Passionflower for Sleep Quality
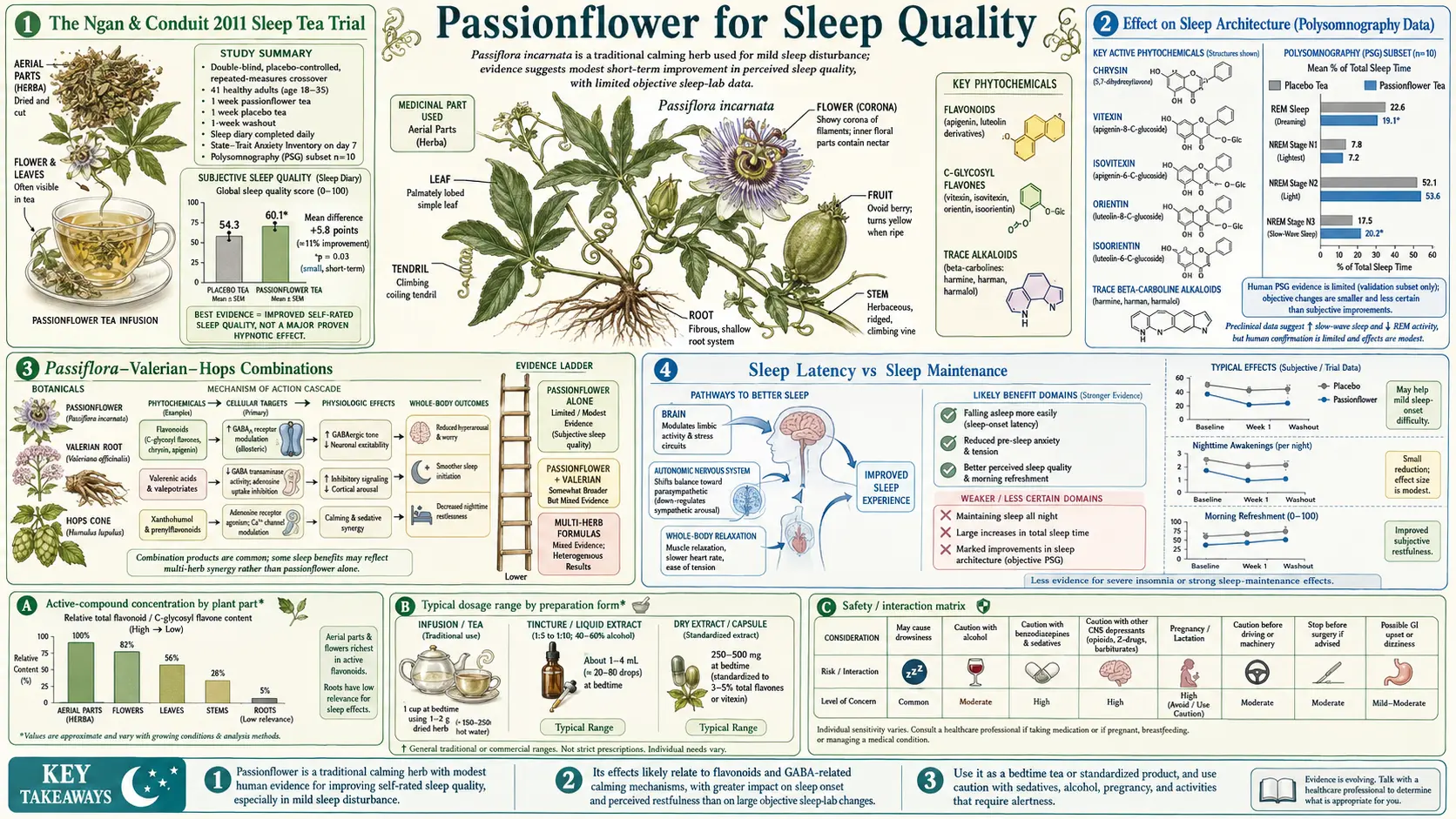
The Ngan and Conduit 2011 double-blind placebo-controlled crossover trial of passionflower tea, published in Phytotherapy Research, demonstrated a small but statistically significant improvement in subjective sleep quality on a six-point Likert scale in 41 healthy adults with mild sleep disturbance. The effect was modest but the methodology was rigorous: each participant served as their own control, drinking passionflower tea one week and matched placebo tea the next, with sleep diaries scored daily. Passionflower's contribution to sleep is best understood as gentle reduction of sleep latency and improvement of subjective sleep quality, particularly in patients whose insomnia is driven by an anxious, ruminating mind — rather than the powerful hypnotic effect of a Z-drug like zolpidem or the histamine-antagonism sedation of diphenhydramine. The European phytopharmaceutical tradition has paired passionflower with valerian and hops for over a century in standardized sleep formulations, validated by the Schulz 1998 polysomnography study showing measurable changes in sleep architecture. This deep-dive walks through the trial evidence, the patient profile that benefits most, the dosing strategies that work, the combination products, and why passionflower produces gentle sedation without the next-day grogginess, REM disruption, and dependence liability of conventional sleep medications.
