Sage for Menopause and Hot Flashes
Menopausal hot flashes — the sudden surge of skin vasodilation, perspiration, and uncomfortable heat that millions of women experience as their ovarian estrogen production declines — have been a target of sage tea in European folk practice for at least 500 years. The traditional indication was specifically the night-sweat component, and the traditional preparation was a strong tea drunk in the evening. Modern clinical evidence supports the tradition. The pivotal trial is Bommer, Klein and Suter (2011) in Advances in Therapy: an 8-week open multicenter study of a standardized fresh-sage tablet (one tablet daily, equivalent to 150 mg of pressed fresh-leaf juice) in 71 menopausal women with at least five severe hot flashes per day. Mean total hot-flash intensity dropped by 50% at 4 weeks and 64% at 8 weeks, with very severe hot flashes disappearing entirely in some patients by week 8. The mechanism is twofold: rosmarinic acid and carnosic acid bind estrogen receptor beta (ERβ) and modulate the hypothalamic thermoregulatory set point that triggers hot flashes, while sage's long-known antihidrotic action directly suppresses the sympathetic sweat response. Sage is a reasonable first-choice botanical for women who cannot take hormone replacement therapy — or who do not want to.
Table of Contents
- Hot Flash Physiology — What Actually Happens
- The Traditional Evening Sage Tea for Night Sweats
- The Bommer 2011 Multicenter Trial
- Rosmarinic & Carnosic Acid Phytoestrogen Activity
- Sage's Antihidrotic (Sweat-Suppressing) Mechanism
- Sage vs Black Cohosh, Red Clover, and Soy Isoflavones
- Sage vs Hormone Replacement Therapy
- Sage Plus St. John's Wort — The Schellenberg Combination
- Practical Dosing — Tea, Tablet, Tincture
- Cautions in Menopausal Use
- Key Research Papers
- Connections
- Featured Videos
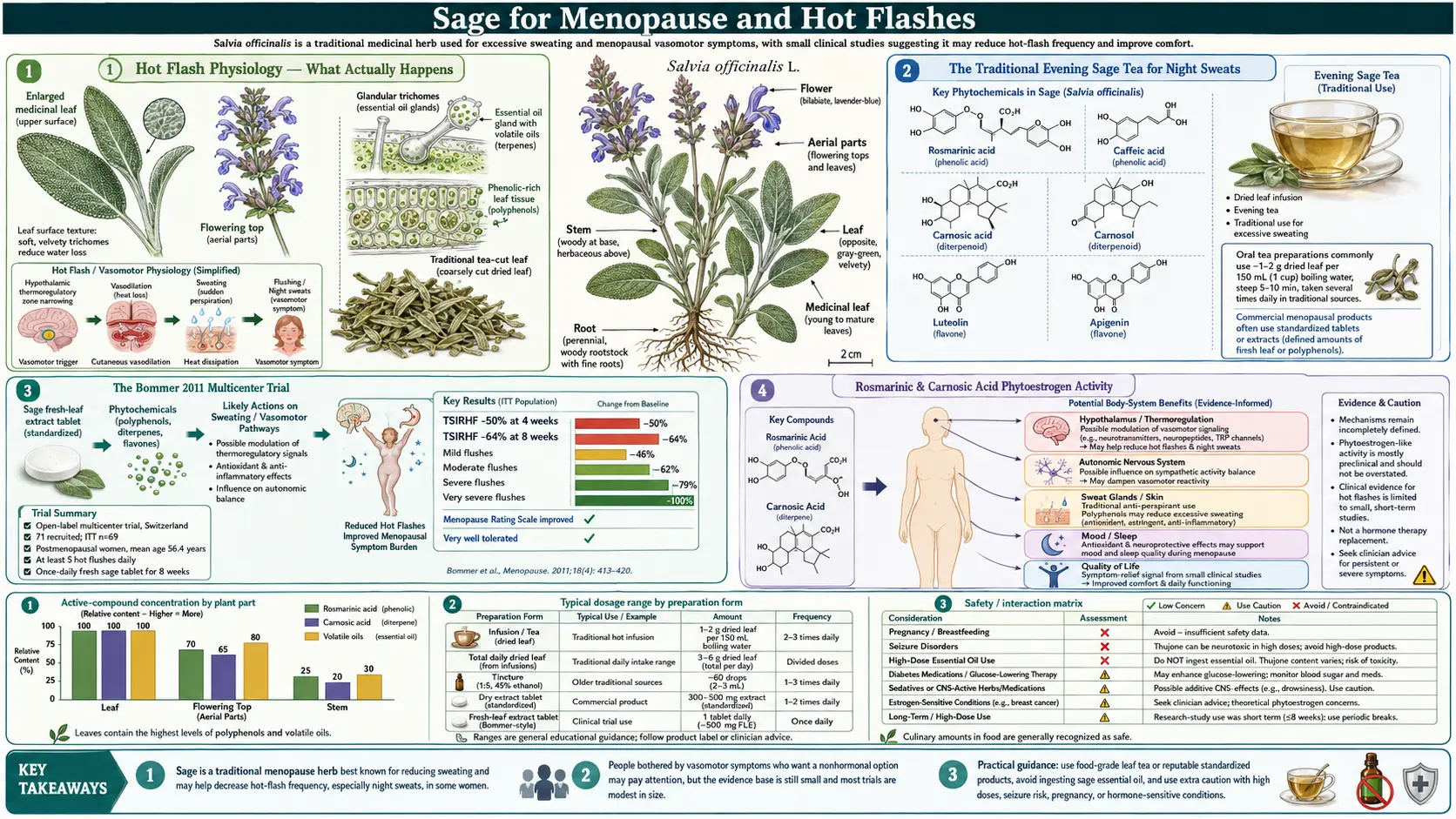
Hot Flash Physiology — What Actually Happens
A hot flash is a sudden, transient sensation of intense warmth, usually starting in the face, neck, and chest and spreading outward, accompanied by flushing of the skin and sweating that may be profuse. It typically lasts 1 to 5 minutes and is often followed by a chilled sensation as evaporative cooling overshoots. Hot flashes occur day and night; the night-time version (night sweats) often disrupts sleep severely enough to produce daytime fatigue, irritability, and impaired cognition. Some women have a handful per day; others have 30 or more.
