Sage for Antimicrobial Use & Sore Throat
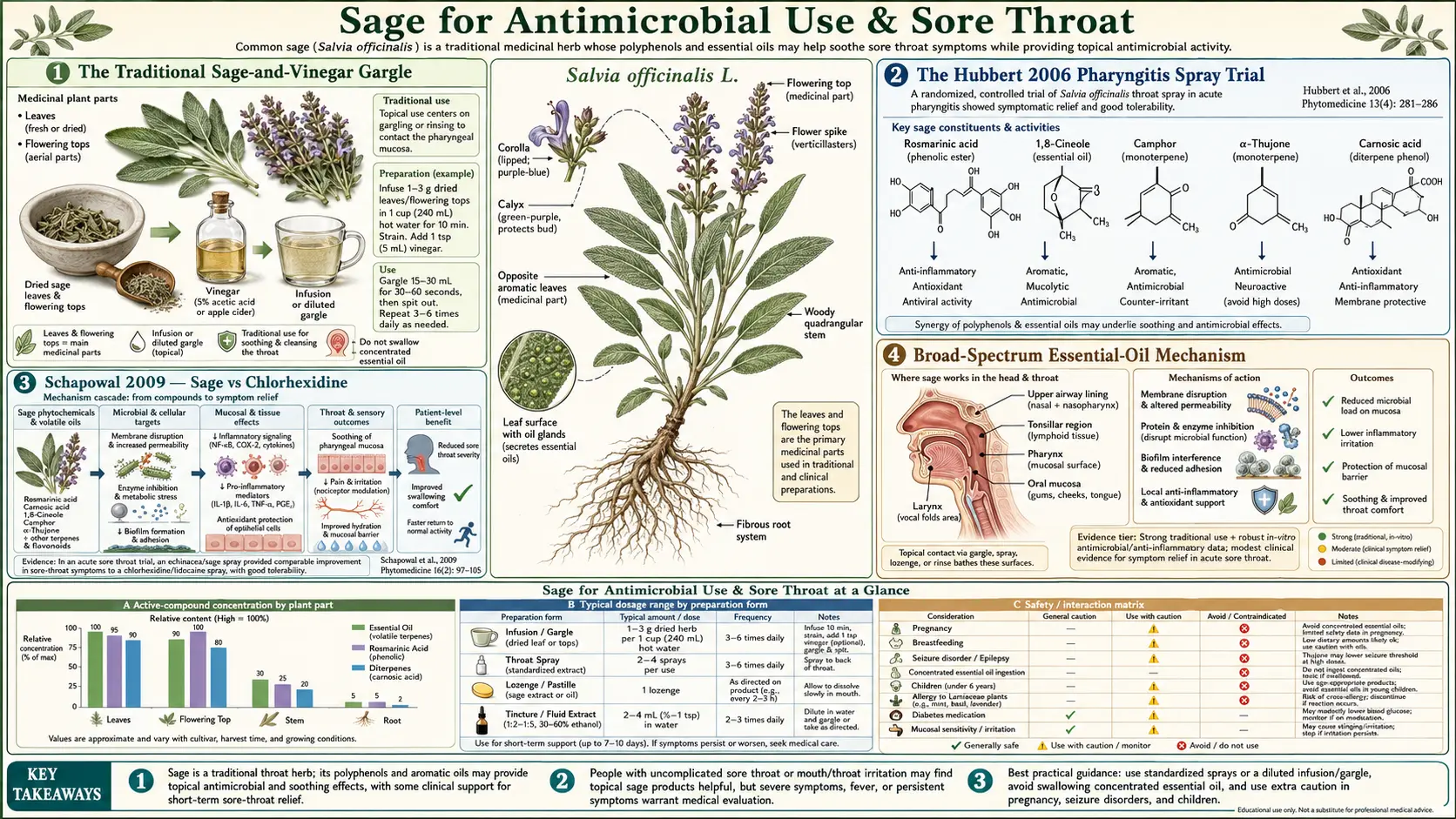
A sage-and-vinegar gargle for sore throat is one of the most universally taught home remedies in European folk medicine, recommended in 16th-century herbals and still in the front pages of every Mediterranean grandmother's health notebook. The traditional indication tracks well to modern microbiology: sage essential oil shows broad-spectrum activity against the bacterial and fungal species that colonize the oral cavity and oropharynx, including Streptococcus pyogenes (the cause of bacterial sore throat / "strep throat"), Staphylococcus aureus, Candida albicans, and several oral biofilm species. The clinical anchor is the Hubbert 2006 multicenter randomized double-blind placebo-controlled trial of a 15% sage essential-oil spray in 286 adult patients with acute viral pharyngitis: significantly faster symptom relief than placebo, with the effect appearing within the first two hours of the first dose. A subsequent Schapowal 2009 trial showed that an echinacea-sage spray was equivalent to a prescription chlorhexidine-lidocaine spray in symptom relief, suggesting sage's combined antimicrobial-plus-mild-anaesthetic action can substitute for a pharmaceutical sore-throat formulation. The traditional gargle, the modern lozenge, the mouthwash for gingivitis, and the historic plague-doctor reputation all rest on the same broad-spectrum essential-oil pharmacology.
Table of Contents
- The Traditional Sage-and-Vinegar Gargle
- The Hubbert 2006 Pharyngitis Spray Trial
- Schapowal 2009 — Sage vs Chlorhexidine
- Broad-Spectrum Essential-Oil Mechanism
- Sage vs Streptococcus pyogenes
- Sage vs Candida albicans and Oral Thrush
- Sage Mouthwash for Gingivitis & Oral Biofilm
- The Plague-Doctor Vinegar & Sage History
- Practical Preparations — Gargle, Lozenge, Spray, Mouthwash
- Cautions for Topical & Oropharyngeal Use
- Key Research Papers
- Connections
- Featured Videos
The Traditional Sage-and-Vinegar Gargle
The traditional Mediterranean preparation for a sore throat is a hot tea of one tablespoon of dried sage leaf in 250 mL of water steeped 10 minutes covered, strained, and combined with one tablespoon of apple-cider vinegar and a teaspoon of honey. The mixture is used to gargle for 30 seconds, swish through the front of the mouth for another 15 seconds, and either spat out or swallowed. The recommended frequency for active sore throat is every 2 to 3 hours during the acute phase.
