Kava for Anxiety Relief
Kava (Piper methysticum) is the only botanical anxiolytic with consistent positive evidence in modern randomized controlled trials, including the landmark 2013 Sarris KADSS (Kava Anxiety Depression Spectrum Study) showing significant reduction in generalized anxiety disorder symptoms versus placebo, and the Pittler & Ernst 2003 Cochrane meta-analysis pooling 11 RCTs that found a clinically meaningful effect size compared to placebo. The mechanism is positive allosteric modulation of GABA-A receptors by the kavalactone class — principally kavain, methysticin, and yangonin — at sites distinct from the benzodiazepine binding pocket, producing anxiolysis without the tolerance, withdrawal, or amnestic effects characteristic of BZDs. This deep-dive walks through the clinical trial evidence, the GABA-A pharmacology, the comparison to benzodiazepines and SSRIs, and the practical use of kava as a first-line botanical option for mild to moderate generalized anxiety.
Table of Contents
- The Sarris 2013 KADSS Trial
- The Pittler & Ernst 2003 Cochrane Meta-Analysis
- The Six Principal Kavalactones
- GABA-A Allosteric Modulation Mechanism
- Kava versus Benzodiazepines
- Kava versus SSRIs and Buspirone
- Trial History (Volz 1997 to Witte 2005)
- Dosing and Practical Use for Anxiety
- Social Anxiety and Performance Anxiety
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
The Sarris 2013 KADSS Trial
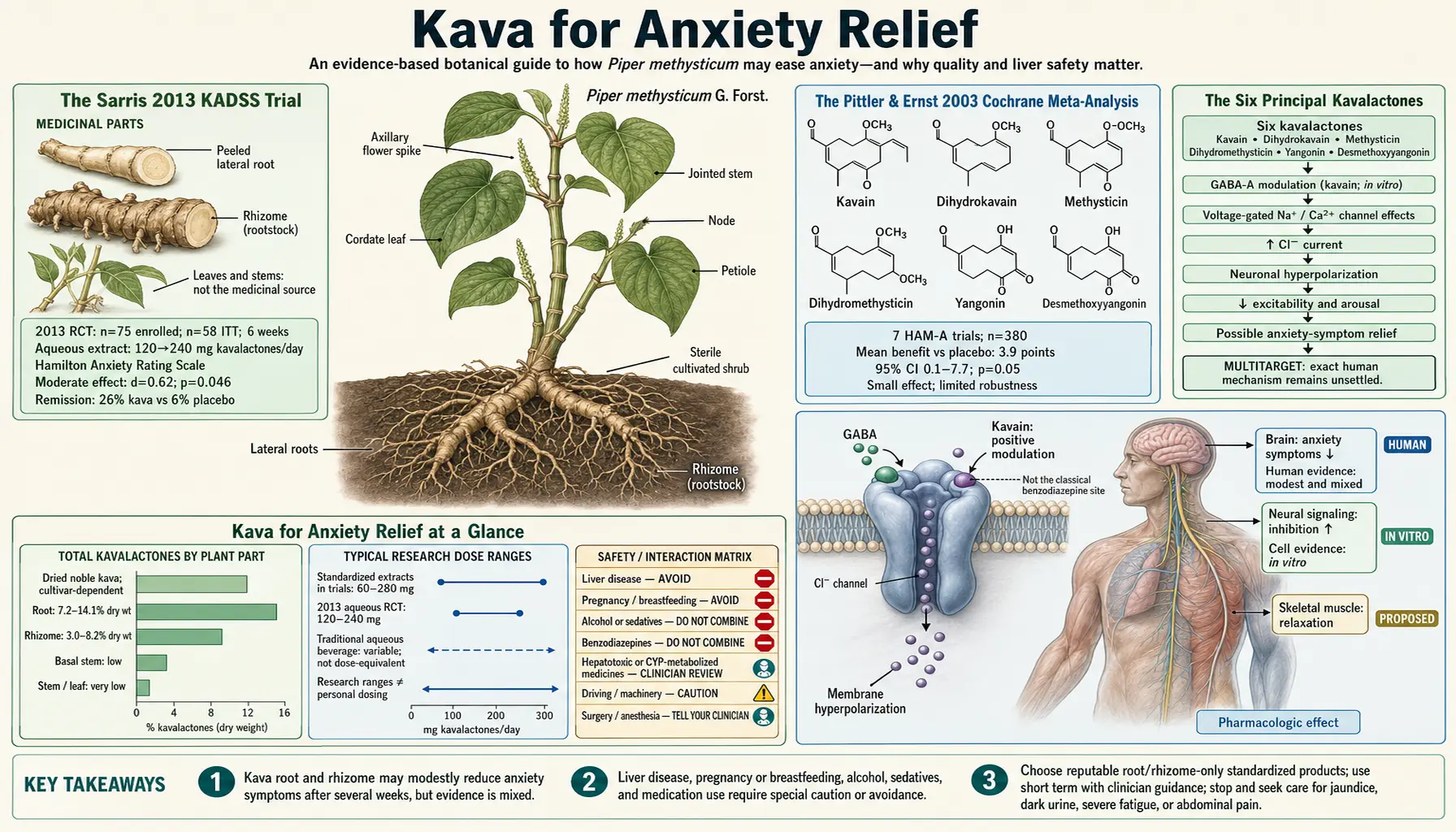
The single strongest piece of modern evidence that kava is genuinely anxiolytic in clinically diagnosed anxiety disorder is the Sarris et al. 2013 KADSS trial, published in the Journal of Clinical Psychopharmacology. The study enrolled 75 adults with DSM-IV diagnosed generalized anxiety disorder (Hamilton Anxiety Rating Scale ≥ 20 at baseline), randomized them double-blind to either an aqueous extract of noble Vanuatu kava cultivar (titrated to 120 mg kavalactones per day for the first three weeks, escalated to 240 mg/day for an additional three weeks if needed) or matched placebo, and measured HAM-A change at 6 weeks.
Results were unambiguous:
- HAM-A reduction — the kava group showed a 7.6 point reduction in HAM-A score versus 3.4 points in the placebo group, a statistically significant difference (p = 0.046)
