LDH Test: Lactate Dehydrogenase — Tissue Damage and Disease Activity Marker
Lactate dehydrogenase (LDH) is an enzyme found in nearly every cell of the human body, where it catalyzes the final step of anaerobic glycolysis — the reversible conversion of pyruvate to lactate. When cells are damaged, dying, or under metabolic stress, LDH leaks out of the cell and into the bloodstream, making serum LDH a sensitive but non-specific marker of tissue injury. Clinicians use it to monitor hemolysis, track lymphoma and other cancers, evaluate pulmonary embolism severity, assess myocardial damage (a legacy role now replaced by troponin), and gauge the severity of critical illness. Understanding which LDH isoenzyme is elevated — and combining that knowledge with the clinical picture — is what transforms this humble marker into a powerful diagnostic clue.
Table of Contents
- Overview — What LDH Measures
- LDH Isoenzymes
- Reference Ranges
- Causes of Elevated LDH
- LDH in Hemolysis
- LDH in Cancer and Lymphoma
- LDH in Pulmonary Embolism
- LDH in Critical Illness
- Research References
- Featured Videos
Overview — What LDH Measures
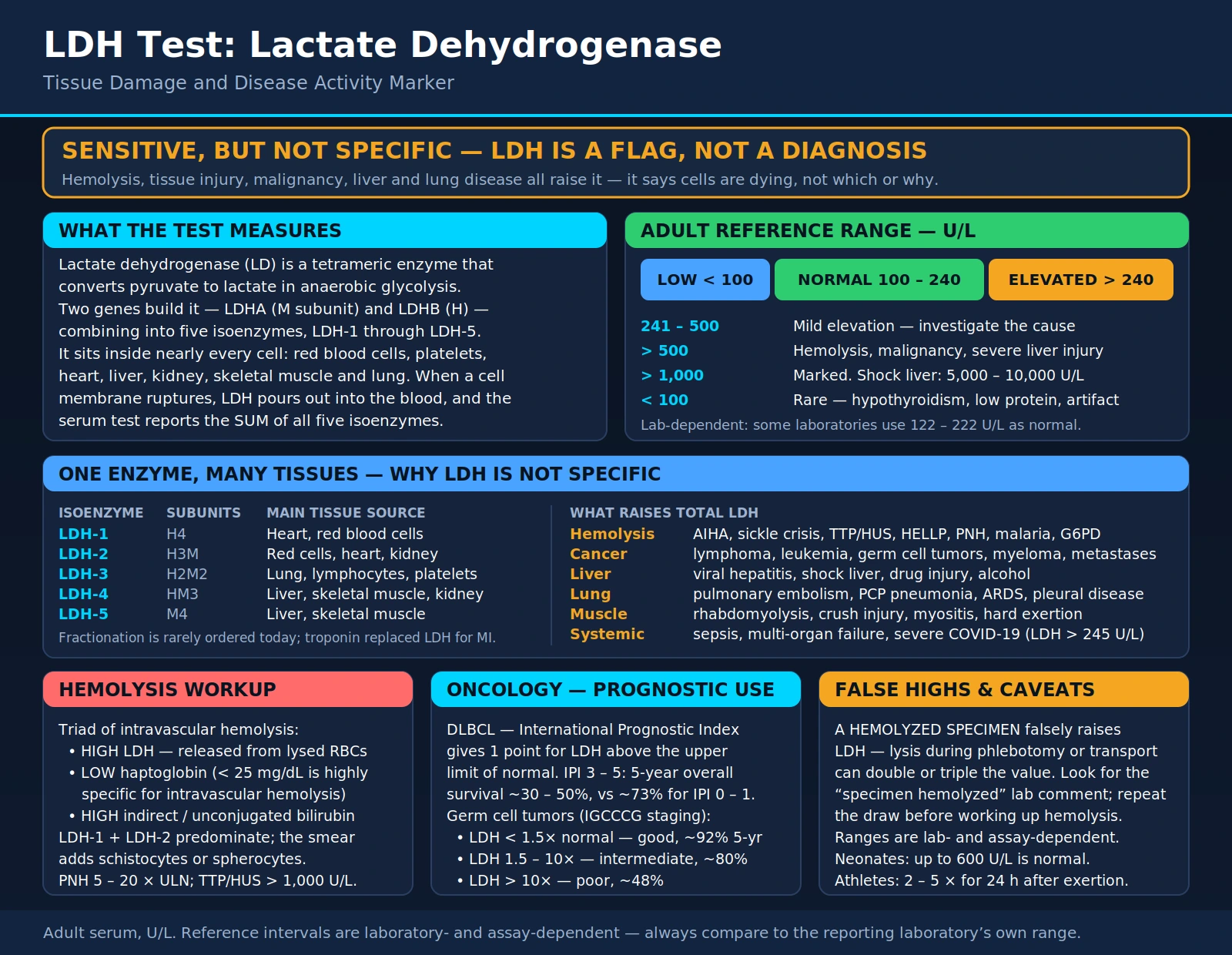
LDH (also written LD) is a tetrameric enzyme encoded by two gene products — LDHA and LDHB — which combine in different ratios to form five distinct isoenzymes (LDH-1 through LDH-5). The enzyme's job is reversible: it converts pyruvate to lactate during anaerobic metabolism, and lactate back to pyruvate when oxygen is available. This reaction is fundamental to cellular energy production under oxygen-limited conditions, such as intense exercise or hypoxia.
When cell membranes rupture due to injury, ischemia, inflammation, or programmed cell death, LDH pours out into the extracellular space and eventually into the bloodstream. The total serum LDH test measures the sum of all five isoenzymes. Because LDH is present in red blood cells, platelets, heart, liver, kidney, skeletal muscle, and lung, almost any type of significant cellular injury will raise the total. This sensitivity makes LDH useful for detecting that something is wrong; it takes isoenzyme fractionation or clinical context to identify what.