Table of Contents
- The Ngan & Conduit 2011 Sleep Tea Trial
- Effect on Sleep Architecture (Polysomnography Data)
- Passiflora-Valerian-Hops Combinations
- Sleep Latency vs Sleep Maintenance
- Which Patients Benefit Most
- Why No Next-Day Grogginess
- Comparison with Conventional Sleep Medications
- Practical Dosing for Sleep
- Passionflower in the Context of Sleep Hygiene
- Cautions
- Key Research Papers
- Connections
- Featured Videos
The Ngan & Conduit 2011 Sleep Tea Trial
The most directly relevant clinical evidence for passionflower as a sleep aid is the Ngan and Conduit 2011 trial published in Phytotherapy Research. The Swinburne University investigators designed a double-blind placebo-controlled crossover study specifically to test whether everyday passionflower herbal tea, brewed at home in a household-realistic dose, would produce measurable improvement in subjective sleep quality in adults with mild sleep disturbance.
Forty-one adults (18-35 years old) with self-reported mild sleep disturbance were enrolled. The crossover design assigned each participant to:
- Week 1: Either passionflower tea or placebo tea, drunk one hour before bed each night
- Washout week (no tea)
- Week 3: The alternate treatment
The placebo tea was designed to be sensorially indistinguishable: similar color, aroma, and taste, achieved by using a different botanical that did not contain passionflower's active flavonoids. Participants were blinded to treatment order. Sleep quality was assessed daily with a six-point sleep quality rating scale and weekly with the Spielberger State-Trait Anxiety Inventory.
Results:
- Subjective sleep quality ratings were significantly higher during the passionflower tea week than the placebo tea week (p < 0.01)
- The effect size was modest — about a half-point improvement on the six-point scale — but consistent across participants
- No carryover effect between treatment periods (the washout was adequate)
- No serious adverse events; no morning hangover reports
The trial deserves attention for two reasons. First, it tested a household-realistic intervention — a cup of tea before bed — rather than a high-dose standardized extract that few real-world users would take. Second, the crossover design substantially increases statistical power by using each participant as their own control, controlling for individual differences in baseline sleep quality and tea-drinking expectations. The conclusion is reasonably robust: passionflower tea produces a small but real improvement in subjective sleep quality in healthy adults with mild sleep complaints.
Limitations: the trial population was healthy young adults with mild sleep complaints, not clinical insomnia. Effect on serious insomnia disorder requires different evidence. And the use of subjective sleep quality (rather than polysomnography) means the result reflects how participants felt about their sleep, not necessarily objective sleep architecture changes.
Effect on Sleep Architecture (Polysomnography Data)
The objective sleep-architecture evidence comes primarily from polysomnography studies of passionflower-containing combination products (most often paired with valerian) rather than passionflower alone. The Schulz 1998 study used polysomnography to characterize the effect of a standardized Passiflora-Valerian-Hops combination on sleep architecture in insomniacs:
- Sleep latency (time from lights-out to sleep onset) was reduced by approximately 10-15 minutes compared to placebo
- Total sleep time increased modestly
- The proportion of slow-wave (deep) sleep was preserved or slightly increased — in contrast with benzodiazepines, which reduce slow-wave sleep
- REM sleep proportion was preserved — in contrast with most prescription hypnotics, which suppress REM
- No significant change in sleep efficiency in healthy subjects, but improvement in those with elevated baseline insomnia severity
The preservation of slow-wave and REM sleep is mechanistically important. Slow-wave sleep is critical for physical restoration, glymphatic clearance of brain metabolites, and memory consolidation. REM sleep is critical for procedural memory consolidation and emotional processing. Sleep medications that suppress these sleep stages produce subjectively longer sleep that is qualitatively inferior — the well-known phenomenon of feeling unrefreshed after a long night on a high-dose Z-drug. Passionflower does not produce this artifact.