- Remission rate — 26% of the kava group versus 6% of the placebo group achieved full remission (HAM-A ≤ 7) by week 6
- Comorbid depression — the Montgomery-Åsberg Depression Rating Scale (MADRS) also improved more in the kava group, an important subsidiary finding that motivated subsequent depression-focused research
- Liver function — serial liver function tests (ALT, AST, GGT, alkaline phosphatase, bilirubin) showed no significant change in the kava group versus placebo, supporting the safety of noble-cultivar aqueous root extracts
- Adverse events — the kava group reported slightly more headache and reduced libido but no serious adverse events
The KADSS trial was important because it used a noble Vanuatu cultivar aqueous extract — the traditional preparation type — rather than the acetonic or ethanolic extracts implicated in the 2002 European hepatotoxicity controversy. The clean liver function results at clinical doses are themselves a contribution to the kava safety literature, beyond the primary efficacy finding.
A 2020 follow-up trial by Sarris (the larger KGA trial, K-GAD) attempted to replicate the KADSS finding with a different extract and longer duration but found a smaller, statistically non-significant effect — consistent with the literature's general pattern that aqueous root extracts of noble cultivars produce more reliable anxiolysis than more processed commercial preparations. The KADSS protocol remains the methodological benchmark for kava anxiolysis research.
The Pittler & Ernst 2003 Cochrane Meta-Analysis
The Pittler and Ernst 2003 Cochrane systematic review pooled 11 randomized double-blind placebo-controlled trials of kava extract for anxiety, with a combined sample of 645 patients. The primary outcome was reduction in Hamilton Anxiety Rating Scale (HAM-A) total score versus placebo. Results showed a weighted mean difference of -3.9 HAM-A points favoring kava (95% CI -5.7 to -2.1, p < 0.0001), corresponding to a clinically meaningful effect size of approximately 0.4 standardized mean difference.
The Cochrane review noted several important caveats:
- Heterogeneity of extract type — the 11 included trials used different kava preparations (predominantly WS 1490 acetonic extract, but also LI 150 methanolic extract and others). Effect sizes varied with extract type.