The major clinical applications today include: monitoring hemolytic anemia, tracking treatment response in lymphoma and germ cell tumors, risk-stratifying pulmonary embolism, and as a general severity marker in sepsis, organ failure, and COVID-19.
LDH Isoenzymes (LDH-1 through LDH-5)
The five LDH isoenzymes are formed by different combinations of two subunits — the H (heart) subunit encoded by LDHB and the M (muscle) subunit encoded by LDHA. Their tissue distributions differ substantially, which historically allowed clinicians to localize the source of cell injury from the isoenzyme fractionation pattern.
- LDH-1 (H4) — Heart and red blood cells: Composed of four H subunits. Predominates in cardiac muscle and erythrocytes. Historically, a rise in LDH-1 peaking 48–72 hours after chest pain onset was the classic laboratory confirmation of myocardial infarction before troponin assays were available. LDH-1 is also the primary isoenzyme released during red blood cell hemolysis.
- LDH-2 (H3M) — Red blood cells, heart, kidney: Three H subunits and one M subunit. Under normal conditions, LDH-2 is the most abundant isoenzyme in serum. Along with LDH-1, it predominates in intravascular hemolysis.
- LDH-3 (H2M2) — Lung, lymphocytes, platelets, brain: Two H and two M subunits. Elevated LDH-3 points toward pulmonary parenchymal injury (including Pneumocystis pneumonia), lymphoproliferative disease, or platelet destruction.
- LDH-4 (HM3) — Liver, skeletal muscle, kidney: One H subunit and three M subunits. Elevated in early hepatocellular injury and moderate muscle damage.
- LDH-5 (M4) — Liver and skeletal muscle: Four M subunits. The dominant liver isoenzyme. Markedly elevated in acute hepatocellular injury, rhabdomyolysis, and ischemic hepatitis. When LDH-5 is disproportionately elevated, liver or muscle damage is the likely source.