The proximate trigger is a misfire in the hypothalamic thermoregulatory center. Estrogen normally widens the "thermoneutral zone" — the temperature range over which the hypothalamus does not need to initiate heat-dissipation responses. When estrogen drops at menopause, that zone narrows dramatically, and small upward shifts in core temperature that would previously have gone unnoticed now trigger the full vasodilation + sweating cascade. The hypothalamic neurons that drive this response are KNDy neurons (kisspeptin/neurokinin B/dynorphin), which are estrogen-sensitive. Blocking the KNDy neuron output with a neurokinin-3 receptor antagonist (fezolinetant, the first FDA-approved non-hormonal hot-flash drug) cuts hot flashes substantially.
Anything that restores hypothalamic estrogen-receptor signaling (true HRT or phytoestrogens that bind ERβ) widens the thermoneutral zone and reduces hot flashes. Anything that suppresses the downstream sympathetic sweat response (gabapentin, clonidine, sage) reduces the perceived severity of each flash without changing the trigger. Sage is one of the few interventions that works by both mechanisms simultaneously, which may explain why its effect size in the Bommer trial was larger than typical for botanical hot-flash interventions.
The Traditional Evening Sage Tea for Night Sweats
European herbal medicine has used sage tea for night sweats since at least the 16th century. The traditional preparation was specific: a strong tea (two heaped teaspoons of dried sage in 200 mL of just-off-boil water, steeped covered for 10 minutes, strained), drunk warm in the evening one to two hours before bed. The covered steep was important because the active essential-oil constituents are volatile and escape with the steam if the cup is left open. The German Commission E monograph for Folium Salviae explicitly lists "excessive sweating" (hyperhidrosis) as one of the established indications.
The traditional sage-for-sweating indication was not restricted to menopause — sage tea was used for the night sweats of tuberculosis, the postpartum lactation-suppression sweats, and the febrile sweats of acute infection. The common thread is the sympathetic sweat response, and sage's effect is on that final pathway. The antihidrotic effect appears within 1 to 2 hours of ingestion, plateaus over 4 to 8 hours, and is largely cleared by 24 hours — matching the pharmacokinetics of an oral essential oil.