- Generally short duration — most trials were 4 to 12 weeks. Longer-term efficacy and safety were not addressed.
- Generally mild-to-moderate baseline anxiety — trials enrolled patients with anxiety symptoms (mostly tension, mixed anxiety/depression, generalized anxiety) but typically not severe panic disorder or specific phobia
- Safety signal — the meta-analysis reviewed adverse event reporting and found no significant difference in adverse event rate between kava and placebo. However, the pooled trials predated much of the 2002 hepatotoxicity reporting and could not address that issue directly.
The 2003 Cochrane review concluded that kava was "an effective symptomatic treatment for anxiety" with a favorable risk-benefit profile in the trials reviewed, while noting the emerging hepatotoxicity concern warranted ongoing vigilance. The 2011 Cochrane update (Pittler & Ernst again) reached a similar conclusion with additional trials included.
The combination of the Pittler Cochrane review (high-quality meta-analytic evidence for anxiolysis as a class effect) plus the Sarris KADSS trial (a methodologically rigorous single trial confirming efficacy in DSM-IV diagnosed GAD with a safer extract type) constitutes the strongest evidence base for any botanical anxiolytic.
The Six Principal Kavalactones
Kava's bioactivity resides in the kavalactone class — styryl-2-pyranones (also called α-pyrones) concentrated in the root and rhizome of Piper methysticum. Six kavalactones together account for approximately 96% of the kavalactone content of a typical noble-cultivar root preparation:
- Kavain (also kawain) — the most extensively studied kavalactone; principal GABA-A allosteric modulator; voltage-gated sodium channel blocker; weak dopamine reuptake inhibitor. Approximately 15–25% of total kavalactones in a typical noble cultivar.
- Methysticin — second most abundant; GABA-A modulator; neuromuscular effects; weak dopamine reuptake inhibitor. Approximately 10–20% of total kavalactones.
- Yangonin — pigmented kavalactone with characteristic yellow color; principal MAO-B inhibitor among the kavalactone class; relevant to mood effects. Approximately 10–20% of total kavalactones.
- Desmethoxyyangonin — structural variant of yangonin with similar MAO-B inhibitory activity; weaker GABA-A activity than kavain. Approximately 5–15% of total kavalactones.
- Dihydromethysticin — saturated version of methysticin; longer-acting at GABA-A; implicated in the longer-duration sedative effect of some preparations. Approximately 5–15% of total kavalactones.
- Dihydrokavain — saturated kavain analog; significant skeletal muscle relaxant activity; less GABA-A modulation than kavain. Approximately 5–15% of total kavalactones.
The relative proportions of these six kavalactones is highly cultivar-specific and is captured in the "chemotype" notation: a six-digit code (e.g. 462531) indicating the rank order of abundance from highest to lowest. A chemotype 462531 cultivar means desmethoxyyangonin (#4) is most abundant, dihydromethysticin (#6) is second, etc. Traditional Pacific kava cultivars have specific chemotypes that have been selected over millennia for their balanced anxiolytic-sedative-muscle-relaxant profile. Cultivars with high flavokavain B and pipermethystine content (the tudei cultivars) have historically been used only in restricted ritual contexts because of their less-tolerated psychoactive and toxicity profile.
The chemotype variability also explains why kava research is so methodologically difficult: a clinical trial of a single standardized extract (e.g. WS 1490 acetonic extract titrated to 70% kavalactones) does not necessarily generalize to a different aqueous root preparation of a different cultivar.
GABA-A Allosteric Modulation Mechanism
The principal anxiolytic mechanism of the kavalactones is positive allosteric modulation of GABA-A receptors — the same receptor class targeted by benzodiazepines, barbiturates, ethanol, neurosteroids, propofol, and zolpidem — but at distinct binding sites with distinct functional consequences.