Each component has a pharmacological role:
- Sage essential oil (extracted into the hot water during the 10-minute steep) — the primary antimicrobial agent, with broad-spectrum activity at the concentrations achieved in a strong tea
- Sage polyphenols (rosmarinic acid, carnosic acid, flavonoids) — anti-inflammatory and astringent effects on the inflamed mucosal surface
- Acetic acid from vinegar — lowers local pH, which is itself bactericidal at the levels reached in a gargle, and is the basis of the "vinegar tea-cleanse" tradition for oral biofilm
- Honey — provides demulcent coating of the inflamed pharyngeal mucosa, has its own antimicrobial activity through hydrogen peroxide generation and high osmolarity, and makes the gargle palatable
The German Commission E monograph for Folium Salviae explicitly lists "inflammation of the mucous membranes of the mouth and throat" as an established indication and describes the dilute tea-gargle as a recognized therapeutic preparation. The European Medicines Agency's well-established-use indication agrees.
The Hubbert 2006 Pharyngitis Spray Trial
The pivotal modern clinical trial of sage for sore throat is the Hubbert and colleagues multicenter randomized double-blind placebo-controlled study published in European Journal of Medical Research in 2006. The protocol:
- 286 adult patients with acute viral pharyngitis — defined as sore throat onset within 72 hours, with at least moderate throat pain and no clinical suspicion of bacterial (strep) etiology
- Randomized to a 15% Salvia officinalis essential-oil spray, a 5% sage spray, or placebo spray (vehicle only)
- Two sprays applied to the throat every 2 hours during waking hours
- Primary outcome: throat pain reduction at 2 hours after first dose (visual analog scale)
- Secondary outcomes: throat pain reduction at later time points, tolerability, global assessment
The headline results:
- 15% sage spray — significantly faster throat-pain reduction than placebo at 2 hours after first dose. The pain-reduction effect was clinically meaningful (about 60% symptomatic improvement from baseline) and rapid.