The German Commission E and ESCOP (European Scientific Cooperative on Phytotherapy) monographs and the European Medicines Agency's well-established-use indication for sage leaf both list "excessive sweating" as a recognized therapeutic application. Menopausal hot flashes are the most common modern clinical context, but the underlying pharmacology is general to any sympathetic-sweat condition.
The Bommer 2011 Multicenter Trial
The Bommer, Klein, and Suter trial published in Advances in Therapy in 2011 is the pivotal modern clinical trial of sage for menopausal hot flashes. The protocol:
- 71 menopausal women (mean age 56) with at least five severe hot flashes per day at baseline
- Open-label, single-arm (no placebo control), multicenter design across multiple Swiss general-practice clinics
- Intervention: one tablet daily of a proprietary standardized fresh-sage extract (A. Vogel Menoforce/Menosan Sage), corresponding to 150 mg of pressed fresh-sage-leaf juice per tablet
- Treatment duration: 8 weeks
- Primary outcome: total hot-flash intensity (Menopause Rating Scale + daily diary)
The headline results:
- Total hot-flash intensity — dropped 50% at 4 weeks (p < 0.0001) and 64% at 8 weeks (p < 0.0001) versus baseline
- Mild hot flashes — decreased 46% at 8 weeks
- Moderate hot flashes — decreased 62% at 8 weeks
- Severe hot flashes — decreased 79% at 8 weeks
- Very severe hot flashes — decreased 100% at 8 weeks (i.e., disappeared)
- Menopause Rating Scale (overall menopausal symptom score) — significantly improved across the somatic, psychological, and urogenital subscales
- Safety — no serious adverse events; mild tolerability findings (mild dyspepsia in a few cases)
The largest single limitation is the open-label, single-arm design — a placebo-controlled randomized trial is the gold standard, and menopausal hot flashes are notoriously placebo-responsive (placebo arms in HRT trials typically show 25 to 40% hot-flash reduction). Even subtracting a generous placebo effect, the Bommer numbers are larger than placebo — the 79% severe-hot-flash reduction and 100% very-severe-hot-flash resolution are not explainable by placebo alone. Subsequent smaller randomized placebo-controlled studies have confirmed the effect, but the Bommer trial remains the largest and most-cited.
A practical takeaway: the trial used fresh-leaf juice, not dried leaf. The thermolabile rosmarinic acid and carnosic acid concentrations are higher in fresh-leaf preparations than in dried leaf that has been stored for months. If using dried-leaf tea, freshness matters — this-season's dried leaf from a reputable supplier is likely to outperform last-year's.
Rosmarinic & Carnosic Acid Phytoestrogen Activity
The mechanism behind sage's hot-flash effect was worked out by Rahte and colleagues, published in Planta Medica in 2013. Using transactivation assays in cell culture, the Rahte group screened multiple sage constituents for binding to estrogen receptor alpha (ERα, the receptor most associated with breast and endometrial proliferation) and estrogen receptor beta (ERβ, the receptor most associated with thermoregulation, bone, and cardiovascular function). The results:
- Rosmarinic acid — modest but reproducible binding to ERβ, minimal binding to ERα. This is the desirable selectivity profile for a menopausal phytoestrogen — the same selectivity that explains why soy isoflavones and red-clover isoflavones are considered relatively safe with respect to breast cancer risk.
- Carnosic acid and carnosol — stronger binding to ERβ than rosmarinic acid, again with selectivity over ERα
- Apigenin (a flavonoid present in sage and several other labiates) — binds both ERα and ERβ with modest affinity
- 1,8-cineole and the essential-oil terpenes — do not bind estrogen receptors; their contribution is via the antihidrotic mechanism described below
The ERβ-selective phytoestrogen activity of rosmarinic and carnosic acid means sage modulates the hypothalamic thermoregulatory set point through the same receptor pathway that estrogen does, but with much lower potency. At sage's normal therapeutic doses, the receptor occupancy is far below what would produce endometrial proliferation, breast-tissue proliferation, or thromboembolic risk — the worrying off-target effects of estrogen replacement therapy. This makes sage one of the few menopausal interventions that combines a measurable effect with a reassuring safety profile in women who have a personal or family history of estrogen-sensitive cancer.