The GABA-A receptor is a pentameric ligand-gated chloride channel composed of various combinations of subunits (typically two α, two β, and one γ subunit). GABA binding at the α-β interface opens the channel and allows chloride influx, hyperpolarizing the postsynaptic neuron and reducing its excitability. Various allosteric modulators bind at distinct sites on the receptor to enhance (positive modulation) or reduce (negative modulation) GABA's effect:
- The benzodiazepine site at the α-γ interface (sensitive to flumazenil reversal)
- The barbiturate site on the β subunit
- The neurosteroid site on the membrane-facing α subunit
- The ethanol site (multiple proposed locations on α and δ subunits)
The kavalactones do not displace flumazenil from the benzodiazepine site in radioligand binding studies (Boonen et al. 1998, others), indicating their site of action is distinct from the BZD site. The exact molecular pocket has not been definitively identified, but pharmacological evidence suggests interaction at the β3 subunit or a novel allosteric site. Functional consequences differ from benzodiazepines in three important ways:
- No cross-tolerance with benzodiazepines — patients on chronic benzodiazepines do not show reduced response to kava, suggesting non-overlapping mechanism
- No flumazenil reversal — the BZD antagonist flumazenil does not reverse kava-induced anxiolysis, confirming separate sites
- Less amnestic effect — kava at clinical doses does not produce the anterograde amnesia characteristic of benzodiazepines, presumably because it does not act at the hippocampally-enriched α5-containing GABA-A subtype that mediates BZD amnestic effects
The functional implication is that kava provides GABA-A-mediated anxiolysis without the most problematic side effects of benzodiazepines: tolerance, withdrawal syndrome, amnesia, and abuse liability. This pharmacological profile makes kava a useful option in clinical situations where a patient needs an anxiolytic but cannot tolerate or should not be exposed to benzodiazepines — including older patients, patients with substance use history, and patients requiring sustained daily use beyond a few weeks.
For broader context on GABA pharmacology and other natural GABAergic modulators, see the Valerian page and the Passionflower page — both work through partially overlapping but distinct GABA mechanisms.
Kava versus Benzodiazepines
The clinical comparison between kava and benzodiazepines is one of the most important practical questions in botanical anxiolytic medicine. The two classes target overlapping receptor populations but produce meaningfully different clinical profiles.
Where Kava Wins
- No physical dependence or withdrawal — kava does not produce a benzodiazepine-style withdrawal syndrome on discontinuation. There is no documented requirement for tapering. This is the single most important practical advantage in patients who would otherwise need chronic anxiolytic therapy.
- No anterograde amnesia — clinical doses of kava do not impair encoding of new memories, in contrast to benzodiazepines
- Less cognitive blunting — kava at clinical doses does not impair reaction time, working memory, or driving simulator performance (see the Mood and Cognitive Effects deep-dive)
- No respiratory depression — kava does not produce the respiratory depression risk that makes benzodiazepines dangerous in overdose or in combination with opioids
- No paradoxical disinhibition — benzodiazepines occasionally produce paradoxical agitation, aggression, or disinhibition, particularly in older adults and those with personality disorders. This is not a documented effect of kava.
Where Benzodiazepines Win
- Onset speed — sublingual or IV benzodiazepines act in minutes for acute panic or severe agitation. Oral kava onset is 20–45 minutes.
- Potency — benzodiazepines produce stronger anxiolysis in severe acute anxiety, panic, or pre-procedural sedation. Kava's clinical effect size in the trials is moderate, not large.
- Reliability across patients — benzodiazepine response is highly predictable. Kava response varies meaningfully with cultivar, extract type, and individual pharmacogenomics.
- Hepatic safety record — though kava-related hepatotoxicity is overwhelmingly associated with poor-quality extracts of aerial plant material (see the Hepatotoxicity Controversy section on the hub page), benzodiazepines have a cleaner hepatic safety profile in absolute terms.
The practical synthesis is that benzodiazepines remain the right choice for acute severe anxiety or pre-procedural sedation, while kava is a reasonable first-line choice for mild-to-moderate generalized anxiety where chronic use is anticipated. The decision should also account for patient preference, history of substance use disorder, age (kava is generally safer in geriatric populations), and concurrent medications.
Kava versus SSRIs and Buspirone
SSRIs (sertraline, escitalopram, paroxetine) are first-line pharmacological therapy for generalized anxiety disorder in most modern psychiatric guidelines. Buspirone (a 5-HT1A partial agonist) is a second-line oral agent specifically approved for GAD. Kava's place in this hierarchy is not yet formally established but its profile suggests specific clinical niches.
