Kava for Mood and Cognitive Effects
One of the most striking and counterintuitive findings in the modern kava literature is that the kavalactones, despite producing measurable anxiolysis and physical relaxation, do not impair cognitive performance at clinical doses — in direct contrast to alcohol, benzodiazepines, and most other GABAergic anxiolytics. Reaction time, working memory, attention, and driving simulator performance are all preserved on kava in head-to-head trials. The Sarris KADSS depression sub-analysis additionally documented improvement in comorbid depressive symptoms alongside the primary anxiety endpoint, suggesting a genuine mood-elevating effect distinct from the anxiolysis. The leading mechanistic hypotheses for the mood effect are reversible monoamine oxidase B inhibition by yangonin and desmethoxyyangonin (prolonging dopamine and phenethylamine in the synapse) and weak dopamine reuptake inhibition by kavain and methysticin (similar to but much milder than the mechanism of stimulants). This deep-dive walks through the depression sub-analysis evidence, the cognitive non-impairment studies, the MAO-B and dopamine reuptake hypotheses, and the practical implications for "the only sociable sedative."
Table of Contents
- Sarris KADSS Depression Sub-Analysis
- "The Only Sociable Sedative" — The Subjective Quality
- Cognitive Non-Impairment Trials
- Kava versus Alcohol on Cognitive Performance
- Kava versus Benzodiazepines on Cognitive Performance
- The MAO-B Inhibition Hypothesis
- Dopamine Reuptake Inhibition Hypothesis
- Mood Elevation Without Stimulant Character
- Kava in Major Depressive Disorder Pilot Evidence
- Cautions for the Mood Use Case
- Key Research Papers
- Connections
- Featured Videos
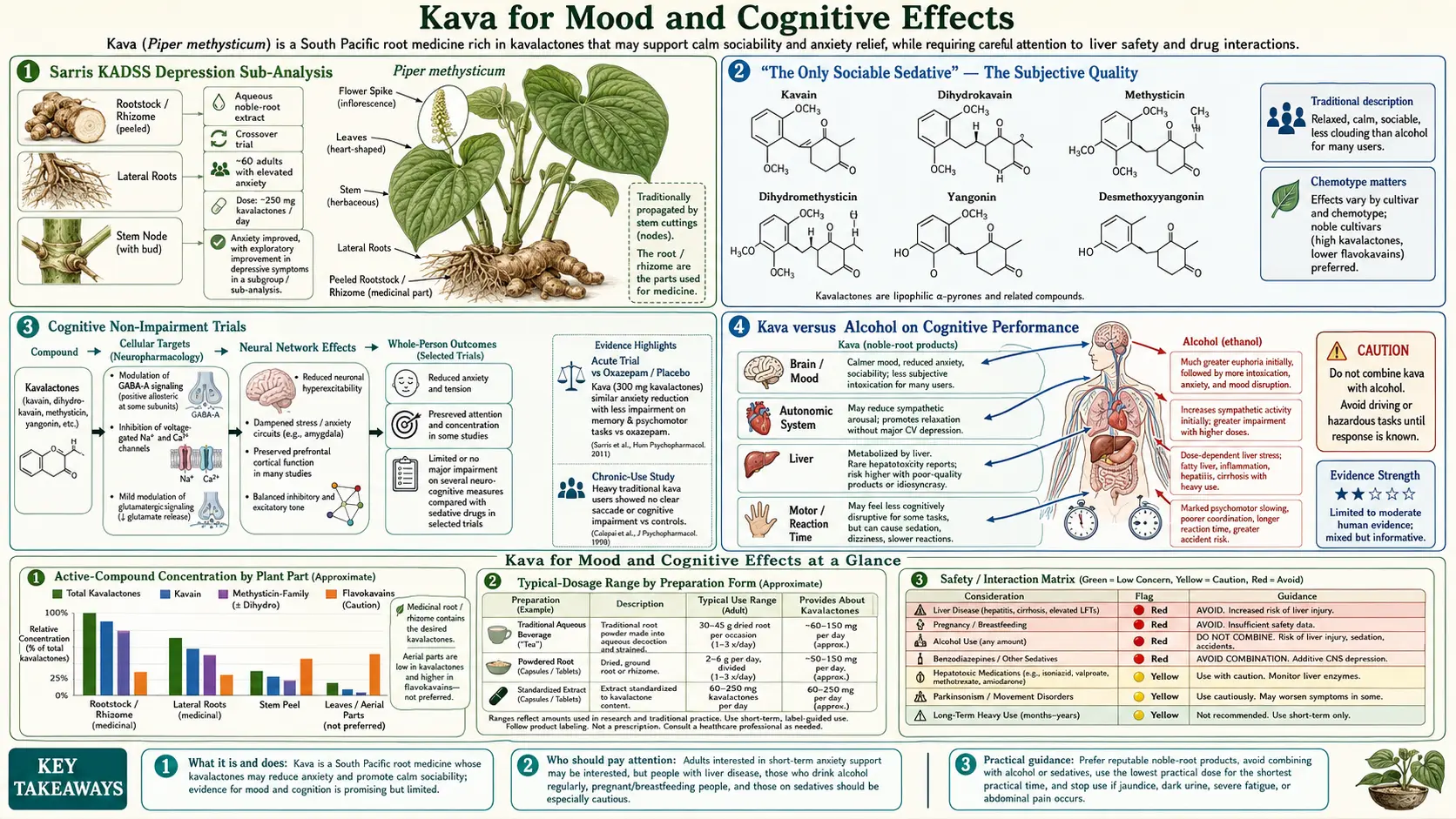
Sarris KADSS Depression Sub-Analysis
The 2013 Sarris KADSS (Kava Anxiety Depression Spectrum Study) trial, discussed extensively in the Anxiety Relief deep-dive, was designed with anxiety as the primary endpoint but explicitly included the Montgomery-Åsberg Depression Rating Scale (MADRS) as a secondary outcome because of suggestive earlier evidence that kava might also produce mood improvement.
The depression sub-analysis result was striking: 75 patients with DSM-IV generalized anxiety disorder, many of whom had comorbid depressive symptoms at baseline (mean baseline MADRS ~13, in the mild-to-moderate range). At 6 weeks:
- MADRS reduction — the kava group showed a 3.5 point reduction in MADRS score versus 1.2 points in the placebo group, a statistically significant difference
- Bf-S well-being scale — significant improvement in subjective well-being in the kava group versus placebo