- 5% sage spray — trend toward benefit but did not reach statistical significance versus placebo, suggesting a dose-response relationship
- Placebo spray — the placebo response itself was substantial (typical for self-reported throat-pain trials), but the 15% sage spray clearly exceeded it
- Tolerability — well tolerated. The most common adverse effect was transient bitter taste; no serious adverse events.
The two-hour timeline is notable. A bacterial culture takes 24 to 48 hours, and even the rapid streptococcal antigen test takes 5 to 10 minutes. A sore-throat patient who feels meaningfully better within two hours of starting a treatment is getting symptom relief on a clinically relevant timescale. The combination of broad-spectrum essential-oil antimicrobial action and the mild local-anaesthetic and anti-inflammatory effect of the sage polyphenols is the likely explanation.
The 15% sage spray product evaluated in the Hubbert trial (Salviathymol N) became a regulated phytomedicine in several European countries on the strength of this evidence. In the U.S., similar concentrations are achievable with carefully prepared concentrated sage tea or with commercial throat-spray products that combine sage with thyme, echinacea, or other antimicrobial botanicals.
Schapowal 2009 — Sage vs Chlorhexidine
The Schapowal, Berger and colleagues 2009 trial published in European Journal of Medical Research compared an echinacea-sage combination spray against a chlorhexidine-lidocaine combination spray (the standard prescription European sore-throat formulation) in 154 adult patients with acute sore throat. The two products were compared head-to-head, double-blind, double-dummy.
The result was therapeutic equivalence. The echinacea-sage spray produced symptom reduction comparable to the chlorhexidine-lidocaine spray, with similar onset and duration of effect. The botanical product had a slightly more favorable tolerability profile (chlorhexidine produces transient tongue and dental staining with repeated use; lidocaine produces brief numbing of the tongue that some patients dislike).
The therapeutic-equivalence finding is important because it positions sage-containing products not as an "alternative" inferior option but as a clinically equivalent first-line choice for acute viral pharyngitis. The fact that the comparator was a prescription product (rather than acetaminophen or saltwater gargle) raises the practical clinical bar substantially.
Broad-Spectrum Essential-Oil Mechanism
The antimicrobial mechanism of sage essential oil is largely shared with the essential oils of related labiate herbs (thyme, oregano, rosemary, marjoram). The dominant pharmacology is membrane-disruption by lipophilic monoterpenes:
- The essential-oil constituents are small lipophilic molecules that partition into the bacterial cell membrane (or fungal cell membrane / yeast cell wall)
- At threshold concentrations, the accumulated membrane perturbation disrupts membrane integrity, leaks intracellular contents (ATP, potassium, nucleotides), and kills the cell
- This is a relatively non-specific mechanism, which is why a broad range of unrelated microbes is susceptible — gram-positive bacteria (Strep pyogenes, Staph aureus), gram-negative bacteria (E. coli), fungi (Candida albicans), and biofilm communities
- The same non-specific membrane mechanism means resistance does not develop the way it does with targeted antibiotics — there is no enzyme to mutate, no efflux pump to upregulate, no target receptor to modify
Among the sage essential-oil constituents, 1,8-cineole, thujone, camphor, and alpha-pinene all contribute to the antimicrobial effect, with the relative contribution varying by target organism. The minimum inhibitory concentrations (MICs) for sage essential oil against most relevant respiratory pathogens are in the 0.05 to 0.5% range — well below the 5% or 15% concentrations used in the Hubbert trial spray, providing a comfortable safety margin between the topical application concentration and the in-vitro inhibitory threshold.