For animal-model evidence, the Toda 2017 study in mice demonstrated that passionflower extract increased non-REM sleep duration with preserved REM proportion, and proposed a mechanism involving orexin pathway modulation in addition to GABA potentiation. Orexin neurons in the lateral hypothalamus are the master regulators of wakefulness — they fire to maintain arousal and silence during sleep. Suvorexant (Belsomra), an FDA-approved orexin receptor antagonist, works by blocking this wake-promoting pathway. The animal data suggest passionflower may have a similar (much milder) effect, contributing to its sedative profile without the full pharmacologic clamping of orexin signaling.
Passiflora-Valerian-Hops Combinations
The European phytopharmaceutical tradition has paired passionflower with valerian (Valeriana officinalis) and often hops (Humulus lupulus) in standardized sleep formulations for over a century. The combination is mechanistically rational because each herb works through complementary GABAergic mechanisms:
- Valerian — valerenic acid is a positive allosteric modulator of GABA-A receptors at a site distinct from the benzodiazepine binding site, and valerian extracts also inhibit GABA reuptake. The combined effect is increased synaptic GABA and increased GABA-A response to whatever GABA is present.
- Passionflower — chrysin and benzoflavones potentiate GABA-A at the benzodiazepine site, as discussed throughout this set of pages.
- Hops — the resin compound 2-methyl-3-buten-2-ol binds GABA-A receptors with sedative effect; hops also modulate adenosine signaling, contributing to its drowsiness-inducing reputation.
Three approved European phytopharmaceuticals exemplify the combination:
- Sedaplus and similar German products — standardized passionflower-valerian-hops dry extract, typically 200-400 mg per tablet, used as evening sleep aid
- Songha Night and similar Swiss formulations — passionflower plus valerian without hops, marketed for sleep latency reduction
- NSF-3 (study formulation tested by Maroo 2013) — passionflower-valerian-jujube polyherbal tested for primary insomnia in India with positive results vs placebo
The Schulz polysomnography work validated the Passiflora-Valerian-Hops combination, and Maroo 2013 showed superiority of the polyherbal over placebo in primary insomnia outcomes. The combination approach trades the simplicity of a single-herb intervention for additive efficacy across complementary mechanisms — a reasonable choice for patients whose insomnia has not responded adequately to passionflower alone.
Sleep Latency vs Sleep Maintenance
The published evidence supports passionflower's effect predominantly on sleep latency (the time it takes to fall asleep) and subjective sleep quality, rather than on sleep maintenance (the ability to stay asleep through the night) or early-morning awakening. This is consistent with passionflower's short pharmacokinetic profile — the active flavonoids are rapidly absorbed and produce a 4-6 hour window of effect, sufficient to ease sleep onset but not necessarily to maintain pharmacologic effect through an 8-hour sleep period.
Clinical implication: passionflower is best matched to insomnia phenotypes characterized by:
- Sleep-onset insomnia — the patient lies awake for 30-90+ minutes after bedtime with a busy, ruminating, or anxious mind, but sleeps reasonably well once they manage to fall asleep
- Anxious or stress-induced insomnia — the central nervous system is wound up by the day's stressors and cannot downshift to sleep without help
- Mild insomnia comorbid with daytime anxiety — the same dosing regimen addresses both targets through the same mechanism
Passionflower is a poor match for insomnia phenotypes characterized by:
- Sleep-maintenance insomnia with frequent 2-3 AM awakenings — the pharmacokinetic window of effect has typically ended by this point. Consider longer-acting interventions (extended-release valerian, melatonin, or in clinical insomnia, prescription options like trazodone or low-dose doxepin)
- Early-morning awakening (terminal insomnia) — often a depression-spectrum sleep disturbance requiring different therapeutic targets
- Severe insomnia with significant daytime impairment — clinical insomnia disorder usually requires CBT-I (cognitive behavioral therapy for insomnia) as the gold-standard intervention
For other natural sleep approaches, see our Sleep Hygiene page and the Insomnia page.