- Effect appeared independent of anxiety improvement — the depression score reduction did not fully track the anxiety score reduction, suggesting some independent mood-elevating effect rather than simply secondary improvement from reduced anxiety
The Sarris depression sub-analysis was not a definitive demonstration of antidepressant efficacy — the study was not powered as a depression trial, the patients were not enrolled for primary depressive diagnosis, and the depression score change was modest. But it provided enough signal to motivate subsequent dedicated investigation of kava in major depressive disorder, and it confirmed the broader pattern observed across the kava literature: aqueous noble-cultivar kava extracts produce mood elevation that goes beyond simple anxiolysis.
The earlier 2009 Sarris KADSS pilot study had identified the same pattern with a smaller sample, providing the rationale for including the MADRS in the larger trial. A subsequent open-label trial by Sarris et al. specifically in adults with major depressive disorder found modest improvement in HAM-D scores over 4 weeks but was not placebo-controlled.
"The Only Sociable Sedative" — The Subjective Quality
Long-time observers of kava use across both traditional Pacific contexts and modern recreational/medicinal use commonly describe the kava experience with a phrase that captures something genuinely unusual in psychopharmacology: kava is the only "sociable sedative." Unlike alcohol, it does not disinhibit. Unlike benzodiazepines, it does not blunt. Unlike opioids, it does not produce euphoria. Unlike stimulants, it does not energize. What it produces is best described as relaxed sociability with mental clarity — a state in which conversation flows more easily, interpersonal warmth increases, social anxiety drops, but the participant remains fully present, alert, and able to make complex judgments.
This subjective quality is essentially incompatible with the conventional GABA-A pharmacology of sedatives. Most GABA-A modulators (alcohol, benzodiazepines, barbiturates) produce sedation precisely because they reduce cortical activity globally, including the cortical activity needed for cognitive performance and emotional regulation. Kava's ability to produce anxiolysis without this global cortical depression is one of the more interesting unsolved questions in psychopharmacology.
The leading hypotheses for why kava is sociable while other GABAergic agents are not:
- GABA-A subunit selectivity — kavalactones may act preferentially at α2/α3-containing GABA-A receptors (mediating anxiolysis) rather than α1-containing receptors (mediating global sedation). This pattern would produce anxiolysis without sedation.