The clinical reach of this mechanism is limited. Topical and oropharyngeal application reaches relevant concentrations at the mucosal surface, but systemic absorption from a swallowed gargle does not produce the serum concentrations needed for systemic antibacterial action. Sage is not a substitute for antibiotics in bacterial pneumonia, urinary tract infection, or skin/soft-tissue infection. Its useful niche is local: gargles for pharyngitis, mouthwashes for gingivitis, and topical applications for minor oral and skin infections.
Sage vs Streptococcus pyogenes
Streptococcus pyogenes (group A streptococcus, "strep") is the causative organism in 5 to 15% of adult sore throats and 15 to 30% of pediatric sore throats. Strep is the one bacterial pharyngitis that requires antibiotic treatment because of the small but real risk of rheumatic fever and post-streptococcal glomerulonephritis in untreated cases. Sage is not a substitute for penicillin or amoxicillin in confirmed strep throat — the systemic antibiotic prevents the post-streptococcal complications, which the topical gargle cannot.
That said, sage essential oil has been shown in vitro to inhibit S. pyogenes at MICs of 0.1 to 0.5%, and a sage gargle can be a reasonable symptomatic adjunct in a patient who has tested positive for strep and started appropriate antibiotic therapy. The acute pain and the discomfort with swallowing typically dominate the first 24 to 48 hours of strep throat treatment before antibiotic effects take hold, and the local symptomatic relief from a sage gargle covers that gap usefully.
For viral pharyngitis (the majority of adult sore throats), strep should be ruled out by rapid antigen test or culture if there is any clinical suspicion (Centor criteria: fever, tonsillar exudate, tender anterior cervical lymphadenopathy, absence of cough). Once strep is ruled out, sage gargle or spray is a reasonable symptomatic-only treatment, with the Hubbert trial as the supporting evidence base.
For more on pharyngitis evaluation and treatment, see our Sinusitis & Upper Respiratory Infection page and the Streptococcus pyogenes page.
Sage vs Candida albicans and Oral Thrush
Candida albicans is the most common cause of oral thrush, particularly in immunocompromised patients, denture wearers, patients on inhaled corticosteroids for asthma or COPD, and patients on broad-spectrum antibiotics. Topical antifungal nystatin suspension is the standard treatment, with oral fluconazole reserved for severe or refractory cases.
Sage essential oil has demonstrated in-vitro activity against Candida albicans at MICs of approximately 0.1 to 0.25%. A sage mouthwash or gargle (held in the mouth for 30 seconds, swished through the front of the mouth, and either spat out or swallowed) is a reasonable adjunct to topical antifungal therapy in mild oral thrush and may be a sufficient single intervention in early or mild presentations. The combined antimicrobial-plus-astringent action of the sage polyphenols also helps with the discomfort and dysgeusia that typically accompany active oral thrush.
Particular populations where this matters: inhaled-corticosteroid users (rinse the mouth with sage tea or sage mouthwash after each inhaled-steroid dose to reduce candidal colonization), denture wearers (overnight soaking of dentures in a 1:10 dilute sage tea reduces candidal biofilm), and post-antibiotic users (a 5- to 7-day course of sage mouthwash twice daily after completing a course of broad-spectrum antibiotics helps restore the normal oral flora balance).
Sage Mouthwash for Gingivitis & Oral Biofilm
Gingivitis — the early reversible inflammatory stage of periodontal disease — is caused by accumulated dental biofilm (plaque) of mixed-species bacterial origin. The standard treatment is improved mechanical oral hygiene (brushing, flossing, professional cleaning) with antimicrobial mouthwash adjunct as needed. Chlorhexidine mouthwash is the gold-standard pharmaceutical antimicrobial rinse but has the side effects of tongue and tooth staining and altered taste sensation with prolonged use, limiting it to short courses.
Multiple smaller trials have evaluated sage-containing mouthwashes for gingivitis. The aggregate finding is that sage mouthwash reduces gingival inflammation indices, reduces plaque accumulation, and is well tolerated for long-term daily use without the staining and dysgeusia problems of chlorhexidine. Commercial sage mouthwash products are widely available in European pharmacies; homemade sage tea cooled to room temperature can be used as a daily rinse (one to two cups of cooled sage tea swished through the mouth twice daily after toothbrushing).
