Kava for Sleep and Insomnia
The use of kava for sleep is closely tied to its anxiolytic effect — for a large fraction of patients with chronic insomnia, the proximate cause is stress, anxiety, and ruminative cognition that prevent sleep onset and produce middle-night awakenings. Kava addresses this anxiety-driven insomnia pathway through GABA-A allosteric modulation, with two key advantages over the benzodiazepine, z-drug (zolpidem, eszopiclone), and antihistamine alternatives: it preserves REM sleep and slow-wave (NREM stage 3) sleep architecture rather than suppressing them, and it does not produce next-day cognitive impairment or amnesia. The Lehrl 2004 trial of WS 1490 in stress-related insomnia and the Wheatley 2001 head-to-head comparison of kava with valerian provide the strongest clinical evidence. This deep-dive walks through the trial literature, the sleep architecture preservation, the comparison with conventional hypnotics, and the practical use of kava for difficult-to-treat insomnia in patients who cannot tolerate or should not use benzodiazepines and z-drugs.
Table of Contents
- The Anxiety-Insomnia Axis
- The Lehrl 2004 WS 1490 Trial
- The Wheatley 2001 Kava vs Valerian Trial
- Sleep Architecture Preservation (REM and NREM3)
- Kava versus Benzodiazepines for Sleep
- Kava versus Z-Drugs (Zolpidem, Eszopiclone)
- Kava versus Antihistamines (Diphenhydramine, Doxylamine)
- Kava versus Melatonin, Valerian, and Other Natural Sleep Aids
- Menopausal and Perimenopausal Insomnia
- Practical Protocol for Sleep Use
- Key Research Papers
- Connections
- Featured Videos
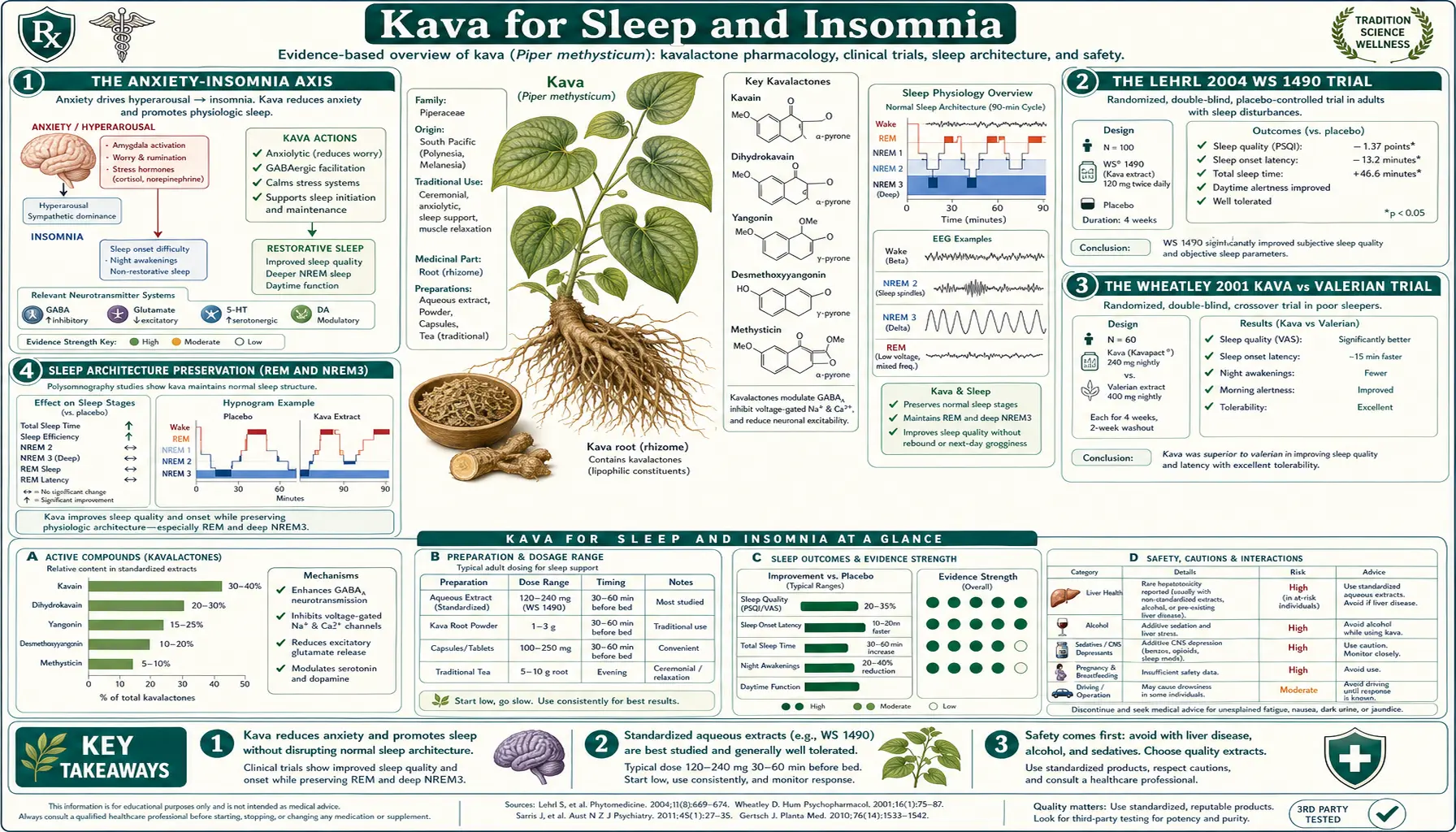
The Anxiety-Insomnia Axis
Chronic insomnia is overwhelmingly anxiety-driven in adults. The clinical picture is familiar: difficulty falling asleep because of ruminative cognition (work concerns, financial worries, relationship stress), repeated middle-night awakenings with the same cognitive ruminations preventing return to sleep, and early-morning awakening with sustained autonomic arousal. The conventional sleep-medicine literature distinguishes "primary insomnia" from "anxiety-related insomnia" diagnostically but the underlying neurobiology is largely shared — both involve persistent hyperarousal of the limbic system and elevated sympathetic tone, both respond to the same pharmacological targets, and both share substantial epidemiological overlap with generalized anxiety disorder.
