Anti-Müllerian Hormone (AMH) Test
Anti-Müllerian hormone (AMH) is a glycoprotein produced by granulosa cells in growing ovarian follicles that serves as the most reliable direct measure of a woman's remaining egg supply — called ovarian reserve. Unlike FSH and estradiol, which fluctuate significantly across the menstrual cycle, AMH remains relatively stable throughout the cycle and even between cycles, making it measurable at any time with high clinical accuracy. AMH testing has transformed fertility evaluation, helping women understand their reproductive timeline, guiding assisted reproduction protocols, and detecting conditions like PCOS and premature ovarian insufficiency.
Table of Contents
- What AMH Measures
- Why It Is Ordered
- How the Test Is Performed
- Reference Ranges and Interpretation
- What Abnormal Results Mean
- Conditions It Helps Detect
- How to Protect and Improve Your Numbers
- Limitations and Considerations
- Key Research Papers
- Featured Videos
What AMH Measures
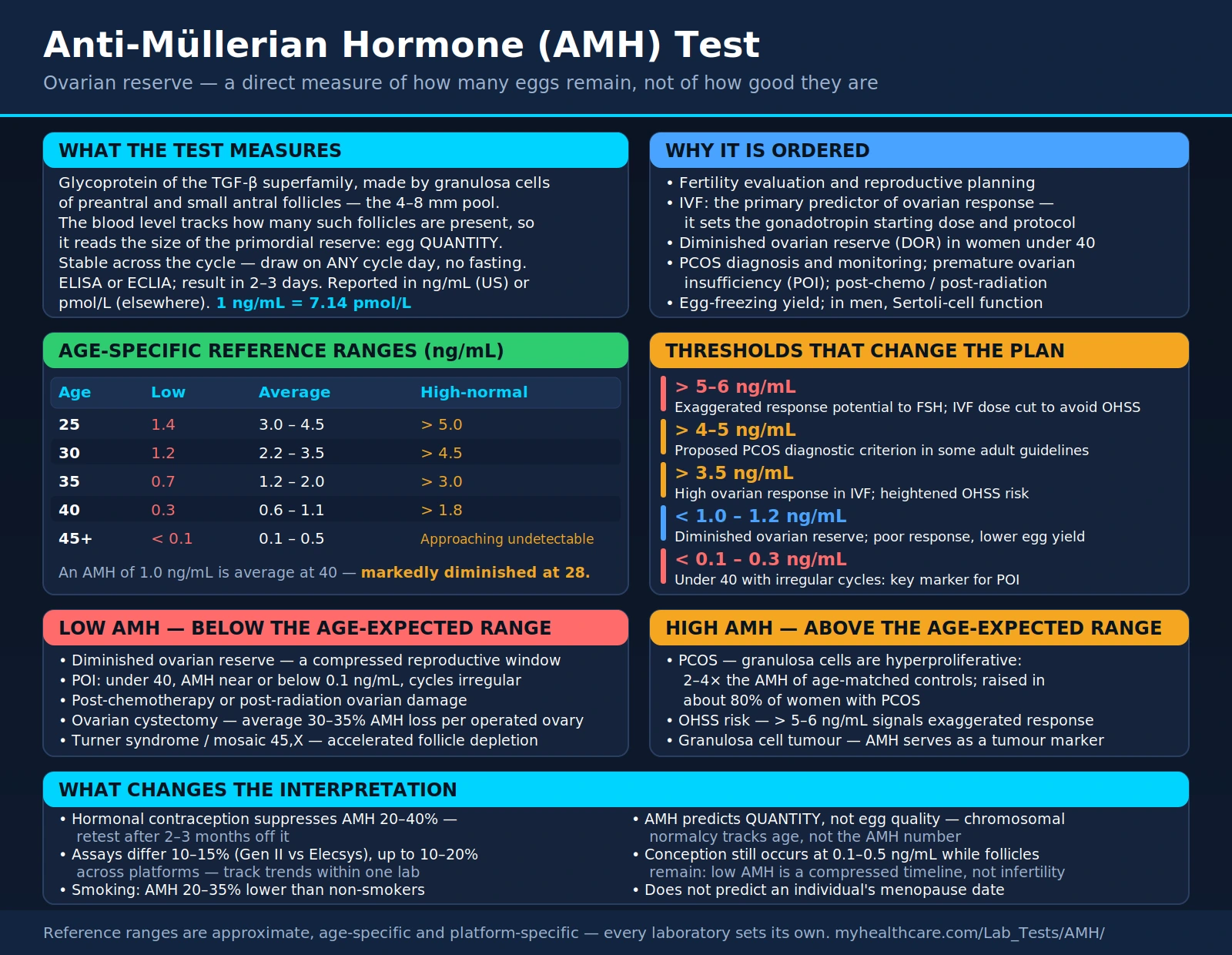
Anti-Müllerian hormone is a member of the transforming growth factor-beta (TGF-β) superfamily. In women, it is secreted by granulosa cells of preantral and small antral follicles — the pool of follicles that are currently actively growing and reflect the overall size of the primordial follicle reserve. This is the reserve established before birth that cannot be replenished; it declines continuously from birth onward, accelerating after age 32 and dropping sharply around age 37.