Historically, an LDH “flip” — in which LDH-1 rises above LDH-2 (reversing the normal LDH-2 > LDH-1 ratio) — was the classic laboratory pattern of acute myocardial infarction. Today, troponin I and T have completely replaced LDH for cardiac diagnosis due to superior sensitivity and specificity. Isoenzyme fractionation is rarely ordered in modern clinical practice; most laboratories report total LDH only, and fractionation must be specifically requested when needed to distinguish hepatic from cardiac or hemolytic sources.
Flipped LDH pattern in hemolysis: LDH-1 and LDH-2 predominate when red cells lyse, because erythrocytes are rich in these two cardiac-type isoenzymes. In contrast, LDH-5 dominates when the source of elevation is liver or skeletal muscle injury. This distinction — even without formal fractionation — can often be inferred from the clinical context and companion biomarkers (bilirubin, haptoglobin, CK, ALT, AST).
Reference Ranges
LDH — Adults (U/L)
LDH — Mild Elevation (U/L)
Reference ranges vary significantly between laboratories and assay methods — some institutions use 122–222 U/L as their normal interval. Always compare a result to the reporting laboratory's own reference range, printed on the result report. The values above reflect a commonly used adult reference interval in the United States.
Key thresholds to know:
- < 100 U/L (below normal): Rare; occasionally seen in hypothyroidism, low-protein states, or as a laboratory artifact. Clinical significance is uncertain in isolation.
- 100–240 U/L: Normal adult range. No specific action required; interpret in clinical context.
- 241–500 U/L (mild elevation): Warrants investigation. Can reflect mild hemolysis, hepatic inflammation, active lymphoma, muscle injury, or pulmonary disease.
- > 500 U/L (significant elevation): Strongly suggests active hemolysis, malignancy with high cell turnover, severe hepatocellular injury, rhabdomyolysis, or major organ ischemia.
- > 1,000 U/L (markedly elevated): Ischemic hepatitis (“shock liver”) can produce values of 5,000–10,000 U/L; Burkitt lymphoma, ALL, and severe rhabdomyolysis also reach this range.
Special populations:
- Neonates and infants: LDH is physiologically higher in the first weeks of life, with values up to 600 U/L considered normal in the neonatal period. Values normalize toward adult ranges by early childhood.
- Athletes: Intense endurance or resistance exercise transiently elevates LDH-5 (skeletal muscle source) by 2–5× within 24 hours of exertion. Values typically normalize within 48–72 hours of rest.
- Pregnancy: Mild LDH elevations are common in the third trimester, reflecting placental tissue turnover. Markedly elevated LDH in pregnancy may signal HELLP syndrome (Hemolysis, Elevated Liver enzymes, Low Platelets) and requires urgent evaluation.
Causes of Elevated LDH
Because LDH is expressed in nearly every tissue, the list of conditions that elevate it is broad. The key to clinical interpretation is grouping elevated LDH with companion findings that narrow the source.
Hemolytic conditions:
- Autoimmune hemolytic anemia (warm and cold antibody types)
- Sickle cell disease crisis
- Mechanical hemolysis (prosthetic heart valves, LVAD)
- Microangiopathic hemolytic anemia: thrombotic thrombocytopenic purpura (TTP), hemolytic uremic syndrome (HUS), HELLP syndrome
- Paroxysmal nocturnal hemoglobinuria (PNH)
- Transfusion reactions
- Malaria (parasitized erythrocytes lyse at merozoite release)
- G6PD deficiency during oxidative stress
LDH from lysed red blood cells is predominantly LDH-1 and LDH-2.
Cancer and hematologic malignancy:
- Non-Hodgkin lymphoma — LDH is incorporated into the International Prognostic Index (IPI) for diffuse large B-cell lymphoma (DLBCL)
- Hodgkin lymphoma
- Acute leukemia (ALL, AML)
- Germ cell tumors (testicular cancer) — LDH is one of three serum tumor markers used to stage non-seminomatous germ cell tumors (NSGCT)
- Multiple myeloma
- Metastatic solid tumors (liver metastases, lung metastases, melanoma)
Elevated LDH in malignancy reflects high tumor cell turnover and necrosis within rapidly growing tumor masses.