The implication for therapy is that any agent that effectively reduces anxiety will improve sleep, and any agent that effectively improves sleep needs to address the upstream arousal rather than just sedate the patient. Sedation without anxiolysis (the profile of antihistamines and to some extent z-drugs) tends to produce next-day grogginess without restorative sleep. Anxiolysis with mild sedation (the profile of benzodiazepines and kava) tends to produce more genuinely restorative sleep.
Kava's profile fits the anxiolysis-with-mild-sedation pattern. The kavalactones produce GABA-A-mediated reduction in limbic arousal at clinical doses, with sedative effects emerging only at the higher end of the dose range or in combination with other CNS depressants. The Sarris KADSS trial (discussed in the Anxiety Relief deep-dive) explicitly identified sleep improvement as a secondary outcome, with subjective sleep quality improving alongside HAM-A score reduction.
The Lehrl 2004 WS 1490 Trial
The most cited sleep-specific kava trial is Lehrl 2004, published in the Journal of Affective Disorders. The study enrolled 61 adults with sleep disturbances associated with non-psychotic anxiety disorder, randomized them double-blind to either WS 1490 standardized kava extract (200 mg kavalactones per day in three divided doses) or placebo for 4 weeks, and measured sleep outcomes via the Sleep Questionnaire SF-A (a German validated sleep questionnaire) plus the HAM-A anxiety scale.
Results:
- Sleep quality (SF-A "quality of sleep" subscale) — significantly improved in the kava group versus placebo (p < 0.01)
- Recovery from sleep (SF-A "feeling rested" subscale) — significantly improved in the kava group
- Sleep latency — reduced in the kava group
- HAM-A score — significantly reduced in the kava group, confirming the parallel anxiolytic effect
- Subjective well-being — the well-being index (Bf-S) significantly improved in the kava group
- Safety — no significant changes in laboratory values, vital signs, or adverse event rate versus placebo over the 4-week trial
The Lehrl finding is consistent with the broader trial literature suggesting kava's sleep effect is mediated through anxiolysis rather than primary sedation — the patients who improved most on sleep also improved most on the anxiety measure, and the improvement in subjective well-being is incompatible with a heavy-sedation mechanism that would produce next-day fatigue.
The 4-week duration is a limitation; longer-term sleep efficacy and safety data are more limited. The choice of WS 1490 acetonic extract (rather than aqueous noble-cultivar root extract) is another consideration that became prominent in the wake of the 2002 European hepatotoxicity controversy, but in this specific trial liver function tests showed no adverse signal.