Because AMH is produced specifically by follicles in the 4–8 mm size range (primary and secondary follicles just becoming FSH-sensitive), its blood level directly reflects how many of these follicles are present — and by extension, how large the deeper primordial pool is. Women with more follicles at any given age have higher AMH; women with fewer have lower AMH.
In men, AMH is produced by Sertoli cells from fetal life through puberty and plays an essential role in male sexual differentiation (causing regression of the Müllerian ducts that would otherwise become the female reproductive tract). In adult men, AMH levels are much lower and are used clinically to assess testicular function, particularly Sertoli cell reserve in infertility workups.
Why It Is Ordered
For women, AMH is ordered in the following clinical contexts:
- Fertility evaluation and reproductive planning — particularly for women who want to understand how much time they may have before egg quantity becomes a significant fertility barrier
- IVF (in vitro fertilization) planning — AMH is the primary predictor of ovarian response to controlled ovarian stimulation, guiding the gonadotropin starting dose and protocol selection
- Evaluation of diminished ovarian reserve (DOR), particularly in women under 40 with unexpected difficulty conceiving
- Diagnosis and monitoring of polycystic ovary syndrome (PCOS), where AMH is typically 2–4 times higher than age-matched controls
- Assessment of premature ovarian insufficiency (POI, formerly called premature menopause) in women under 40 with irregular or absent periods
- Monitoring ovarian function after chemotherapy, radiation, or ovarian surgery to assess whether treatment has compromised fertility potential
- Evaluation before elective egg freezing to estimate expected yield and counsel on realistic expectations
- Evaluation of Turner syndrome or other chromosomal conditions affecting ovarian development
For men, AMH is ordered to assess Sertoli cell function in azoospermia (absent sperm), distinguish obstructive from non-obstructive causes of infertility, and evaluate intersex conditions or undescended testes.
How the Test Is Performed
The AMH test requires a standard venous blood draw. Because AMH levels do not meaningfully fluctuate with the menstrual cycle, the test can be done on any day of the cycle — a significant practical advantage over FSH and estradiol testing, which must be drawn on cycle days 2–4 for accurate interpretation.
Fasting is not required. The blood sample is processed using an enzyme-linked immunosorbent assay (ELISA) or electrochemiluminescence immunoassay (ECLIA). Results are typically available within 2–3 days and reported in ng/mL (United States) or pmol/L (Europe and elsewhere; 1 ng/mL = 7.14 pmol/L).
Two major assay platforms are widely used: the Beckman Coulter AMH Gen II assay and the Elecsys AMH Plus assay (Roche). Results between platforms can differ by 10–15%, so serial monitoring is best done using the same laboratory platform for consistency.
AMH declines gradually over years, not months — a single test result provides useful snapshot information. Annual monitoring is sufficient for most women tracking ovarian reserve changes unless there is a specific clinical reason (e.g., post-chemotherapy monitoring) to test more frequently.