Onset and Time Course
- SSRIs — 4–8 weeks to clinical effect; common early-treatment activation, GI upset, sexual dysfunction; discontinuation syndrome possible especially with paroxetine
- Buspirone — 2–4 weeks to clinical effect; well-tolerated; no significant withdrawal; modest efficacy
- Kava — effect emerges within days to weeks; the Sarris KADSS trial showed measurable separation from placebo by week 2; no withdrawal syndrome; modest efficacy similar to buspirone
Clinical Niche for Kava
- Patients who have failed or cannot tolerate SSRIs (typically due to sexual dysfunction, GI upset, or activation/agitation)
- Patients who refuse SSRIs based on preference or stigma concerns
- Patients requiring acute symptomatic relief while waiting for SSRI onset
- Patients with anxiety that is primarily situational or stress-related rather than chronic
- Older patients in whom benzodiazepines are contraindicated and SSRIs may cause hyponatremia or fall risk
Combination Considerations
Combining kava with SSRIs is not absolutely contraindicated but warrants caution because the MAO-B inhibitory activity of yangonin and desmethoxyyangonin could theoretically interact with serotonergic medications. In practice, the in vivo MAO-B inhibition appears clinically modest and serotonin syndrome from this combination is not well-documented in case reports, but conservative clinicians avoid the combination. Combining kava with benzodiazepines should also be avoided because of additive CNS depression, even though the receptor sites are distinct.
For broader context on natural anxiety remedies and stress management, see our Natural Anxiety Relief page and Stress Management page.
Trial History (Volz 1997 to Witte 2005)
The clinical trial literature on kava for anxiety spans nearly three decades and includes more than 20 randomized controlled trials. The principal milestones:
- Lehmann 1996 — one of the earliest controlled trials, 58 patients with anxiety of non-mental origin, demonstrated symptomatic improvement with WS 1490 versus placebo
- Volz & Kieser 1997 — the most cited European trial of kava for anxiety. 101 patients with various anxiety disorders, randomized to WS 1490 (100 mg three times daily, providing 210 mg kavalactones/day) or placebo for 25 weeks. The HAM-A score reduction was significantly greater in the kava group, and the separation appeared as early as week 8. This trial substantially established the German market for kava extracts.
- Watkins et al. 2001 — small (12 patient) mechanistic study of kava's effect on heart rate variability in generalized anxiety disorder, finding improved vagal tone consistent with autonomic anxiolysis
- Connor & Davidson 2002 — US trial in 35 patients with generalized anxiety disorder, marginal positive result; published just as the European hepatotoxicity controversy was emerging and contributed to subsequent caution
- Pittler & Ernst 2003 Cochrane review — meta-analytic synthesis of available trials, strongly positive effect estimate
- Witte et al. 2005 — meta-analysis specifically of WS 1490 trials (six studies), pooled effect size approximately -9.7 HAM-A points favoring kava
- Sarris et al. 2009 (KADSS pilot) — smaller pilot of aqueous extract in 60 patients with anxiety, positive signal
- Sarris et al. 2013 (KADSS full trial) — the trial discussed in detail above, the modern benchmark for kava anxiolysis evidence
- Sarris et al. 2020 (K-GAD) — larger 171 patient trial in DSM-5 diagnosed GAD, failed to show statistically significant separation from placebo. The trial used a different cultivar mix and an ethanolic extract; the discrepant result has been variously attributed to extract type, dosing, and patient population.
The overall pattern across nearly three decades of trials is consistent: aqueous extracts of noble cultivars at adequate kavalactone dose produce moderate but reliable anxiolysis in generalized anxiety disorder, with an effect size comparable to buspirone and a safety profile that is favorable in noble-cultivar root extracts but problematic in acetonic-or-ethanolic extracts of aerial plant material.
Dosing and Practical Use for Anxiety
Effective anxiolytic dosing for kava is measured in milligrams of total kavalactones per day, not in grams of root or milliliters of preparation. Different products have different kavalactone concentrations, so reading the label for kavalactone content is essential.