The Wheatley 2001 Kava vs Valerian Trial
The Wheatley 2001 study published in Phytotherapy Research is one of the few head-to-head trials comparing two botanical sleep aids. The study enrolled adults with stress-induced insomnia, treated them sequentially with 6 weeks of kava (120 mg kavalactones daily), a 2-week washout, and 6 weeks of valerian (600 mg standardized root extract daily). Both treatments produced significant improvement on the Sleep Questionnaire SF-B versus baseline:
- Kava sleep improvement — 13.8 point reduction on the stress subscale (p < 0.001 vs baseline)
- Valerian sleep improvement — 12.5 point reduction on the stress subscale (p < 0.001 vs baseline)
- Both treatments reduced stress-related symptoms measured by the Bf-S well-being scale
- Adverse events — both treatments well-tolerated; the most common complaint with kava was dizziness, with valerian was vivid dreams
The clinical implication is that for stress-related insomnia, both kava and valerian appear roughly equivalent in efficacy, with each having distinctive subjective qualities. The choice between them is therefore made on the basis of:
- Anxiety-predominant vs sleep-predominant complaint — kava's anxiolytic effect is generally stronger than valerian's
- Tolerance to side effects — some patients dislike valerian's characteristic earthy taste and vivid-dream effect; others dislike kava's numbing tongue effect
- Hepatotoxicity concern — valerian has a cleaner long-term hepatic safety profile in absolute terms; kava with noble-cultivar aqueous extract is also acceptably safe but requires more careful product selection
- Combination — the two can be combined at moderate doses for synergistic effect, though formal trials of the combination are limited
For broader context on natural sleep aids see our Valerian page, Passionflower page, and Lavender page.
Sleep Architecture Preservation (REM and NREM3)
One of the most important pharmacological distinctions between kava and conventional sleep medications concerns sleep architecture — the specific pattern of REM (rapid eye movement) and NREM (non-REM, divided into stages N1, N2, N3) sleep cycles through the night. Polysomnography is the technique used to map this architecture in laboratory studies.
Healthy human sleep alternates approximately every 90 minutes between NREM and REM phases. Each phase has distinctive electrical signatures, distinctive functional roles, and distinctive vulnerabilities to drug interference:
- NREM stage 3 (N3, also "slow-wave sleep") — characterized by high-amplitude delta waves on EEG. This is the physiologically restorative phase: growth hormone is released, glymphatic clearance of brain metabolites is active, and immune function is consolidated. Selective deprivation of N3 produces the subjective experience of "unrefreshing sleep" even when total sleep time is preserved.
- REM sleep — characterized by rapid eye movements, near-paralytic muscle atonia (except eye muscles), low-amplitude high-frequency EEG, and active dreaming. REM is essential for memory consolidation, particularly procedural and emotional memory. Selective deprivation of REM produces the experience of memory fragmentation and emotional dysregulation.
Most conventional sleep medications suppress one or both of these critical phases:
- Benzodiazepines — significantly suppress N3 (slow-wave sleep) and modestly suppress REM. The patient sleeps longer in stage N2 (light sleep), which the brain experiences as less restorative.
- Z-drugs (zolpidem, zaleplon) — similar pattern to benzodiazepines but typically less severe N3 suppression; eszopiclone is the most architecture-friendly of the z-drugs
- Antihistamines (diphenhydramine, doxylamine) — suppress REM sleep substantially; produce the characteristic "drugged sleep with vivid dreams during withdrawal" pattern
- Alcohol — suppresses REM in the first half of the night, then produces rebound REM in the second half (a major contributor to alcohol-related insomnia)
- Trazodone — less architecture disruption than benzodiazepines, often a preferred conventional choice for chronic insomnia
- Mirtazapine — relatively architecture-preserving
Kava polysomnography studies (limited but consistent) suggest the kavalactones do not significantly suppress either REM or N3 at clinical doses. The kava sleep effect appears to be primarily anxiolytic (reducing the limbic hyperarousal that prevents sleep onset) rather than direct sedative suppression of higher cortical states. This is one of the strongest theoretical advantages of kava over conventional hypnotics for patients with chronic insomnia who need sustained therapy.
The mechanistic explanation likely involves the specific GABA-A subunit selectivity of the kavalactones. Benzodiazepines act non-selectively across α1, α2, α3, and α5 containing GABA-A receptors, with the α1 subtype mediating both sedation and the slow-wave sleep suppression effect. The kavalactones appear to act preferentially at non-α1 subtypes, producing anxiolysis (α2/α3 mediated) without the sleep-architecture disruption that comes from heavy α1 stimulation.