Reference Ranges and Interpretation
AMH levels decline continuously with age. Interpreting any single value requires comparison against age-specific norms, not a single population-wide cutoff. The table below reflects the approximate age-related distribution:
| Age | Low (ng/mL) | Average (ng/mL) | High-Normal (ng/mL) |
|---|---|---|---|
| 25 | 1.4 | 3.0 – 4.5 | > 5.0 |
| 30 | 1.2 | 2.2 – 3.5 | > 4.5 |
| 35 | 0.7 | 1.2 – 2.0 | > 3.0 |
| 40 | 0.3 | 0.6 – 1.1 | > 1.8 |
| 45+ | < 0.1 | 0.1 – 0.5 | Approaching undetectable |
Interpreting against age is essential: An AMH of 1.0 ng/mL is reassuringly average for a 40-year-old but represents markedly diminished reserve in a 28-year-old. For IVF planning specifically, values below 1.0 ng/mL at any age are associated with poor ovarian response and lower expected egg yields, while values above 3.5 ng/mL are associated with high response and heightened risk of ovarian hyperstimulation syndrome (OHSS).
What Abnormal Results Mean
Low AMH (below age-expected range):
- Diminished ovarian reserve — fewer remaining eggs than expected for the patient's age, indicating a compressed reproductive window
- Premature ovarian insufficiency (POI) — in women under 40 with AMH near or below 0.1 ng/mL and irregular or absent cycles
- Post-chemotherapy or post-radiation ovarian damage — AMH drops rapidly after gonadotoxic treatment; recovery varies by regimen, age, and individual ovarian reserve
- Ovarian cystectomy — removal of ovarian tissue (e.g., for endometriomas) irreversibly reduces follicle count and AMH
- Turner syndrome or mosaic Turner — 45,X and mosaic karyotypes cause accelerated follicle depletion from birth
High AMH (above age-expected range):
- Polycystic ovary syndrome (PCOS) — granulosa cells in PCOS ovaries are hyperproliferative, producing 2–4 times the AMH of age-matched controls; AMH is increasingly used as a diagnostic criterion for PCOS in conjunction with clinical and ultrasound features
- Ovarian hyperstimulation risk — very high AMH (>5–6 ng/mL) signals exaggerated ovarian response potential to FSH stimulation; IVF protocols must be adjusted downward to prevent dangerous OHSS
- Granulosa cell tumor — rarely, a significantly elevated AMH in a post-menopausal woman or one without PCOS may indicate a granulosa cell tumor of the ovary; AMH is used as a tumor marker for monitoring treatment and recurrence
Conditions It Helps Detect
- Polycystic ovary syndrome (PCOS): AMH is elevated in approximately 80% of women with PCOS, reflecting the two to four times greater number of antral follicles in polycystic ovaries compared to normal ovaries. Some guidelines now include AMH >4–5 ng/mL as a diagnostic criterion in adult women, potentially replacing the need for pelvic ultrasound in some settings.
- Premature ovarian insufficiency (POI): AMH below 0.1–0.3 ng/mL in a woman under 40 with menstrual irregularity is a key diagnostic marker. It helps differentiate true ovarian failure from hypothalamic amenorrhea (where AMH may be low-normal rather than undetectable).
- Diminished ovarian reserve (DOR): Women with AMH below 1.0–1.2 ng/mL at any age may face greater difficulty conceiving naturally or with IVF, though spontaneous conception remains possible even at very low AMH levels as long as any eggs remain.
- Endometriosis: Women with endometriosis, particularly those who have undergone surgery for endometriomas, often have lower AMH than age-matched controls due to inflammatory damage to adjacent follicles and surgical follicle loss. AMH helps quantify this impact.
- Fertility preservation planning: AMH guides oncologists and reproductive endocrinologists in counseling young women facing gonadotoxic cancer treatment about egg freezing before treatment and monitoring after.
- Granulosa cell tumors: These rare ovarian tumors produce AMH as a tumor marker. Post-treatment AMH monitoring detects recurrence earlier than imaging alone.
How to Protect and Improve Your Numbers
AMH reflects a finite, non-renewable resource — primordial follicles cannot be regenerated. However, several modifiable factors influence the rate of follicle depletion and the functional quality of remaining eggs:
- Avoid smoking: Cigarette smoking directly accelerates follicle loss through polycyclic aromatic hydrocarbon-mediated apoptosis of granulosa cells. Women who smoke have AMH levels 20–35% lower than non-smokers at comparable ages. Quitting smoking slows the decline, though lost follicles cannot be recovered.
- Vitamin D optimization: Multiple studies find positive correlations between serum 25-OH vitamin D levels and AMH, particularly in women with PCOS. Vitamin D receptors are expressed in granulosa cells, and deficiency appears to impair follicle function. Optimizing vitamin D to 50–70 ng/mL may support better ovarian function.