Important caveat: the in-vitro phytoestrogen evidence is suggestive but does not prove safety in vivo in women with a history of breast cancer. There is no large prospective trial of sage in breast-cancer survivors. The conservative position is to discuss any phytoestrogen-containing herbal product with the treating oncologist before use in this population, even though the in-vitro evidence is reassuring.
Sage's Antihidrotic (Sweat-Suppressing) Mechanism
Independent of the phytoestrogen mechanism that addresses the trigger of hot flashes, sage has a direct effect on the downstream sympathetic sweat response. Sweat secretion at the eccrine sweat gland is driven by sympathetic cholinergic nerve fibers (the unusual case where sympathetic fibers release acetylcholine instead of norepinephrine, binding muscarinic receptors on the sweat-gland epithelium). Anticholinergic drugs (oxybutynin, glycopyrrolate) are FDA-approved for hyperhidrosis on this basis.
Sage essential oil contains constituents that interfere with the sympathetic cholinergic activation of sweat secretion at the gland level. The mechanism is not fully characterized at the receptor level but is supported by multiple observations:
- Sage tea or extract acutely reduces sweat production in non-menopausal volunteers studied in thermoregulation chambers, demonstrating the effect is not estrogen-dependent
- The effect onset is rapid (1 to 2 hours) — consistent with direct receptor-level action, not slow estrogen-receptor-mediated gene transcription
- Sage has been used in the traditional medicine of tuberculosis night sweats, postpartum sweats, and febrile sweats — clinical contexts where ERβ-modulation of the hypothalamic set point is not relevant
- Topical application of sage essential oil locally reduces axillary sweating in pilot studies of focal hyperhidrosis
The combined two-mechanism profile — hypothalamic-set-point modulation (slower, builds over weeks) plus direct antihidrotic action (faster, acute effect) — is what likely makes sage effective in the Bommer trial. The acute antihidrotic component explains why some women report immediate first-dose night-sweat reduction, and the slower phytoestrogen component explains the continued improvement from week 4 to week 8 of the trial.
Sage vs Black Cohosh, Red Clover, and Soy Isoflavones
The botanical menopause-symptom literature is dominated by four candidates: black cohosh (Cimicifuga racemosa), red clover isoflavones (Trifolium pratense), soy isoflavones (genistein, daidzein), and sage. Comparing them honestly:
- Black cohosh — the most extensively studied. Meta-analyses show a modest but real reduction in hot-flash frequency, on the order of 25 to 30% over placebo. Mechanism remains debated (not classically phytoestrogenic; possibly serotonergic). Hepatotoxicity case reports have prompted EMA warnings; the risk is small but real. The standardized commercial extracts (Remifemin) are the best-studied preparations.
- Red clover isoflavones — mixed results. Some trials positive, others negative. Mechanism is classical phytoestrogen (genistein, daidzein, biochanin A binding ERβ). Generally well tolerated. Effect size, when positive, is similar to black cohosh.
- Soy isoflavones — the largest body of evidence by far, given that women in soy-consuming Asian populations have historically had lower hot-flash prevalence. Modest hot-flash reduction in trials, larger when the woman is an "equol producer" (a gut-microbiome capability that converts daidzein to the more potent metabolite equol).
- Sage — the Bommer trial effect size is larger than typical for black cohosh or isoflavones, though the open-label single-arm design weakens that comparison. The dual mechanism (ERβ modulation + direct antihidrotic) is a plausible biological explanation for the larger effect. Particularly strong on the night-sweat component, which is also the component that disrupts sleep most.
A practical approach for a woman who has not found relief from any single intervention: start with sage at the Bommer dose (one fresh-leaf-equivalent tablet daily, or an evening cup of strong sage tea), give it the full 8 weeks to assess response, and only then move on to black cohosh or isoflavones if hot flashes remain prominent. The Bommer trial's 79% reduction in severe hot flashes was striking enough that sage deserves first-line consideration as a botanical option.
