme iron per 100 g
- Oysters — 7.8 mg iron per 100 g
- Lentils — 3.3 mg non-heme iron per 100 g
- Tofu — 2.7 mg non-heme iron per 100 g
- Pumpkin seeds — 8.8 mg non-heme iron per 100 g
The numerical iron content of spinach is in the same range as lentils, tofu, and beef chuck — respectable but not extraordinary. The catch is that the bioavailable fraction (the iron actually absorbed and used) is much lower for spinach than for any of those comparisons because of the oxalate chelation effect described below.
Heme vs Non-Heme Iron Bioavailability
Dietary iron exists in two distinct chemical forms with very different absorption mechanisms:
- Heme iron — iron bound in the heme prosthetic group of hemoglobin and myoglobin, present only in animal flesh. Absorbed intact via the heme carrier protein 1 (HCP1) in the duodenal enterocyte and then released from the porphyrin ring inside the cell by heme oxygenase. Bioavailability is 15-35% depending on iron status, dietary co-factors, and the meat source.
- Non-heme iron — ionic iron (Fe³+ or Fe²+) bound to various dietary ligands. Must be reduced from ferric (Fe³+) to ferrous (Fe²+) by the duodenal cytochrome b reductase (DCYTB) before absorption via the divalent metal transporter 1 (DMT1). Bioavailability ranges from 1-25% depending heavily on dietary co-factors and inhibitors. Found in plant foods, dairy, and fortified grains.
Spinach iron is non-heme iron, and within the non-heme iron category it has one of the lowest bioavailability rates of any common food. The Hallberg and Hulthen 2000 algorithm for predicting dietary iron absorption assigns spinach a "high-inhibitor" score because of the oxalate content. Their model predicts approximately 1-3% absorption from spinach in the typical mixed-diet context, compared to 5-12% for non-heme iron in low-inhibitor foods (cooked lentils, tofu, fortified cereal).
The key implications:
- Spinach is not a reliable treatment for iron deficiency. Patients with iron-deficiency anemia who try to correct it through spinach consumption alone will not see meaningful improvement in ferritin or hemoglobin.
- For iron deficiency, the rank order of dietary effectiveness is: heme iron from red meat > iron supplements > non-heme iron from low-inhibitor foods (lentils, pumpkin seeds, fortified cereal) with vitamin C >> non-heme iron from high-oxalate greens.
- Vegan and vegetarian patients at risk of iron deficiency need to actively manage iron intake through low-oxalate, high-bioavailability plant sources (lentils, pumpkin seeds, fortified products) plus vitamin C co-ingestion, rather than relying on greens.
- Spinach can still contribute incidentally to iron intake in a mixed diet but should not be counted on for iron-deficiency correction.
Oxalate-Iron Chelation Chemistry
Oxalate (oxalic acid, C&sub2;H&sub2;O&sub4;) is a small dicarboxylic acid produced by many plants as a defense compound and as a calcium-regulating metabolite. Spinach, beet greens, rhubarb, Swiss chard, almonds, and a few other foods are particularly high in oxalate.
The chemistry of oxalate-mineral interaction is that the two carboxylate groups can chelate divalent metal cations to form insoluble or poorly absorbed complexes. Calcium oxalate (the substance of most kidney stones) is the most familiar example, but oxalate also forms similar complexes with iron (iron oxalate), magnesium, and zinc:
- Calcium oxalate (CaC&sub2;O&sub4;) — the most common chelation product because dietary calcium is typically the highest divalent cation concentration in the gut. Highly insoluble at physiologic pH; precipitates in the gut and passes in stool. This is actually beneficial for kidney stone prevention because it reduces dietary oxalate absorption.
- Iron oxalate (FeC&sub2;O&sub4;) — insoluble at the alkaline pH of the small intestine where non-heme iron is absorbed. Most spinach iron is bound as iron oxalate by the time it reaches the absorptive duodenum, and passes through the gut unabsorbed.