Myocardial injury (historical role):
- LDH rises 12–24 hours after myocardial infarction, peaks at 48–72 hours, and persists for 10–14 days — far longer than troponin
- Now replaced by troponin I and T for MI diagnosis; LDH retains a niche role in delayed presentations (>48–72h since symptom onset) when troponin may be normalizing
Liver disease:
- Acute viral hepatitis (A, B, E)
- Ischemic hepatitis (“shock liver”) — LDH often exceeds 5,000 U/L; the LDH/ALT ratio > 1.5 supports ischemic rather than viral etiology
- Drug-induced liver injury (DILI): acetaminophen, isoniazid, statins
- Hepatic infiltration by lymphoma
- Alcoholic hepatitis
Pulmonary conditions:
- Pulmonary embolism (reflects lung parenchymal infarction)
- Pneumocystis jirovecii pneumonia (PCP) — markedly elevated LDH, often >500 U/L, is a diagnostic clue in immunocompromised patients and correlates with disease severity
- ARDS (acute respiratory distress syndrome)
- Pleuritis and pleural effusion with inflammation
Skeletal muscle injury:
- Rhabdomyolysis — massive release; LDH may exceed 1,000 U/L; creatine kinase (CK) is the companion marker and rises proportionally higher
- Trauma, crush injury, compartment syndrome
- Extreme exertion (ultramarathon, military training)
- Inflammatory myopathies: dermatomyositis, polymyositis
- Statin-induced myopathy
Renal conditions:
- Renal infarction
- Acute tubular necrosis (ATN)
- HELLP syndrome
Critical illness and systemic conditions:
- Sepsis and multi-organ dysfunction — LDH elevation correlates with organ failure burden and mortality
- COVID-19 — LDH >245 U/L on admission associated with higher ICU admission rates and mortality in multiple cohort studies
- Hypothyroidism (mild LDH reduction; rarely causes elevation)
Artifactual elevation (clinically important): Specimen hemolysis during phlebotomy or transport releases red blood cell LDH and can double or triple the measured value. Always suspect artifact when LDH is unexpectedly elevated with no other supporting clinical findings. A lab comment noting “specimen hemolyzed” is the key flag. In this situation, a repeat venipuncture with careful sample handling is the correct next step — not further diagnostic workup for hemolytic disease.
LDH in Hemolysis
Detecting and quantifying hemolysis is one of the most clinically important uses of LDH. When red blood cells break down inside blood vessels (intravascular hemolysis), LDH is released in large quantities — primarily LDH-1 and LDH-2, reflecting the cardiac-type isoenzyme predominance within erythrocytes. The triad of elevated LDH + elevated indirect (unconjugated) bilirubin + low or undetectable haptoglobin is the classic laboratory fingerprint of intravascular hemolysis.
Each component of this triad reflects a different consequence of red cell lysis:
- LDH elevation reflects direct enzyme release from the ruptured cell membrane into the circulation.
- Haptoglobin falls because it binds free hemoglobin released during hemolysis; the hemoglobin-haptoglobin complex is rapidly cleared by hepatic macrophages, consuming available haptoglobin. A haptoglobin < 25 mg/dL is highly specific for intravascular hemolysis.
- Indirect bilirubin rises because metabolized heme is converted to unconjugated bilirubin faster than the liver can conjugate and excrete it.
The peripheral blood smear adds morphological evidence: schistocytes (fragmented red cells) in microangiopathic hemolytic anemia (TTP, HUS, HELLP), spherocytes in autoimmune hemolytic anemia, and sickled cells in sickle cell disease.
Clinical relevance by condition:
- Sickle cell disease: LDH distinguishes vaso-occlusive crisis (moderate LDH elevation reflecting ongoing sickling and minor hemolysis) from aplastic crisis (very low LDH when marrow suppression prevents cell production) or acute hemolytic crisis (markedly high LDH). Serial LDH tracks hemolytic rate over time and correlates with pulmonary hypertension risk in this population.