Dose Ranges from the Trial Literature
- Minimum anxiolytic dose — approximately 60 mg kavalactones/day; below this, most trials fail to separate from placebo
- Standard anxiolytic dose — 120–240 mg kavalactones/day, typically divided into 2–3 doses; this is the range used in the Sarris KADSS trial
- WS 1490 standardized acetonic extract (German market, no longer sold in Europe but referenced in much of the trial literature) — 100 mg three times daily, providing ~210 mg kavalactones/day
- Traditional Pacific kava preparation — a single "shell" of traditional aqueous extract typically delivers 100–250 mg kavalactones; a social session might involve 4–8 shells over 2–3 hours
Onset and Duration
- Onset — 20–45 minutes after oral dosing; faster on empty stomach
- Peak effect — 1–2 hours after dosing
- Duration — 4–6 hours of subjective effect; longer-acting dihydromethysticin component may extend perceived effect to 8 hours
- Steady-state effect — full anxiolytic effect from regular daily dosing typically establishes by 2–4 weeks of consistent intake, similar to the time course of buspirone
Product Selection
- Choose products labeled "noble cultivar" with cultivar names from the Vanuatu noble list (Borogu, Melomelo, Palarasul, others)
- Prefer aqueous extract or instant kava ("water soluble") preparations over acetonic, ethanolic, or supercritical CO2 extracts
- Verify "root only" labeling, not "aerial parts" or "whole plant"
- Reasonable consumer certifications: American Kava Association (AKA) noble certification
- If using whole-root kava for traditional preparation: 1–3 tablespoons of ground noble root in cold water, kneaded in a strainer bag for 5–10 minutes, strained, consumed
Cycling and Duration of Use
Traditional Pacific use is social and ceremonial, not daily medication. For modern anxiolytic use, a reasonable conservative approach is to cycle the herb — for example, 4 weeks of daily use followed by a 1-week break, repeated as needed. Baseline liver function testing (ALT, AST, GGT, alkaline phosphatase, total bilirubin) before starting and after the first month, with periodic repeats every 3–6 months, is prudent for anyone using kava daily.
Social Anxiety and Performance Anxiety
While most randomized controlled trial evidence for kava concerns generalized anxiety disorder, traditional Pacific use is overwhelmingly in social and ceremonial contexts — a context that maps onto modern Western diagnostic categories of social anxiety disorder and situational performance anxiety. The subjective qualities reported by long-time kava users are precisely those one would want for these conditions: sociable but not euphoric, relaxed but mentally clear, fluent but not impulsive.
Pilot evidence for kava in social anxiety disorder is suggestive but limited. A small open-label study in social phobia patients found measurable improvement on Liebowitz Social Anxiety Scale scores. No large randomized controlled trial has specifically targeted social anxiety disorder as the primary diagnosis.
The use case for kava in performance anxiety (public speaking, stage performance, test-taking, athletic performance, situations where benzodiazepines are problematic because of their cognitive blunting) is supported by mechanistic arguments and by traditional use evidence but not by formal RCT data. The practical considerations:
- Onset of 20–45 minutes means kava should be taken before the anxiety-provoking event, not at the moment of acute symptoms
- Effect on cognitive performance is neutral at clinical doses, in contrast to beta-blockers (which can cause fatigue) and benzodiazepines (which impair memory and reaction time) — an advantage for situations requiring cognitive performance
- The 4–6 hour duration matches a typical examination, presentation, or stage performance window
- Repeat dosing for sustained performance over days (multi-day examinations, tournament play) is reasonable
For broader context on anxiety conditions, see our Anxiety page.
Cautions and Drug Interactions
- Hepatotoxicity from poor-quality extracts — the most important caution, covered comprehensively in the dedicated section on the Benefits hub page. Use only noble-cultivar aqueous root extracts. Obtain baseline liver function testing and repeat periodically.
- Concurrent alcohol — substantially increases hepatic risk and additive CNS depression. Avoid the combination. The 2002 European case reports of severe hepatotoxicity frequently involved concurrent alcohol consumption.
- Concurrent acetaminophen — both compete for hepatic glutathione conjugation. Limit acetaminophen to less than 2 g/day in kava users, and avoid the combination entirely for daily chronic kava use.