Kava versus Benzodiazepines for Sleep
Benzodiazepines (temazepam, lorazepam, clonazepam used at bedtime, alprazolam less commonly) are still widely prescribed for insomnia despite well-established harms with chronic use. Kava's profile for sleep parallels its profile for anxiety, with several specific advantages and one disadvantage in the sleep-specific use case.
Where Kava Wins for Sleep
- Preserved sleep architecture — as discussed above, kava does not significantly suppress REM or slow-wave sleep, while benzodiazepines do
- No next-day cognitive impairment — the morning-after grogginess characteristic of benzodiazepines (particularly longer-acting agents like clonazepam) is generally absent with kava at sleep-appropriate doses
- No memory impairment — the bedtime amnesia that benzodiazepines produce (forgetting events between taking the medication and falling asleep, occasional middle-night amnesia for sleepwalking or eating episodes) does not occur with kava
- No physical dependence or withdrawal — the rebound insomnia that complicates benzodiazepine discontinuation is much milder or absent with kava
- No respiratory depression risk — particularly relevant for patients with sleep apnea or COPD who should not use benzodiazepines
- Less fall risk in older adults — benzodiazepines are a leading cause of falls and hip fractures in older patients
Where Benzodiazepines Win for Sleep
- Reliability of effect — a 1 mg lorazepam at bedtime will almost certainly produce sleep onset within 30 minutes in essentially every patient. Kava response varies meaningfully with product, individual pharmacogenomics, and current arousal level.
- Acute severe insomnia — benzodiazepines are appropriate for short-term use in acute crisis insomnia (post-bereavement, post-major-life-event, hospitalization). Kava is better suited to chronic mild-to-moderate sleep disturbance.
- Cleaner hepatic safety profile — in absolute terms benzodiazepines have a cleaner hepatic safety record, though kava with noble-cultivar aqueous root extract has an acceptable safety profile
The practical synthesis is that for the typical patient with chronic stress-related insomnia not responsive to sleep hygiene measures, kava is a reasonable trial before initiating benzodiazepine therapy. For acute severe insomnia or patients in whom rapid reliable effect is needed, benzodiazepines retain their role.
Kava versus Z-Drugs (Zolpidem, Eszopiclone)
The "z-drugs" (zolpidem, zaleplon, eszopiclone, zopiclone) are non-benzodiazepine GABA-A modulators that selectively target the α1 subunit, producing more selective sedation with somewhat less of the anxiolytic effect of classic benzodiazepines. They have largely replaced benzodiazepines as first-line prescribed hypnotics in much of the developed world.
Important distinctions versus kava:
- Z-drug parasomnias — zolpidem is well-documented to produce sleepwalking, sleep-driving, sleep-eating, and middle-night amnestic episodes in a meaningful fraction of users. These complications are essentially absent with kava.
- Z-drug tolerance — though marketed as less tolerance-prone than benzodiazepines, the z-drugs do produce dose-escalation tolerance with chronic use. Kava's tolerance profile is less well-studied but appears modest based on traditional use evidence.
- Z-drug rebound insomnia — discontinuation of chronic z-drug use commonly produces 1–2 weeks of rebound insomnia. Kava discontinuation does not typically produce rebound.
- Z-drug FDA boxed warning — in 2019 the FDA added a boxed warning to zolpidem, zaleplon, and eszopiclone regarding serious injuries and deaths from complex sleep behaviors. Kava carries no such warning.
- Z-drug cognitive effects in older adults — zolpidem in particular is associated with worsened cognitive performance in older adults; the American Geriatrics Society Beers Criteria recommend against its use in this population
For patients who have had a poor experience with z-drugs (whether through parasomnias, tolerance, or persistent next-day grogginess), kava represents a reasonable alternative with a meaningfully different mechanism and side-effect profile.
Kava versus Antihistamines (Diphenhydramine, Doxylamine)
The over-the-counter "PM" formulations (Tylenol PM, Advil PM, ZzzQuil) rely on first-generation antihistamines — diphenhydramine or doxylamine — for their sleep effect. These are extremely widely used, easily available, and generally considered "safe" by the lay public despite a problematic profile for chronic use.
Antihistamine sleep aids have important limitations versus kava:
- Anticholinergic burden — diphenhydramine is a substantial muscarinic antagonist; chronic use is associated in observational studies with increased dementia risk in older adults (Gray et al. JAMA Internal Medicine 2015). Kava has no anticholinergic activity.