- TTP/HUS: Extremely high LDH (often >1,000 U/L) combined with thrombocytopenia and schistocytes on the blood smear is the diagnostic triad. LDH is used to monitor treatment response to plasma exchange — falling LDH confirms improving hemolysis.
- PNH: LDH is used to monitor disease activity and treatment response to eculizumab. Pre-treatment LDH can be 5–20× the upper limit of normal; eculizumab therapy normalizes it in most responders.
- Autoimmune hemolytic anemia (AIHA): LDH correlates with hemolytic severity and guides steroid and second-line therapy decisions.
LDH:AST ratio in distinguishing hemolysis from liver disease: In intravascular hemolysis, LDH rises disproportionately relative to AST, because RBCs contain abundant LDH but relatively little AST. A markedly elevated LDH with a normal or only mildly elevated AST in the correct clinical context strongly favors hemolysis over hepatocellular injury as the source.
LDH in Cancer and Lymphoma
LDH has dual value in oncology: as a staging and prognostic marker incorporated into established scoring systems, and as a serial treatment-response marker tracked over the course of therapy.
Diffuse Large B-Cell Lymphoma (DLBCL): The International Prognostic Index (IPI) assigns 1 point for an LDH above the upper limit of normal. A total IPI score of 3–5 (high-intermediate or high risk) is associated with a 5-year overall survival of roughly 30–50%, compared to approximately 73% for low-risk IPI (score 0–1). LDH above twice the upper limit of normal independently predicts inferior outcomes in most aggressive B-cell lymphoma subtypes. At diagnosis, LDH provides an immediate, inexpensive prognostic data point while awaiting PET staging results.
Germ Cell Tumors (NSGCT — Testicular Cancer): The International Germ Cell Cancer Collaborative Group (IGCCCG) classification uses LDH as one of three serum markers alongside AFP (alpha-fetoprotein) and beta-hCG to assign prognostic groups:
- LDH < 1.5× normal = Good prognosis (5-year survival ~92%)
- LDH 1.5–10× normal = Intermediate prognosis (~80%)
- LDH > 10× normal = Poor prognosis (~48%)
LDH normalization after orchiectomy or chemotherapy is tracked as a marker of remission. Rising LDH during surveillance raises concern for relapse and triggers re-imaging.
Leukemia and Myeloma: Markedly elevated LDH at diagnosis in acute leukemia correlates with high blast count and total disease burden. Serial LDH tracks treatment response — a falling LDH after induction chemotherapy suggests effective cytoreduction. In multiple myeloma, LDH elevation identifies a high-risk subset with extramedullary disease or plasma cell leukemia.
Metastatic Solid Tumors:
- Melanoma: The AJCC staging system designates Stage IV M1d for any distant metastatic site with elevated LDH, the category associated with worst prognosis among Stage IV patients. Baseline LDH predicts response to immunotherapy (ipilimumab, pembrolizumab) — patients with elevated LDH respond less well.
- Renal cell carcinoma: Elevated LDH is one component of the IMDC (International Metastatic RCC Database Consortium) adverse risk criteria.
- Small cell lung cancer: LDH correlates with disease burden and survival in both limited and extensive stage SCLC.
- Colorectal cancer with hepatic metastases: LDH elevation reflects hepatic involvement and correlates with volume of liver metastases.
Tumor Lysis Syndrome (TLS): After initiating chemotherapy for high-burden malignancies — especially Burkitt lymphoma, ALL, CLL, and bulky DLBCL — massive tumor cell death releases large quantities of LDH, potassium, phosphate, and uric acid into the circulation simultaneously. Monitoring LDH during the first 48–72 hours post-chemotherapy is standard practice to detect TLS before the electrolyte derangements cause cardiac arrhythmia, seizures, or acute kidney injury. Prophylactic allopurinol or rasburicase is given preemptively in high-risk patients.