- Concurrent dopaminergic effect — the weak dopamine reuptake inhibition by kavain and methysticin would counterbalance any GABA-mediated sedation, maintaining alertness and reward-system activity that supports sociable interaction
- Concurrent MAO-B inhibition — yangonin and desmethoxyyangonin's MAO-B inhibition would prolong dopamine and phenethylamine availability, supporting alertness and mood
- Multi-receptor multi-mechanism convergence — the simultaneous action across four mechanisms produces a clinical signature no single-target drug reproduces
Whatever the mechanism, the practical implication is that kava occupies a clinical niche that no pharmaceutical anxiolytic occupies: an agent that reduces social anxiety enough to enable comfortable social engagement, without the cognitive blunting that would interfere with that engagement, without the disinhibition that creates problems with alcohol, and without the abuse liability that complicates benzodiazepine use in this context.
Cognitive Non-Impairment Trials
The "kava is not impairing" claim is one of the more rigorously documented findings in the kava literature, with multiple independent studies using validated cognitive performance batteries reaching similar conclusions.
Reaction Time and Information Processing
Heinze et al. (1994) administered standardized event-related potential (ERP) testing to volunteers given kava extract or placebo, measuring the P300 evoked response that indexes cortical information processing. The kava group showed unchanged or slightly enhanced P300 amplitude compared to placebo, contrasting sharply with the clear P300 reduction produced by oxazepam (a benzodiazepine) in the same paradigm.
Multiple subsequent studies have confirmed this finding. Simple and choice reaction time, digit-symbol substitution test performance, and trail-making test performance are all unaffected or marginally improved on kava at clinical doses. The pattern is consistent: kava produces measurable anxiolysis and subjective relaxation without measurable cognitive slowing.
Working Memory and Attention
Studies of working memory (n-back tasks, digit span) and sustained attention (Continuous Performance Test) on kava versus placebo and versus benzodiazepines have produced similar results. Kava does not impair working memory capacity or sustained attention performance. Benzodiazepines clearly do impair both.
Driving Simulator Performance
Driving simulator studies are particularly important practically because they capture integrated psychomotor performance under simulated real-world demands. Studies of driving simulator performance on kava have generally found no measurable impairment at standard anxiolytic doses (120–240 mg kavalactones). Higher doses, particularly in combination with alcohol or other CNS depressants, do impair driving performance. The practical implication is that standard kava doses are likely compatible with driving, while traditional "session" kava use (4–8 shells over an evening, delivering perhaps 1–2 g of kavalactones) is not.
Real-World Cognitive Performance
Several studies have measured complex real-world cognitive performance — arithmetic tasks, reading comprehension, problem-solving — on kava versus placebo and versus benzodiazepines. The consistent finding is that kava preserves complex cognitive performance to a degree that benzodiazepines, antihistamines, and other conventional anxiolytics do not.
Kava versus Alcohol on Cognitive Performance
The cognitive contrast between kava and alcohol is particularly stark and well-documented. Both are widely used as social lubricants. Both produce subjective relaxation and reduced social anxiety. Both engage GABA-A receptors. But they differ profoundly in their cognitive consequences.
Alcohol Cognitive Profile
- Measurable impairment of reaction time and motor coordination at blood alcohol concentrations as low as 0.02%
- Substantial impairment of complex psychomotor tasks (driving) at 0.05% and above
- Impairment of working memory, problem-solving, and decision-making
- Disinhibition leading to socially inappropriate behavior
- Anterograde amnesia at higher doses ("blackouts")
- Severe withdrawal syndrome on cessation after chronic heavy use (delirium tremens, seizures)
- Hepatotoxicity from chronic use
- Substantial neurotoxicity from chronic use (cerebellar atrophy, Wernicke-Korsakoff syndrome)
Kava Cognitive Profile
- No measurable impairment of reaction time at clinical doses
- Driving simulator performance preserved
- Working memory and complex problem-solving preserved
- No disinhibition; if anything, social judgment may be improved (consistent with the traditional ceremonial use for dispute resolution and political negotiation)
- No amnesia at clinical doses; very high traditional ceremonial doses produce subjective "fuzziness" but not blackout
- No significant withdrawal syndrome on cessation
- Hepatotoxicity concern with poor-quality preparations (covered in detail on the Benefits hub page); noble-cultivar aqueous root extracts have an excellent safety record
- No evidence of CNS neurotoxicity from chronic use
The implication is that for the use case alcohol has traditionally occupied in many cultures — social lubrication, end-of-day relaxation, mild anxiolysis — kava represents a categorically safer alternative in cognitive and neurological terms. The hepatotoxicity comparison is more nuanced (alcohol is unambiguously hepatotoxic; kava's hepatic safety depends on product selection) but for the cognitive and behavioral effects the comparison strongly favors kava.