For active periodontal disease (with attachment loss or pocketing), sage mouthwash is an adjunct only, not a substitute for professional scaling and root planing. The mechanical biofilm disruption from professional cleaning is the necessary primary intervention.
The Plague-Doctor Vinegar & Sage History
The legendary "Four Thieves Vinegar" of 17th-century plague-era France (versions also documented in Italy and England) was a herbal vinegar that, according to several recipe variants, contained sage, rosemary, thyme, lavender, mint, garlic, wormwood, and rue infused in red-wine vinegar. The legend held that four thieves in Marseilles or Toulouse used the preparation to protect themselves from plague while robbing the dead, were caught, and traded the recipe for their freedom. The recipe survived in European folk pharmacopoeias well into the 19th century.
Modern microbiology cannot validate or refute the plague-specific claim — Yersinia pestis spreads primarily through flea bites in bubonic plague and through respiratory droplets in pneumonic plague, neither of which a topical or oral herbal vinegar would meaningfully address. But the recipe is reasonable as a broad-spectrum oral and topical antimicrobial in a pre-antibiotic era: each ingredient has independent in-vitro antimicrobial activity, the vinegar base lowers pH to bactericidal levels, and the combination was used both as a topical wash and as an oral rinse/swallow.
The historical role of sage in this kind of formulation, and in the medieval plague-doctor literature more broadly, was as a reliable broad-spectrum antimicrobial in a pharmacy that had no antibiotics. That role is largely obsolete now for serious systemic infection, but the niche of topical oral, oropharyngeal, and skin infection — where sage essential oil reaches working concentrations — is still clinically real.
Practical Preparations — Gargle, Lozenge, Spray, Mouthwash
- Sage gargle (for acute sore throat) — 1 tablespoon dried S. officinalis leaf in 250 mL just-off-boil water, steeped covered for 10 minutes, strained. Add 1 tablespoon apple-cider vinegar and 1 teaspoon honey. Gargle 30 seconds, swish 15 seconds, spit or swallow. Repeat every 2 to 3 hours during waking hours for the first 48 hours of an acute sore throat. Discontinue when symptoms resolve.
- Sage throat spray (Hubbert protocol) — commercial sage essential-oil sprays at 5 to 15% concentration applied as 2 sprays to the back of the throat every 2 to 3 hours during waking hours. The German Salviathymol N is the best-known commercial product.
- Sage lozenge — widely available commercial lozenges containing sage essential oil, often combined with honey, lemon, or eucalyptus. Reasonable for symptomatic mild sore throat or as a substitute when a gargle is impractical (during travel, work, etc.).
- Sage mouthwash (for gingivitis or recurrent oral thrush) — cooled sage tea prepared as above, used as a 30-second rinse twice daily after toothbrushing. Long-term daily use is well tolerated.
- Topical application for minor skin infection or insect bite — cooled strong sage tea applied with a clean cloth as a compress; or a 1:10 dilution of sage essential oil in a carrier oil (jojoba, sweet almond) applied 2 to 3 times daily. Not for use on broken skin in young children or on burns.
Cautions for Topical & Oropharyngeal Use
- Do not substitute sage for antibiotic therapy in confirmed strep throat or any bacterial infection requiring systemic antibiotics — the gargle and spray have local effect only and do not prevent post-streptococcal complications
- Pregnancy and breastfeeding — topical gargle and spray use (where the patient does not swallow significant volume) is generally considered acceptable. Avoid swallowed sage tea in repeated daily use because of the uterotonic and lactation-suppression concerns covered in the Menopause & Hot Flashes page.
- Children under 6 — essential-oil sprays and concentrated tinctures are not recommended for young children because of swallowing risk and the thujone exposure profile. Cooled dilute sage tea (one teaspoon of dried leaf in 250 mL water) is acceptable as a gargle in children old enough to gargle reliably (typically age 6 and up).