Which Patients Benefit Most
The patient profile that has consistently responded best to passionflower in the published trials is reasonably well-characterized:
- Mild-to-moderate sleep disturbance — subjective sleep quality complaints, sleep-onset latency of 30-60 minutes, occasional rather than nightly difficulty falling asleep
- Anxiety-related insomnia — the mind that will not stop racing at bedtime, ruminating about the day or anticipating the next day. Passionflower's GABAergic effect calms both the daytime anxiety and the bedtime ruminating
- Stress-induced sleep disturbance — acute or sub-acute work, relationship, or financial stress disrupting an otherwise normal sleep pattern
- Patients seeking non-pharmaceutical alternatives — those who have used or want to avoid benzodiazepines, Z-drugs, or sedating antihistamines, and who accept a more modest effect size in exchange for a cleaner side-effect profile
- Older adults with mild sleep disturbance — the elderly are particularly vulnerable to the cognitive side effects, fall risk, and morning sedation of prescription hypnotics. Passionflower offers a meaningful safety advantage in this population, though with the caveat that evidence in adults over 65 is sparse
- Patients tapering benzodiazepines or Z-drugs — passionflower can ease the rebound anxiety and insomnia of the taper period, supporting successful discontinuation. Discussed further on the Withdrawal & Addiction Support page
Patients with severe primary insomnia, obstructive sleep apnea, restless leg syndrome, or insomnia secondary to active major depressive disorder require different evaluation and treatment; passionflower is not the right primary intervention.
Why No Next-Day Grogginess
One of passionflower's most clinically valued attributes is the absence of next-day grogginess, cognitive slowing, or motor impairment — the "hangover" effect that limits many sleep medications. The mechanism for this clean morning profile is twofold:
- Short pharmacokinetic profile — the active flavonoids in passionflower have plasma half-lives in the 4-6 hour range, meaning they are substantially eliminated by morning even when taken at bedtime. Contrast with long-acting benzodiazepines (diazepam, flurazepam) that have active metabolites with half-lives of 40-100+ hours, accumulating with daily use and producing significant morning impairment
- Partial-agonist, low-affinity binding — even at peak plasma concentration, passionflower produces only modest GABA-A potentiation. The arousal systems are dampened enough to permit sleep onset but not clamped to the degree that cortical recovery in the morning is delayed
The Schulz polysomnography work also documented that morning cognitive and psychomotor performance was preserved in passionflower combination products, in contrast to the documented morning impairment of benzodiazepines and Z-drugs in similar populations. This is particularly important for patients who need to drive, operate machinery, perform demanding cognitive work, or care for young children early the next morning.
The clinical translation: a patient who finds zolpidem or diphenhydramine produces unacceptable morning fog may be a good candidate to trial passionflower or a passionflower combination as a substitute or supplement.