LDH in Pulmonary Embolism
In pulmonary embolism, LDH elevation reflects lung parenchymal infarction and ischemic pneumocyte death distal to the occluded pulmonary artery. LDH is not part of the initial diagnostic algorithm for PE — that role belongs to D-dimer, the Wells score, and CT pulmonary angiography. However, once PE is confirmed, LDH elevation — particularly in the context of elevated troponin and elevated BNP/NT-proBNP — contributes to hemodynamic risk stratification. The combination of right ventricular dysfunction (by echo or CT) plus elevated cardiac biomarkers identifies the intermediate-high risk group most likely to benefit from systemic or catheter-directed thrombolysis.
Pleural effusion differentiation: LDH is also measured in pleural fluid to classify effusions as transudates versus exudates using Light's Criteria. An exudate is suggested when any of the following are present:
- Pleural fluid protein / serum protein > 0.5
- Pleural fluid LDH / serum LDH > 0.6
- Pleural fluid LDH > two-thirds the upper limit of normal for serum LDH
Exudative effusions (parapneumonic, malignant, rheumatoid, empyema) require further workup; transudative effusions (heart failure, cirrhosis, nephrotic syndrome) reflect fluid redistribution and are managed by treating the underlying condition.
Pneumocystis jirovecii pneumonia (PCP): In immunocompromised patients — especially HIV-positive individuals with CD4 count <200 cells/µL, solid organ transplant recipients, and patients on prolonged high-dose corticosteroids — markedly elevated LDH (often >500 U/L, sometimes >1,000) in the setting of subacute hypoxia and bilateral infiltrates is a diagnostic clue to PCP pneumonia. A normal LDH in a hypoxic HIV patient makes PCP substantially less likely. LDH also correlates with disease severity and predicts the likelihood of requiring mechanical ventilation; LDH >500 U/L at presentation is associated with significantly increased 30-day mortality.
Practical pearl: When a patient has unexplained hypoxia with bilateral infiltrates and an elevated LDH, the differential includes PE, PCP (if immunocompromised), atypical bacterial pneumonia, and ARDS. CT pulmonary angiography plus bronchoalveolar lavage with Gomori methenamine silver stain or direct fluorescent antibody testing for Pneumocystis resolves the diagnosis in most cases.
LDH in Critical Illness and COVID-19
In the intensive care unit, LDH elevation is common and typically multifactorial — simultaneously reflecting elements of hepatic ischemia from hypoperfusion, intravascular hemolysis, skeletal muscle catabolism, lung parenchymal injury, and systemic cytokine-driven inflammation. A single LDH value is less informative than a serial trend: rising LDH over 24–48 hours signals worsening organ failure, while a sustained decline accompanying clinical improvement confirms tissue reperfusion and reduced cell death rate.
COVID-19: During the SARS-CoV-2 pandemic, LDH emerged as one of the most consistently and markedly elevated biomarkers in severe disease. A pooled meta-analysis (Henry et al., 2020, PMID 32738466) found LDH was elevated in approximately 73% of ICU-admitted COVID-19 patients versus 25% of ward patients. An LDH >245 U/L on hospital admission was independently associated with a roughly 6-fold higher odds of severe disease progression. LDH was incorporated alongside ferritin, CRP, interleukin-6, and D-dimer as a cluster of “cytokine storm” severity markers used to identify patients at risk of rapid deterioration who might benefit from anti-inflammatory therapy (dexamethasone, tocilizumab).
The mechanism of LDH elevation in COVID-19 is multifactorial: SARS-CoV-2 infects ACE2-expressing type II pneumocytes directly, causing diffuse alveolar damage and releasing LDH from dying lung cells. Simultaneously, systemic cytokine-mediated inflammation (the “cytokine storm”) produces multi-organ endothelial injury and microthrombi, releasing LDH from liver, kidney, and red blood cells. Macrophage activation and lymphocyte death contribute additional LDH from hematopoietic sources.