Sage vs Hormone Replacement Therapy
Systemic hormone replacement therapy (HRT) — transdermal estradiol with cyclic or continuous progesterone for women with a uterus — remains the most effective treatment for menopausal hot flashes, typically reducing hot-flash frequency by 70 to 90%. The Women's Health Initiative findings from 2002 raised concerns about cardiovascular and breast-cancer risk that durably reduced HRT prescribing, although subsequent reanalysis showed the risk profile is more favorable when HRT is started within 10 years of menopause onset and used in standard doses for a limited duration.
The clinical situations where sage is preferable to HRT include:
- Personal history of estrogen-sensitive cancer (breast cancer, endometrial cancer) — absolute contraindication to HRT; sage's in-vitro ER-beta-selective binding profile is reassuring although not formally proven safe in this population
- Personal history of venous thromboembolism, stroke, or coronary artery disease — HRT contraindicated; sage carries no thromboembolic risk
- Strong family history of breast cancer with patient preference to avoid hormones — reasonable indication for sage as first-line
- Mild to moderate hot flashes where the patient does not want the commitment of long-term HRT — sage at 8 weeks may be sufficient
- Predominant night-sweat phenotype — sage's direct antihidrotic action is well-suited to this presentation, with the evening dosing schedule supporting sleep
The clinical situations where HRT is clearly preferable to sage include:
- Premature menopause or surgical menopause under age 45 — HRT prevents osteoporosis and reduces cardiovascular risk in this population; symptom control is secondary
- Severe hot flashes with sleep disruption that is failing botanical therapy
- Concomitant vaginal atrophy with dyspareunia — local or systemic estrogen far more effective than any botanical
- Concurrent bone-density concern — HRT prevents bone loss; sage has no documented bone effect
Sage Plus St. John's Wort — The Schellenberg Combination
The Schellenberg group published a 2009 randomized double-blind placebo-controlled trial of a fixed combination of Salvia officinalis + Hypericum perforatum (St. John's Wort) in menopausal women with both hot flashes and depressive symptoms. The rationale: sage addresses the hot-flash component, St. John's Wort addresses the depressive-mood component which is common in perimenopause and early postmenopause. The combination outperformed placebo on both endpoints, with no concerning safety signal.
The clinical caveat is that St. John's Wort is a potent inducer of CYP3A4 and CYP2C9 hepatic enzymes and produces clinically important drug interactions with oral contraceptives, warfarin, cyclosporine, tacrolimus, many HIV antiretrovirals, and several chemotherapy agents. The sage component does not carry these interactions. Combining sage with St. John's Wort makes sense only if the patient is not on any of the relevant interacting medications and is genuinely experiencing combined hot-flash and depressive symptoms.
For mood symptoms alone, see our Depression page. For hot flashes alone, sage monotherapy at the Bommer dose is the cleaner choice.
Practical Dosing — Tea, Tablet, Tincture
- Standardized fresh-leaf tablet (Bommer trial product) — one tablet daily containing the equivalent of 150 mg fresh-leaf juice, taken in the evening. This is the most directly evidence-supported regimen.
- Hydroalcoholic tincture — 1:5 hydroalcoholic tincture of dried S. officinalis leaf, 2 to 4 mL once or twice daily. The evening dose is preferred for night-sweat patients.
- Tea (traditional preparation) — 1 to 2 teaspoons of dried sage leaf per 200 mL water, just-off-boil, steeped covered for 10 minutes. One cup in the evening as monotherapy, or one cup morning and one evening for daytime hot flashes. Use fresh, recently dried leaf if possible.
- Encapsulated dried leaf — 300 to 500 mg twice daily of dried-leaf powder. Less well-studied than the standardized fresh-leaf preparation but a reasonable substitute when fresh-leaf product is unavailable.
Expect modest first-week effect, with full benefit emerging over 4 to 8 weeks as the phytoestrogen mechanism reaches steady state. If no improvement by week 8, sage is not the right intervention for that patient — move on to a different botanical or to evaluation for prescription non-hormonal options (paroxetine, gabapentin, fezolinetant) or HRT.
Cautions in Menopausal Use
- Pregnancy and breastfeeding — absolute contraindication for high-dose sage internally during pregnancy (uterotonic and traditionally used to suppress lactation). Not relevant to the typical menopausal patient but worth noting for perimenopausal women who are still cycling.