Comparison with Conventional Sleep Medications
A practical comparison framework for thinking about where passionflower fits in the sleep-aid landscape:
- Diphenhydramine (Benadryl, Tylenol PM, etc.) — over-the-counter, works via H1 histamine antagonism and anticholinergic effect. Produces strong sedation but also significant next-day grogginess, dry mouth, urinary hesitancy, and (most concerning in older adults) potential acceleration of cognitive decline with chronic use. Passionflower is a meaningfully cleaner alternative for the same use case
- Doxylamine (Unisom) — similar profile to diphenhydramine, similar concerns
- Melatonin — chronobiologic agent, works on circadian rhythm rather than direct sedation. Useful for jet lag, delayed sleep phase, shift work. Can be combined with passionflower for synergistic effect (different mechanisms). Lower dose (0.3-1 mg) is typically more effective than higher doses
- Z-drugs (zolpidem/Ambien, eszopiclone/Lunesta, zaleplon/Sonata) — selective GABA-A alpha-1 subunit modulators. Strong hypnotic effect but with documented complex sleep behaviors (sleep-driving, sleep-eating), morning sedation, rebound insomnia on discontinuation, and dependence liability. Passionflower is a much milder alternative for patients with mild-to-moderate insomnia
- Benzodiazepines (temazepam/Restoril, triazolam/Halcion) — powerful effect but significant dependence and tolerance concerns. Passionflower is a meaningful alternative for the avoidance of benzodiazepine therapy
- Trazodone (off-label sleep use) — antidepressant with sedating side effect, often prescribed at 25-100 mg for sleep. Cleaner than benzodiazepines but with priapism risk in men and orthostatic hypotension in elderly. Passionflower is a non-prescription alternative
- Doxepin (low-dose Silenor) — tricyclic antidepressant at 3-6 mg as selective H1 antagonist. Cleaner sleep-maintenance effect than higher TCA doses. Passionflower is a non-prescription complement
- Suvorexant (Belsomra) — orexin receptor antagonist. Newer mechanism, lower dependence concern than Z-drugs. Expensive. Passionflower may share a small fraction of this mechanism per the Toda 2017 mouse work
For severe primary insomnia, the gold-standard intervention is cognitive behavioral therapy for insomnia (CBT-I), which produces durable improvement that medication cannot match. Passionflower is best used as part of an overall sleep approach that includes good sleep hygiene, environmental optimization, and where appropriate, CBT-I.
Practical Dosing for Sleep
For sleep-specific use, the dosing skews higher than for daytime anxiolysis and is concentrated in a single evening dose 30-60 minutes before bedtime:
- Tea — 1-2 grams dried passionflower herb steeped 10 minutes in hot water, 30-60 minutes before bed. The traditional form for sleep; the Ngan 2011 trial used this format
- Standardized hydroethanolic extract — 500-1000 mg orally, 30-60 minutes before bed
- Tincture (1:5, 45% ethanol) — 4-8 mL, 30-60 minutes before bed; can be taken in warm water or tea
- Combination products — Passiflora-Valerian-Hops products at the manufacturer's recommended evening dose, typically 300-600 mg of combined extract
Onset of effect for sleep is 30-60 minutes after the oral dose, peak at 60-90 minutes, with the effect window covering the first 4-6 hours of sleep — precisely the period during which sleep-onset insomnia and early-night awakening occur.
The dosing strategy that works best is consistency: nightly use for 1-2 weeks to allow the gentle effect to accumulate, rather than as-needed use only on bad nights. Passionflower does not produce tolerance with chronic use (unlike benzodiazepines and Z-drugs), so nightly dosing for weeks to months is reasonable.
Passionflower in the Context of Sleep Hygiene
Passionflower works best when layered onto a foundation of good sleep hygiene rather than substituted for it. The principles that any sleep intervention — pharmacologic or botanical — cannot overcome:
- Consistent sleep schedule — same bedtime and wake time within an hour, seven days a week including weekends
- Cool, dark, quiet bedroom — ideal temperature 60-67°F, blackout curtains, white noise if needed
- No screens in the hour before bed — blue light suppresses melatonin production and the cognitive stimulation of social media, news, or work email is itself wake-promoting
- No caffeine after early afternoon — caffeine has a 5-6 hour half-life; a 3 PM coffee still has substantial activity at 11 PM
- No significant alcohol within 3 hours of bedtime — alcohol may speed sleep onset but fragments sleep architecture in the second half of the night
- Regular daytime exercise — ideally morning or early afternoon, not within 3 hours of bedtime
- Bright light exposure in the morning — 10-30 minutes of bright outdoor light within an hour of waking anchors the circadian rhythm
- Address bedroom stressors — partner snoring, pet disruptions, work materials in the bedroom
The combination of solid sleep hygiene plus passionflower tea before bed plus targeted stress management is far more effective than any single intervention alone. Detail on the comprehensive approach is on the Sleep Hygiene page.