- Tolerance within 3–4 days — the sleep-promoting effect of diphenhydramine wanes within 3–4 nights of continued use, leaving residual side effects without continued benefit. Kava does not show this rapid tolerance pattern.
- REM suppression — antihistamines significantly suppress REM sleep, producing unrefreshing sleep and rebound REM with vivid dreams upon discontinuation. Kava preserves REM.
- Next-day grogginess — the 8–10 hour half-life of diphenhydramine produces meaningful next-morning impairment, including impaired driving performance. Kava's 4–6 hour subjective duration produces less morning carryover.
- Constipation, urinary retention, dry mouth — anticholinergic side effects that bother many users. Kava does not produce these.
For patients currently using OTC antihistamines for chronic sleep complaints, kava represents a clear upgrade in side-effect profile and chronic safety.
Kava versus Melatonin, Valerian, and Other Natural Sleep Aids
Within the natural-medicine sleep aid category, kava competes with melatonin, valerian, passionflower, and several others. Each has a distinctive mechanism and use case.
Melatonin
- Acts on MT1 and MT2 receptors to signal the onset of biological night; physiologically a circadian timing signal rather than a sedative
- Best for circadian-misalignment insomnia (jet lag, shift work, delayed sleep phase syndrome)
- Less effective for primary anxiety-related insomnia — the proximate problem in that case is limbic hyperarousal, not circadian timing
- Generally safe; minimal interactions; works well in combination with kava (different mechanism, different time-course)
Valerian
- Acts through GABA reuptake inhibition (valerenic acid) plus weak GABA-A modulation
- Effect emerges over 2–4 weeks of consistent use; less reliable for acute single-dose use than kava
- Distinctive earthy smell and taste limits patient adherence
- Cleaner long-term hepatic safety than kava (in absolute terms; noble-cultivar aqueous kava is also acceptably safe)
- Wheatley 2001 showed roughly equivalent efficacy with kava for stress-related insomnia (discussed above)
Passionflower
- Also GABA-A modulator but at different binding sites than kava or benzodiazepines
- Generally milder effect; useful for mild anxiety-related sleep disturbance
- Often combined with valerian, lemon balm, or kava in proprietary sleep formulas
Lavender (Silexan)
- Standardized oral lavender oil preparation; reduces anxiety in trials comparable to lorazepam
- Less direct sleep evidence than kava but shares the anxiolytic mechanism
- Generally well-tolerated; minimal interactions
Ashwagandha
- Adaptogen with HPA-axis modulating effect
- Longer time course; works through stress hormone reduction rather than direct GABA modulation
- Sleep improvement documented in trials but slower onset than kava
For the patient with primary anxiety-related insomnia who needs both rapid effect and chronic-use tolerance, the most rational starting protocol is often a combination: melatonin 0.5–1 mg at bedtime for circadian signaling plus kava 120 mg kavalactones at bedtime for anxiolysis, with valerian or ashwagandha added for chronic maintenance if needed. For other sleep contexts the order and selection differ.
Menopausal and Perimenopausal Insomnia
Insomnia is one of the most distressing symptoms of perimenopause and early menopause, with up to 60% of perimenopausal women reporting clinically significant sleep disturbance. The biology is multi-factorial: declining progesterone (which has GABA-A modulating activity through its allopregnanolone metabolite) reduces endogenous GABA tone, hot flashes produce direct sleep disruption, mood disturbance contributes to ruminative cognition, and circadian shifts associated with hormonal change disturb sleep timing.
Limited but suggestive evidence supports kava for menopausal anxiety and associated sleep disturbance. The mechanism is appropriate: kava restores GABA-A tone that has dropped with declining progesterone, addresses anxiety component of the menopausal symptom complex, and does so without the cardiovascular concerns of hormone replacement therapy or the SSRI side effects (sexual dysfunction, GI upset, weight gain) that affect many menopausal women on conventional therapy.
The trial literature is small. A 2003 trial by Cagnacci et al. in 68 perimenopausal women with anxiety randomized to calcium plus kava or calcium alone found greater improvement in anxiety and sleep scores in the kava arm. A 2013 review in Menopause identified kava as one of the few botanical options with controlled trial evidence for menopausal anxiety, though noting the small total trial population.