Sepsis: In bacterial sepsis and septic shock, LDH elevation reflects global tissue hypoperfusion and anaerobic metabolism. An elevated serum LDH alongside elevated serum lactate (lactic acidosis) indicates that oxygen delivery to tissues is insufficient to meet metabolic demands — a defining feature of distributive shock. Normalization of LDH over 12–24 hours with adequate fluid resuscitation, vasopressor therapy, and source control confirms tissue reperfusion. In sepsis-associated multi-organ failure, LDH correlates with the number of failing organ systems and predicts 28-day mortality in several scoring systems.
Ischemic hepatitis (“shock liver”): Acute hepatic ischemia from cardiac arrest, cardiogenic shock, or severe hypotension produces one of the highest LDH elevations seen in any condition — often 5,000–10,000 U/L or higher — accompanied by proportionally elevated AST, ALT, and coagulopathy. The LDH/ALT ratio is characteristically >1.5 in ischemic hepatitis, helping distinguish it from acute viral hepatitis where ALT often rises more prominently. Recovery is rapid if perfusion is restored, with LDH often halving within 48–72 hours.
Research References
The following are peer-reviewed publications and PubMed searches supporting the clinical evidence base for LDH testing and interpretation.
- Wroblewski F, LaDue JS. Lactic dehydrogenase activity in blood. Proc Soc Exp Biol Med. 1955;90(1):210–213. PMID: 13272257 — PubMed
- Zaman Z, Verwilghen RL. Quantitation of lactate dehydrogenase isoenzymes in serum. Clin Chim Acta. 1979;96(3):249–258. PMID: 466474 — Search PubMed
- Shipp MA, et al. A predictive model for aggressive non-Hodgkin's lymphoma. N Engl J Med. 1993;329(14):987–994. PMID: 8141877 — PubMed
- International Germ Cell Cancer Collaborative Group. International germ cell consensus classification: a prognostic factor-based staging system for metastatic germ cell cancers. J Clin Oncol. 1997;15(2):594–603. PMID: 9053482 — PubMed
- Montagnana M, Lippi G. Lactate dehydrogenase in clinical laboratory practice. J Lab Med. 2007;31:56–61. PubMed Search
- Henry BM, et al. Lactate dehydrogenase levels predict coronavirus disease 2019 (COVID-19) severity and mortality: A pooled analysis. Am J Emerg Med. 2020;38(9):1722–1726. PMID: 32738466 — PubMed
- Lippi G, Valentino M, Cervellin G. Laboratory diagnosis of acute myocardial infarction. Clin Biochem. 2014;47(1–2):17–24. PMID: 24140059 — Search PubMed
- Brodsky RA. Paroxysmal nocturnal hemoglobinuria. Blood. 2014;124(18):2804–2811. PMID: 25237200 — PubMed
- Shankar-Hari M, et al. Developing a New Definition and Assessing New Clinical Criteria for Septic Shock. JAMA. 2016;315(8):775–787. PMID: 26903336 — PubMed
- Levesque E, et al. Serum lactate dehydrogenase as a hepatocellular injury marker in patients with liver disease. Liver Int. 2014;34(4):e27–e35. PMID: 23870105 — Search PubMed
- Konstantinides SV, et al. 2019 ESC Guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J. 2020;41(4):543–603. PMID: 31504429 — PubMed
- Klatt EC, McGee RS. Pneumocystis carinii pneumonia and lactic dehydrogenase. Arch Intern Med. 1987;147(9):1609–1614. PMID: 3115712 — Search PubMed
PubMed topic search: PubMed: lactate dehydrogenase clinical significance
External Authoritative Resources
- MedlinePlus — Laboratory Tests Reference
- Lab Tests Online — Patient-Oriented Lab Test Reference (AACC)
- StatPearls / NCBI Bookshelf — Clinical Laboratory Reference
Connections
- All Lab Tests
- Comprehensive Metabolic Panel
- Liver Function Tests
- Inflammatory Markers
- Complete Blood Count
- D-Dimer Test
- Ferritin Test
- High-Sensitivity CRP
- Procalcitonin Test
- Uric Acid
- Anemia
- Lymphoma
- Pulmonary Embolism
- Rhabdomyolysis
- NAFLD
- Chronic Kidney Disease