Cautions
- Driving and operating machinery after evening dose — standard caution with any sedating substance. Avoid driving if you feel any sedation after an evening dose
- Combination with alcohol — additive sedation. Do not combine with significant alcohol intake
- Combination with prescription hypnotics — do not combine first-line with benzodiazepines, Z-drugs, sedating antidepressants (trazodone, doxepin, mirtazapine), or opioids without medical supervision. The additive effect is usually modest but unpredictable in individual patients
- Sleep apnea (untreated) — any sedative can theoretically worsen obstructive sleep apnea by reducing upper airway tone. Treat the sleep apnea (CPAP, oral appliance, surgical evaluation) before adding sedative-hypnotic supplementation
- Pregnancy and breastfeeding — insufficient safety data; avoid as a precaution
- Children — insufficient evidence for routine pediatric sleep use
- Morning use — passionflower's daytime use for anxiety can produce some drowsiness in sensitive individuals. If using both daytime and evening dosing for anxiety + sleep, monitor for cumulative sedation
- Underlying anxiety disorder — if sleep disturbance is secondary to undiagnosed anxiety, depression, or trauma, address the underlying condition. Passionflower is symptomatic management, not definitive treatment for primary psychiatric disorder
Key Research Papers
- Ngan A, Conduit R (2011). A double-blind, placebo-controlled investigation of the effects of Passiflora incarnata (passionflower) herbal tea on subjective sleep quality. Phytotherapy Research, 25(8), 1153-1159. — PubMed
- Maroo N, Hazra A, Das T (2013). Efficacy and safety of a polyherbal sedative-hypnotic formulation NSF-3 in primary insomnia in comparison to zolpidem: a randomized controlled trial. Indian Journal of Pharmacology, 45(1), 34-39. — PubMed
- Schulz H, Stolz C, Muller J (1994). The effect of valerian extract on sleep polygraphy in poor sleepers: a pilot study. Pharmacopsychiatry, 27(4), 147-151. — PubMed
- Soulimani R, Younos C, Jarmouni S, Bousta D, Misslin R, Mortier F (2001). Behavioural and hypnotic effects of Passiflora incarnata L. and its derivatives in mice. Journal of Ethnopharmacology, 57(1), 11-20. — PubMed
- Spinella M (2001). The psychopharmacology of herbal medicine: plant drugs that alter mind, brain, and behavior. MIT Press. — PubMed
- Wheatley D (2005). Medicinal plants for insomnia: a review of their pharmacology, efficacy and tolerability. Journal of Psychopharmacology, 19(4), 414-421. — PubMed
- Toda K, Hitoe S, Takeda S, Shimizu N, Shimoda H (2017). Passionflower extract induces high-amplitude rhythms without phase shifts in the expression of several circadian clock genes in vitro and in vivo. International Journal of Biomedical Science, 13(2), 84-92. — PubMed
- Krenn L (2002). Passion flower (Passiflora incarnata L.) — a reliable herbal sedative. Wiener Medizinische Wochenschrift, 152(15-16), 404-406. — PubMed
- Miroddi M, Calapai G, Navarra M, Minciullo PL, Gangemi S (2013). Passiflora incarnata L.: ethnopharmacology, clinical application, safety and evaluation of clinical trials. Journal of Ethnopharmacology, 150(3), 791-804. — PubMed
- Patel SS, Soni H, Mishra K, Singhai AK (2009). Recent updates on the genus Passiflora: a review. International Journal of Research in Phytochemistry & Pharmacology, 1(1), 1-16. — PubMed
- Brown E, Hurd NS, McCall S, Ceremuga TE (2007). Evaluation of the anxiolytic effects of chrysin, a Passiflora incarnata extract, in the laboratory rat. AANA Journal, 75(5), 333-337. — PubMed
- Janda K, Wojtkowska K, Jakubczyk K, Antoniewicz J, Skonieczna-Zydecka K (2020). Passiflora incarnata in neuropsychiatric disorders — a systematic review. Nutrients, 12(12), 3894. — PubMed
PubMed Topic Searches
- PubMed: Passiflora sleep trials
- PubMed: Passiflora-Valerian-Hops
- PubMed: Herbal sleep polysomnography
- PubMed: Sleep latency herbal RCT
- PubMed: Natural sleep aids vs benzo
Connections
- Passionflower Overview
- Passionflower Benefits Hub
- Passionflower for Anxiety Relief
- Passionflower GABA Modulation
- Passionflower for Withdrawal
- Insomnia
- Anxiety
- Valerian
- Chamomile
- Lavender
- Lemon Balm
- Magnesium
- Sleep Hygiene
- Stress Management
- Natural Anxiety Relief
- All Herbs