- Magnesium oxalate — somewhat more soluble than calcium oxalate but still reduces magnesium bioavailability from oxalate-rich foods.
The Holloway 2007 study quantified the practical effect on calcium absorption from spinach. Fractional calcium absorption from milk (low oxalate) was 27%; from spinach (high oxalate) was only 5%. Despite spinach's 136 mg calcium per 100 g cooked appearing on nutrition labels, the bioavailable calcium is approximately 7 mg per 100 g — trivial compared to milk or fortified plant milks.
The Heaney and Weaver 1989 AJCN study performed isotope-labeled calcium absorption studies and reached similar conclusions: spinach calcium is functionally unabsorbable; the calcium in nutrition tables for spinach should not be counted toward daily calcium intake.
The same logic applies to spinach iron and to a lesser extent spinach magnesium. The presence of iron and calcium on the spinach nutrition label is technically accurate (the minerals are present in the leaf tissue) but functionally misleading for the consumer trying to use spinach for those nutrients.
Vitamin C and Other Absorption Enhancers
The single most effective intervention for boosting non-heme iron absorption from spinach (or any non-heme source) is co-ingestion with vitamin C. Ascorbic acid:
- Reduces ferric (Fe³+) iron to the more absorbable ferrous (Fe²+) form in the duodenum, partially bypassing the DCYTB reductase rate-limiting step.
- Chelates iron in a soluble ascorbate-iron complex that competes with oxalate for binding the iron, increasing the soluble iron fraction reaching the enterocyte brush border.
- Reduces the pH of the gut content, increasing iron solubility (most relevant in the proximal duodenum where pH transition from acidic stomach to alkaline jejunum occurs).
The Cook and Reddy 2001 AJCN study quantified the effect: addition of 50-100 mg ascorbic acid to a meal approximately doubled non-heme iron absorption. The effect is dose-related up to about 200 mg vitamin C per meal, with diminishing returns above that.
Practical spinach pairings for iron absorption:
- Spinach + lemon juice — one tablespoon lemon juice contains ~7 mg vitamin C; squeeze over a spinach salad or sauteed spinach.
- Spinach + tomatoes — ~14 mg vitamin C per medium tomato; spinach in marinara sauce or a Greek salad with tomato.
- Spinach + bell peppers — 80-150 mg vitamin C per cup; a spinach stir-fry with bell peppers.
- Spinach + orange juice — 124 mg vitamin C per cup; spinach smoothie with orange.
- Spinach + strawberries — 85 mg vitamin C per cup; spinach-strawberry salad.
- Spinach + beef — the "meat factor" enhances non-heme iron absorption even without vitamin C; spinach as a side to a meat dish, or spinach mixed into ground beef preparations.
Inhibitors to avoid in the same meal: coffee, tea, red wine (tannins), high-calcium dairy (which can compete with iron for absorption), bran cereal (phytate). The Hurrell 1999 study showed that a cup of black tea with a meal can reduce non-heme iron absorption by 75-94%.
Kidney Stones — The Oxalate Concern
Calcium oxalate stones account for approximately 70-80% of all kidney stones — the most common kidney stone type, affecting roughly 10% of the U.S. adult population at some point in life. The recurrence rate after a first stone is approximately 50% within 10 years.
Dietary oxalate is one of several contributors to urinary oxalate excretion, which in turn is a primary determinant of calcium oxalate stone risk. Other contributors include:
- Endogenous oxalate production — the liver produces oxalate as a metabolite of glycine, glyoxylate, hydroxyproline, and vitamin C metabolism. Endogenous production is typically the larger contributor to urine oxalate than dietary intake in most people.
- Dietary oxalate absorption — typically 5-15% of dietary oxalate is absorbed; the rest is bound in the gut by calcium and excreted in stool.
- Calcium intake (paradoxical) — LOW dietary calcium increases urinary oxalate by reducing the gut binding of dietary oxalate. The Curhan 1996 NEJM Nurses Health Study famously showed that higher dietary calcium intake REDUCED kidney stone risk — opposite to the old recommendation to restrict calcium in stone formers.