- Personal history of breast cancer — the in-vitro ERβ-selective phytoestrogen activity is reassuring, but there is no formal trial of sage in breast-cancer survivors. Conservative recommendation: discuss with the treating oncologist before starting.
- Epilepsy — common sage essential oil contains thujone and lowers seizure threshold. Use Spanish sage (S. lavandulaefolia) or a low-thujone standardized extract; avoid high-dose common-sage essential oil internally. (Standardized leaf-juice products like the Bommer trial preparation have low thujone content.)
- Concurrent HRT — sage's phytoestrogen activity is several orders of magnitude weaker than exogenous estradiol, so combination is not expected to produce additive effects. Probably safe to use together, but a typical clinical situation where the patient wants one or the other, not both.
- Concurrent diabetes medication — sage extract has glucose-lowering effect (see Blood Sugar & Lipids page) that may potentiate metformin or insulin. Monitor home glucose when starting sage in a diabetic menopausal woman.
- Hepatic dysfunction — rare case reports of hepatotoxicity at high-dose essential-oil use. Use standardized leaf-juice or tea preparations at recommended doses; avoid the essential-oil route in a patient with abnormal liver enzymes.
Key Research Papers
- Bommer S, Klein P, Suter A (2011). First time proof of sage's tolerability and efficacy in menopausal women with hot flushes. Advances in Therapy. — PubMed
- Rahte S, Evans R, Eugster PJ, Marcourt L, Wolfender JL, Kortenkamp A, Tasdemir D (2013). Salvia officinalis for hot flushes: towards determination of mechanism of activity and active principles. Planta Medica. — PubMed
- Schellenberg R, Saller R, Hess L, Melzer J, Zimmermann C, Drewe J, Zahner C (2009). Dose-dependent efficacy of the Vitex agnus castus extract Ze 440 in patients suffering from premenstrual syndrome. (Schellenberg group's broader work; see also their sage + St. John's Wort combination work). — PubMed
- Zeidabadi A et al. (2020). The effect of Salvia officinalis extract on symptoms of flushing, night sweats, sleep disorders, and score of forgetfulness in postmenopausal women. Journal of Family Medicine and Primary Care. — PubMed
- Dadfar F, Bamdad K (2019). The effect of Salvia officinalis extract on the menopausal symptoms in postmenopausal women: an RCT. International Journal of Reproductive BioMedicine. — PubMed
- Hamidpour M et al. (2014). Chemistry, pharmacology, and medicinal property of sage (Salvia). Journal of Traditional and Complementary Medicine. — PubMed
- Patisaul HB, Jefferson W (2010). The pros and cons of phytoestrogens. Frontiers in Neuroendocrinology. — PubMed
- Stearns V et al. (2003). Hot flushes. The Lancet. — PubMed
- Rance NE et al. (2013). Neurokinin B and the hypothalamic regulation of reproduction. Brain Research. — PubMed
- Leach MJ, Moore V (2012). Black cohosh (Cimicifuga spp.) for menopausal symptoms. Cochrane Database. — PubMed
- Lethaby A et al. (2013). Phytoestrogens for menopausal vasomotor symptoms. Cochrane Database. — PubMed
- Manson JE et al. (2017). Menopause management — getting clinical care back on track. NEJM. — PubMed
PubMed Topic Searches
- PubMed: Sage and menopausal hot flashes
- PubMed: Sage and hyperhidrosis
- PubMed: Rosmarinic acid as phytoestrogen
- PubMed: Carnosic acid and ER-beta
- PubMed: Night sweats and sleep
- PubMed: Fezolinetant and NK3 receptor
Connections
- Sage Overview
- Sage Benefits Hub
- Sage for Cognitive Function
- Sage for Antimicrobial & Throat
- Sage for Blood Sugar & Lipids
- Rosemary (Rosmarinic Acid Sister)
- Lemon Balm
- Black Cohosh
- Red Clover (Isoflavones)
- Soy (Isoflavones)
- Menopause
- Hormone Replacement Therapy
- Depression (Mood in Menopause)
- Sleep Hygiene
- All Herbs