- Asthma — the essential-oil aerosol from a throat spray can occasionally trigger bronchospasm in patients with reactive airway disease. Test with one or two sprays initially before continuing the protocol.
- Hypersensitivity — rare but documented allergic contact stomatitis to sage and the related labiate herbs. Discontinue if oral burning, edema, or rash develops.
- Dental restorations — long-term daily use of sage tea as a mouthwash can produce mild tooth staining, similar to but less severe than chlorhexidine. Less of an issue with intermittent acute-treatment use.
Key Research Papers
- Hubbert M, Sievers H, Lehnfeld R, Kehrl W (2006). Efficacy and tolerability of a spray with Salvia officinalis in the treatment of acute pharyngitis — a randomised double-blind, placebo-controlled study with adaptive design and interim analysis. European Journal of Medical Research. — PubMed
- Schapowal A, Berger D, Klein P, Suter A (2009). Echinacea/sage or chlorhexidine/lidocaine for treating acute sore throats: a randomized double-blind trial. European Journal of Medical Research. — PubMed
- Bozin B, Mimica-Dukic N, Samojlik I, Jovin E (2007). Antimicrobial and antioxidant properties of rosemary and sage (Rosmarinus officinalis L. and Salvia officinalis L., Lamiaceae) essential oils. Journal of Agricultural and Food Chemistry. — PubMed
- Beheshti-Rouy M, Azarsina M, Rezaei-Soufi L, Alikhani MY, Roshanaei G, Komaki S (2015). The antibacterial effect of sage extract (Salvia officinalis) mouthwash against Streptococcus mutans in dental plaque: a randomized clinical trial. Iranian Journal of Microbiology. — PubMed
- Pedrazzi V, Leite MF, Tavares RC, Sato S, do Nascimento GC, Issa JP (2015). Herbal mouthwash containing extracts of Baccharis dracunculifolia as agent for the control of biofilm: clinical evaluation in humans. Scientific World Journal. (Comparison context for herbal antimicrobial mouthwashes.) — PubMed
- Khan A, Sarwar HS et al. (2019). Antimicrobial activity of Salvia officinalis essential oil: a review. — PubMed
- Walch SG et al. (2011). Antioxidant capacity and polyphenolic composition as quality indicators for aqueous infusions of Salvia officinalis. Frontiers in Pharmacology. — PubMed
- Cui H et al. (2015). Antibacterial mechanism of sage essential oil on Escherichia coli. — PubMed
- Centor RM et al. (1981). The diagnosis of strep throat in adults in the emergency room. Medical Decision Making. (Centor criteria for strep-throat clinical evaluation.) — PubMed
- Shelburne SA et al. (2010). Streptococcal infections and their treatment. — PubMed
- Lopes-Lutz D et al. (2008). Screening of chemical composition, antimicrobial and antioxidant activities of Artemisia and sage essential oils. Phytochemistry. — PubMed
- European Medicines Agency (2016). Community herbal monograph on Salvia officinalis L., folium. EMA/HMPC monograph. — PubMed
PubMed Topic Searches
- PubMed: Sage and pharyngitis
- PubMed: Sage essential oil antimicrobial spectrum
- PubMed: Sage and Candida albicans
- PubMed: Sage mouthwash for gingivitis
- PubMed: 1,8-cineole & thujone antimicrobial
- PubMed: Chlorhexidine vs herbal mouthwash
Connections
- Sage Overview
- Sage Benefits Hub
- Sage for Cognitive Function
- Sage for Menopause
- Sage for Blood Sugar & Lipids
- Thyme (Sister Essential-Oil Herb)
- Oregano (Carvacrol)
- Echinacea
- Eucalyptus (1,8-Cineole)
- Sinusitis & URI
- Streptococcus Pyogenes
- Staphylococcus Aureus
- Immune Boosting
- Honey (Throat Demulcent)
- All Herbs