- Hyperabsorption — some individuals (about 20% of recurrent calcium oxalate stone formers) have enhanced intestinal oxalate absorption, possibly related to Oxalobacter formigenes gut microbiota depletion (this bacterium degrades dietary oxalate in the colon).
- Inflammatory bowel disease and Roux-en-Y bypass — both increase oxalate absorption and produce "enteric hyperoxaluria" with markedly elevated stone risk.
The practical implication for spinach consumers: in the general population without a history of calcium oxalate stones, moderate spinach intake (1-2 servings per day) is not a significant kidney stone risk factor, particularly when consumed with adequate dietary calcium that binds the oxalate in the gut. For individuals with a history of calcium oxalate stones, the standard urology recommendation is to limit very-high-oxalate foods (spinach, rhubarb, beet greens, almonds, peanuts, dark chocolate) and to maintain adequate dietary calcium intake (1,000-1,200 mg/day) at the same meals as oxalate-containing foods.
The Curhan 2014 follow-up analysis estimated that high spinach intake increased kidney stone risk in stone formers but had minimal effect in the general population. The Taylor 2008 CJASN study quantified the dose-response of dietary oxalate to urinary oxalate excretion and found that even high spinach intake produced only a modest absolute increase in urinary oxalate when dietary calcium was adequate.
Cooking Methods That Reduce Oxalate
The Chai and Liebman 2005 Journal of Agricultural and Food Chemistry study systematically tested cooking methods for oxalate reduction in spinach and other oxalate-rich vegetables. Results for spinach:
- Raw spinach (control) — 100% soluble oxalate retention
- Steaming — minimal oxalate reduction (5-15%)
- Boiling (10 min, water discarded) — 30-87% reduction in soluble oxalate depending on water volume
- Boiling in large water volume + discard — maximum oxalate reduction; the soluble oxalate dissolves into the cooking water and is poured off
- Blanching (brief immersion in boiling water, then drained) — 30-50% reduction
The critical distinction is between SOLUBLE oxalate (the absorbable, kidney-stone-relevant fraction) and TOTAL oxalate. Cooking does not destroy the oxalate molecule chemically — it dissolves the soluble fraction into the cooking water. If the cooking water is consumed (as in soup or stew), the total oxalate burden on the consumer is unchanged. Only when the water is discarded does the consumer benefit from the oxalate reduction.
This is why traditional Italian preparations of spinach typically blanch the spinach in boiling water and discard the water before sauteing in olive oil and garlic — the technique is centuries old, predating modern oxalate chemistry, but produces a measurable oxalate reduction.
Practical preparation for oxalate-sensitive individuals:
- Bring a large pot of water to a rolling boil.
- Add spinach (or other oxalate-rich greens) and boil for 1-3 minutes until just wilted.
- Drain in a colander; press out as much water as possible.
- Discard the cooking water (do NOT use it for soup or stock).
- Saute the blanched spinach briefly in olive oil with garlic, or use it in dishes that don't depend on cooking liquid.
The trade-off, as discussed in our Cooking vs Raw deep-dive, is that this method also leaches out water-soluble vitamins (folate, vitamin C, B vitamins) which are lost with the discarded water. For folate retention, steaming is preferred; for oxalate reduction, boiling-and-discarding is preferred. There is no single perfect method; the right answer depends on which nutrient or risk factor is most relevant to the individual.
The Calcium-Oxalate Trade-Off
One of the more counterintuitive findings in kidney stone research is that adequate dietary calcium REDUCES rather than increases calcium oxalate stone risk. The mechanism is competitive binding in the gut:
- When dietary calcium and dietary oxalate are consumed at the same meal, the calcium binds the oxalate in the gut to form insoluble calcium oxalate, which precipitates and passes in stool.