- Maintain healthy weight: Both obesity and underweight disrupt hypothalamic-pituitary-ovarian signaling. Obesity accelerates follicle depletion through chronic low-grade inflammation and elevated insulin; underweight suppresses LH pulsatility needed for follicle recruitment. A healthy BMI supports more regular follicle development and protects remaining reserve.
- DHEA supplementation (under medical supervision): For women with diminished ovarian reserve preparing for IVF, dehydroepiandrosterone (DHEA) 25–75 mg/day has been studied as a pretreatment to improve egg quality and IVF outcomes. Some small trials show modest AMH increases with DHEA over 4–6 months; the evidence is mixed but the risk is low when short-term use is monitored.
- Reduce environmental exposome exposures: Endocrine-disrupting chemicals — BPA in plastics, phthalates in personal care products, dioxins in conventionally raised meat, pesticide residues — are associated with accelerated ovarian aging and lower AMH in observational studies. Reducing exposure through glass food storage, cleaner personal care products, and organic produce is a reasonable harm-reduction strategy.
- CoQ10 (ubiquinol form): Mitochondrial function in oocytes is critical for meiosis and early embryo development; CoQ10 declines with age and is essential for mitochondrial energy production. Supplemental CoQ10 (200–600 mg/day ubiquinol) has been studied in IVF patients with DOR and in some trials shows improvements in egg maturation rates and embryo quality, though it does not directly raise AMH.
- Avoid unnecessary ovarian surgery: Surgical removal of endometriomas — even by expert surgeons using minimal-damage techniques — inevitably removes some normal ovarian cortex containing primordial follicles. The decision to operate on endometriomas must weigh pain relief against the documented AMH reduction (average 30–35% decline per operated ovary). Repeated surgeries cause cumulative, additive damage.
Limitations and Considerations
- AMH predicts quantity, not quality: The most important determinant of egg quality — chromosomal normalcy — correlates with age but not with AMH level. A woman with a low AMH at age 32 may have excellent egg quality; a woman with a high AMH at age 42 still faces the high aneuploidy rates typical of her age group. AMH tells you how many eggs remain, not how genetically normal they are.
- Spontaneous conception remains possible at low AMH: Even very low AMH values (0.1–0.5 ng/mL) do not mean conception is impossible without IVF. As long as any follicles remain, spontaneous ovulation and conception can occur. Low AMH means diminished reserve — a compressed timeline — not infertility.
- Hormonal contraceptives suppress AMH: Combined oral contraceptive pills, hormonal IUDs, and the contraceptive ring suppress AMH by 20–40% during use. Testing AMH while on hormonal contraception underestimates true reserve. For the most accurate assessment, test after at least 2–3 months off hormonal contraception.
- Assay variability: Different AMH assay platforms can produce results varying by 10–20%. Serial monitoring should use the same laboratory platform for reliable trend tracking. Reference ranges are platform-specific.
- Not a fertility guarantee or deadline: AMH should not be interpreted as a biological clock that predicts exactly when fertility will end for any individual woman. There is wide variability in how long women with similar AMH levels can conceive naturally. AMH informs probabilistic counseling, not individual timelines.
- Not predictive of time to natural menopause: While population-level studies correlate AMH trajectories with menopause timing, AMH in an individual woman does not reliably predict her personal menopause date within a useful clinical window (the confidence intervals are wide).
Key Research Papers
The following curated PubMed citations and literature searches cover the major evidence base for the AMH test in clinical practice.
- Search PubMed
- Broer SL et al. (2010) — Anti-Mullerian hormone predicts ovarian response to FSH in IVF: a meta-analysis. Human Reproduction Update. PMID: 20616151
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- AMH and Vitamin D — PubMed literature search
- AMH as tumor marker — PubMed literature search
External Authoritative Resources
- MedlinePlus — Anti-Müllerian Hormone Test
- Lab Tests Online — Anti-Müllerian Hormone (AACC)
- ASRM — Ovarian Reserve Testing Patient Guide
Connections
- All Lab Tests
- Hormone Panel
- Testosterone Test
- DHEA-S Test
- Thyroid Panel
- Cortisol Test
- Fasting Insulin
- Polycystic Ovary Syndrome (PCOS)
- Vitamin D3
- Magnesium
- Zinc
- Inflammatory Markers
- Complete Blood Count