The hepatotoxicity caution is particularly relevant in perimenopausal women, who may have higher baseline transaminase elevations (NAFLD prevalence rises in this age range) and who often use kava in combination with other supplements including black cohosh (also with documented hepatotoxicity concerns). Standard practice for any perimenopausal woman using kava should include baseline and follow-up liver function testing.
Practical Protocol for Sleep Use
Product Selection
- Noble cultivar aqueous root extract (instant kava, freeze-dried aqueous extract, or traditional cold-water preparation)
- Standardized to a known kavalactone content (typically 30–70 mg kavalactones per serving)
- Avoid acetonic, ethanolic, or supercritical CO2 extracts unless flavokavain B and pipermethystine content is documented as low
- Root-only labeling, not aerial parts or whole plant
Dosing for Sleep
- Initial trial: 60–120 mg kavalactones taken 45–60 minutes before bedtime
- Titrate upward to 180–240 mg kavalactones at bedtime if 60–120 mg is insufficient
- For mid-night awakening: a second 60 mg dose at the awakening (only if it occurs in the first half of the night, to avoid morning grogginess)
- Combine with melatonin 0.5–1 mg at bedtime for compounded effect if circadian misalignment is also present
What to Expect
- Subjective relaxation within 20–45 minutes of ingestion
- Sleep onset within 30–60 minutes typically
- Sleep quality often improves more than sleep onset time per se — patients commonly report waking less often, returning to sleep faster after middle-night awakenings, and feeling more rested
- Effect tends to build over the first 1–2 weeks of consistent use; do not abandon after a single trial
- Numb mouth/tongue effect at higher traditional doses is normal and harmless
What to Avoid
- Alcohol the same evening — additive CNS depression and additive hepatic stress
- Acetaminophen the same evening, particularly > 1 g
- Benzodiazepines or z-drugs the same evening — additive sedation
- Driving until familiar with personal response to kava
Cycling
Conservative practice for chronic nightly use: 4 weeks of nightly use, 1 week off, repeated. Many patients find that intermittent use (3–4 nights per week, on the worst-sleep nights) is sufficient and minimizes any concern about chronic exposure.
For broader sleep management see our Sleep Hygiene page and Insomnia page.
Key Research Papers
- Lehrl S (2004). Clinical efficacy of kava extract WS 1490 in sleep disturbances associated with anxiety disorders. Journal of Affective Disorders. — PubMed
- Wheatley D (2001). Kava and valerian in the treatment of stress-induced insomnia. Phytotherapy Research. — PubMed
- Cagnacci A et al. (2003). Kava-Kava administration reduces anxiety in perimenopausal women. Maturitas. — PubMed
- Ernst E (2007). Herbal remedies for anxiety: a systematic review of controlled clinical trials. Phytomedicine. — PubMed
- Sarris J et al. (2011). Plant-based medicines for anxiety disorders, Part 2: a review of clinical studies with supporting preclinical evidence. CNS Drugs. — PubMed
- Geier FP, Konstantinowicz T (2004). Kava treatment in patients with anxiety. Phytotherapy Research. — PubMed
- Gray SL et al. (2015). Cumulative use of strong anticholinergics and incident dementia. JAMA Internal Medicine. — PubMed (context for diphenhydramine comparison)
- Kava polysomnographic sleep architecture preservation studies — PubMed: Kava polysomnography
- Emser W, Bartylla K (1991). Effect of Kava Extract WS 1490 on the sleep pattern in healthy subjects (German polysomnography study). — PubMed
- Saletu B et al. (1989). EEG-brain mapping, psychometric and psychophysiological studies on central effects of kavain. Human Psychopharmacology. — PubMed
- Volz HP, Hehnke U, Hauke W (2002). Kava-Special-Extract WS 1490 in non-psychotic anxiety disorders. European Journal of Clinical Pharmacology. — PubMed
- Sarris J et al. (2009). Complementary medicine, exercise, meditation, diet, and lifestyle modification for anxiety disorders. Nutrition Journal. — PubMed
PubMed Topic Searches
- PubMed: Kava insomnia RCTs
- PubMed: Kava polysomnography
- PubMed: Kava menopausal sleep
- PubMed: Natural sleep aids
- PubMed: GABA-A α1 and sleep
Connections
- Kava Overview
- Kava Benefits Hub
- Kava for Anxiety
- Kava for Muscle Relaxation
- Kava for Mood
- Insomnia
- Insomnia (Symptom)
- Anxiety
- Sleep Hygiene
- Stress Management
- Valerian
- Passionflower
- Lavender
- Lemon Balm
- Ashwagandha