- The result is reduced absorption of BOTH the calcium AND the oxalate — both end up in the stool rather than the bloodstream and urine.
- Conversely, low-calcium diets allow more dietary oxalate to be absorbed unbound, leading to higher urinary oxalate excretion and higher calcium oxalate stone risk.
The Curhan 1996 NEJM Nurses Health Study followed 91,731 women over 12 years and found that the highest quintile of dietary calcium intake had a 35% LOWER risk of incident kidney stones compared to the lowest quintile, after adjustment for other risk factors. The 1997 Curhan AJCN study in men replicated the finding. The mechanistic explanation came from balance studies showing that low-calcium diets produce higher urinary oxalate even when dietary oxalate is unchanged.
Practical implications for spinach consumers with kidney stone history:
- Maintain adequate total dietary calcium (1,000-1,200 mg/day) from low-oxalate sources (dairy if tolerated, fortified plant milk, sardines with bones, fortified orange juice).
- Pair high-oxalate foods (spinach, almonds) with calcium at the same meal — spinach with feta cheese, spinach lasagna with ricotta, almonds with yogurt.
- Avoid calcium SUPPLEMENTS taken AWAY from meals — this raises serum and urinary calcium without the protective gut-binding of dietary oxalate. Some evidence suggests supplemental calcium (vs dietary) may actually increase stone risk.
- Adequate hydration (2.5-3 liters fluid daily) is the single most important behavioral intervention for stone prevention, separate from dietary modifications.
If You Have Iron Deficiency
For patients with diagnosed iron-deficiency anemia or low ferritin, the appropriate approach is NOT to rely on spinach. Effective interventions in order of typical clinical use:
- Identify and address the cause — chronic blood loss (GI bleeding, heavy menstrual periods, frequent blood donation), malabsorption (celiac disease, atrophic gastritis, post-bariatric surgery), inadequate intake (strict vegan diets without iron supplementation), or chronic inflammation. The cause matters more than the supplement.
- Oral iron supplementation — ferrous sulfate 325 mg (containing 65 mg elemental iron) every other day on an empty stomach with vitamin C, per the 2015 Stoffel hepcidin-cycle research showing alternate-day dosing produces equivalent iron loading with fewer GI side effects compared to daily dosing. Continue for 3-6 months past ferritin normalization to replete iron stores.
- Heme iron foods — red meat (especially beef chuck, beef liver), poultry dark meat, shellfish (oysters, clams, mussels) provide 15-35% bioavailable iron. Beef liver delivers approximately 6.5 mg highly bioavailable iron per 100 g.
- Non-heme iron foods WITH vitamin C — lentils, tofu, pumpkin seeds, fortified breakfast cereal, blackstrap molasses, paired with citrus, bell peppers, tomatoes, or strawberries to enhance absorption.
- IV iron infusion — for severe deficiency, intolerance to oral iron, or malabsorption (ferric carboxymaltose, iron sucrose, low-molecular-weight iron dextran). Effective in single or 2-3 dose protocols.
Spinach can be a contributing source of dietary iron in a mixed approach but should not be the primary strategy. The 2% absorption rate means that achieving the 8-18 mg/day iron RDA from spinach alone would require eating multiple pounds per day, which is impractical and would deliver excessive oxalate.
For more on iron-deficiency management, see our Iron Deficiency Anemia page.
If You Are Oxalate-Sensitive
For patients with a history of calcium oxalate kidney stones (most stone formers), enteric hyperoxaluria (inflammatory bowel disease, fat malabsorption, Roux-en-Y gastric bypass), or known oxalate hyperabsorption:
- Reduce highest-oxalate foods — the "must reduce" list is spinach, rhubarb, beet greens, Swiss chard, almonds, peanuts, dark chocolate (especially raw cacao), and to a lesser extent tea (especially black tea), sweet potatoes, and instant coffee.
- Boil and discard water if eating moderate amounts of medium-oxalate foods; this is more effective than steaming for oxalate reduction.