- Concurrent benzodiazepines, opioids, or alcohol — additive CNS depression and respiratory effects. Do not combine.
- Concurrent SSRIs or MAOIs — theoretical risk of serotonin syndrome from the MAO-B inhibitory activity of yangonin. Avoid concurrent MAOIs absolutely; use caution with SSRIs.
- CYP450 interactions — kavalactones inhibit CYP1A2, CYP2C9, CYP2C19, CYP2D6, and CYP3A4 in vitro. Clinical implications include possible elevated levels of warfarin, phenytoin, statins, and many other substrates. Use with caution alongside any narrow-therapeutic-index medication.
- Driving and operating machinery — though kava at clinical doses does not measurably impair driving simulator performance, individual response varies. Test response in a safe setting before driving on kava.
- Pregnancy and breastfeeding — insufficient data; avoid as a conservative default
- Parkinson's disease — case reports of worsened parkinsonian symptoms with chronic high-dose kava use, possibly via dopaminergic interaction. Avoid in established Parkinson's.
- Pre-existing liver disease — absolute contraindication in active hepatitis, cirrhosis, or NAFLD with elevated transaminases
- Pre-surgical period — discontinue at least 2 weeks before elective surgery because of additive sedation with general anesthesia
- Dermopathy ("kava dermopathy") — chronic high-dose use (typical of daily Pacific consumers) can produce a reversible dry, scaly, yellowish skin rash. The mechanism may be interference with cholesterol metabolism. Resolves on discontinuation.
Key Research Papers
- Sarris J et al. (2013). Kava in the treatment of generalized anxiety disorder: a double-blind, randomized, placebo-controlled study (KADSS). Journal of Clinical Psychopharmacology. — PubMed
- Pittler MH, Ernst E (2003). Kava extract for treating anxiety. Cochrane Database of Systematic Reviews. — PubMed
- Volz HP, Kieser M (1997). Kava-kava extract WS 1490 versus placebo in anxiety disorders — a randomized placebo-controlled 25-week outpatient trial. Pharmacopsychiatry. — PubMed
- Lehmann E et al. (1996). Efficacy of a special kava extract in patients with states of anxiety. Phytomedicine. — PubMed
- Connor KM, Davidson JRT (2002). A placebo-controlled study of Kava kava in generalized anxiety disorder. International Clinical Psychopharmacology. — PubMed
- Witte S et al. (2005). Meta-analysis of the efficacy of the acetonic kava-kava extract WS 1490. Phytotherapy Research. — PubMed
- Sarris J et al. (2020). Kava in the treatment of generalized anxiety disorder: the K-GAD trial. Journal of Clinical Psychopharmacology. — PubMed
- Watkins LL et al. (2001). Effect of kava extract on vagal cardiac control in generalized anxiety disorder. Journal of Psychopharmacology. — PubMed
- Boonen G, Häberlein H (1998). Influence of genuine kavapyrone enantiomers on the GABA-A binding site. Planta Medica. — PubMed
- Singh YN, Singh NN (2002). Therapeutic potential of kava in the treatment of anxiety disorders. CNS Drugs. — PubMed
- Sarris J, Kavanagh DJ (2009). Kava and St. John's wort: current evidence for use in mood and anxiety disorders. Journal of Alternative and Complementary Medicine. — PubMed
- Smith K, Leiras C (2018). The effectiveness and safety of Kava Kava for treating anxiety symptoms: systematic review and analysis of randomized clinical trials. Complementary Therapies in Clinical Practice. — PubMed
PubMed Topic Searches
- PubMed: Kava GAD randomized trials
- PubMed: Kavalactone GABA-A modulation
- PubMed: Kava vs benzodiazepine
- PubMed: WS 1490 anxiety trials
- PubMed: Kava social anxiety
Connections
- Kava Overview
- Kava Benefits Hub
- Kava for Sleep
- Kava for Muscle Relaxation
- Kava for Mood
- Anxiety
- Depression
- Natural Anxiety Relief
- Stress Management
- Valerian (GABA Reuptake)
- Passionflower (GABA-A)
- Lavender
- Lemon Balm
- Ashwagandha (HPA Axis)
- All Herbs