- Maintain adequate calcium at meals (1,000-1,200 mg/day total) to bind oxalate in the gut.
- Hydrate aggressively — 2.5-3 liters fluid daily to keep urinary oxalate concentration low.
- Limit vitamin C megadoses — vitamin C is metabolized to oxalate; doses above 1,000 mg/day can meaningfully increase urinary oxalate. Maintain vitamin C intake at the 75-200 mg/day range for stone formers; avoid the multi-gram megadoses popular in some wellness regimens.
- Consider potassium citrate per urology recommendation — alkalinizes the urine and reduces calcium oxalate supersaturation; prescription therapy for recurrent stone formers.
- Low-oxalate spinach substitutes — for the leafy green benefits without the oxalate burden: cooked kale (moderate oxalate, generally tolerated), romaine lettuce (low oxalate), arugula (low oxalate), bok choy (low oxalate), butter lettuce (very low oxalate). These can substitute for spinach in salads and side dishes.
For more on kidney stone management, see our Kidney Stones page.
Key Research Papers
- Hallberg L, Hulthen L (2000). Prediction of dietary iron absorption: an algorithm for calculating absorption and bioavailability of dietary iron. AJCN 71:1147-1160. — Search PubMed
- Cook JD, Reddy MB (2001). Effect of ascorbic acid intake on nonheme-iron absorption from a complete diet. AJCN 73:93-98. — Search PubMed
- Heaney RP, Weaver CM (1989). Oxalate: effect on calcium absorbability. AJCN 50:830-832. — Search PubMed
- Chai W, Liebman M (2005). Effect of different cooking methods on vegetable oxalate content. J Agric Food Chem 53:3027-3030. — PubMed PMID 15826055
- Curhan GC et al. (1996). Comparison of dietary calcium with supplemental calcium and other nutrients as factors affecting the risk for kidney stones in women. NEJM 328:833-838. — Search PubMed
- Taylor EN, Curhan GC (2008). Determinants of 24-hour urinary oxalate excretion. CJASN 3:1453-1460. — PubMed PMID 18650406
- Hurrell RF et al. (1999). Inhibition of non-haem iron absorption in man by polyphenolic-containing beverages. British J Nutrition 81:289-295. — PubMed PMID 10999016
- Stoffel NU et al. (2017). Iron absorption from oral iron supplements given on consecutive versus alternate days. Lancet Haematology 4:e524-533. — PubMed PMID 29032957
- Curhan GC et al. (1997). Comparison of dietary calcium with supplemental calcium and other nutrients as factors affecting the risk for kidney stones in men. Ann Internal Med 126:497-504. — PubMed PMID 9092314
- Massey LK et al. (2001). Tea oxalate and calcium oxalate kidney stone risk. J Am Diet Assoc. PubMed: Tea oxalate stone risk
- Holmes RP, Goodman HO, Assimos DG (2001). Contribution of dietary oxalate to urinary oxalate excretion. Kidney International 59:270-276. — PubMed PMID 11135080
- Borghi L et al. (2002). Comparison of two diets for the prevention of recurrent stones in idiopathic hypercalciuria. NEJM 346:77-84. — PubMed PMID 11784873
PubMed Topic Searches
- PubMed: Spinach iron bioavailability
- PubMed: Calcium oxalate kidney stones
- PubMed: Vitamin C iron absorption
- PubMed: Oxalate cooking reduction
- PubMed: Alternate-day iron dosing
Connections
- Spinach Main Page
- Spinach Benefits Hub
- Spinach Folate & Pregnancy
- Spinach for Eyes
- Cooking vs Raw
- Iron
- Calcium
- Vitamin C (Iron Enhancer)
- Iron Deficiency Anemia
- Kidney Stones
- Crohn's Disease (Enteric Hyperoxaluria)
- Lentils (Better Plant Iron Source)
- Kale (Lower Oxalate)
- Beef Liver (Heme Iron)
- Eggs
- All Foods