The growing kava bar phenomenon in the United States and elsewhere is partly a response to this comparison: a venue where adults can engage in social relaxation without the cognitive and behavioral costs of alcohol.
Kava versus Benzodiazepines on Cognitive Performance
The cognitive contrast with benzodiazepines is similarly stark. The Heinze 1994 ERP study, multiple subsequent comparison trials, and meta-analytic synthesis all converge on the same finding: benzodiazepines produce measurable cognitive impairment across reaction time, working memory, attention, and complex psychomotor tasks. Kava does not.
The mechanism difference matters. Benzodiazepines act non-selectively at α1, α2, α3, and α5-containing GABA-A receptors. The α1 subtype mediates sedation. The α2/α3 subtypes mediate anxiolysis. The α5 subtype, enriched in the hippocampus, mediates the amnestic effect that is one of the hallmark side effects of benzodiazepines.
Kavalactones appear to act preferentially at non-α1, non-α5 sites, producing anxiolysis through α2/α3 modulation without the α1-mediated sedation or α5-mediated amnesia. This subunit selectivity is the leading explanation for the cognitive non-impairment.
The pharmaceutical industry has actively pursued α2/α3-selective benzodiazepine receptor modulators for decades, motivated by exactly this profile (anxiolysis without sedation or amnesia). The closest approved agent is bretazenil (limited use in some markets). No widely available pharmaceutical reproduces the kavalactone profile of selective α2/α3 modulation; this is one of kava's genuine pharmacological advantages.
The MAO-B Inhibition Hypothesis
The leading mechanistic hypothesis for kava's mood-elevating effect is reversible inhibition of monoamine oxidase B (MAO-B) by the kavalactones yangonin and desmethoxyyangonin. MAO-B is the mitochondrial enzyme principally responsible for catabolism of dopamine and trace amines (phenethylamine, benzylamine) in the central nervous system. MAO-A (the parallel isoform) is more important for serotonin and norepinephrine catabolism.
In vitro inhibition studies (Uebelhack et al. 1998) show yangonin and desmethoxyyangonin are reversible inhibitors of MAO-B at concentrations achievable with clinical kava doses, with IC50 values in the low micromolar range. The functional implication is that endogenous dopamine and phenethylamine would have somewhat longer half-life in the synapse during kava exposure, producing a mild mood-elevating effect mechanistically similar (but much weaker) to that of pharmaceutical MAO-B inhibitors like selegiline.
Why MAO-B inhibition would produce mood improvement: MAO-B inhibitors like selegiline are FDA-approved for major depression at sufficient dose, and have been used adjunctively in Parkinson's disease for both motor and mood effects for decades. The mechanism is presumed to be increased synaptic dopamine availability in mesolimbic and prefrontal pathways relevant to motivation, hedonic tone, and reward.
Clinical caveats:
- The in vitro MAO-B inhibition is reversible; this is different from irreversible inhibitors like classical MAOI antidepressants (phenelzine, tranylcypromine) that produce dietary tyramine restrictions
- The clinical magnitude of MAO-B inhibition in vivo at typical kava doses is unknown but likely modest
- Co-administration of MAOI antidepressants with kava should be avoided as a conservative measure, even though the risk of clinical serotonin syndrome or hypertensive crisis is theoretical rather than well-documented
- Concurrent SSRI use is generally considered acceptable but with caution, because the MAO-B effect of kava is small compared to that of pharmaceutical MAOIs that absolutely contraindicate SSRI co-administration
Dopamine Reuptake Inhibition Hypothesis
A complementary mechanistic hypothesis for kava's mood effect involves weak inhibition of the dopamine transporter (DAT) by kavain and methysticin. The dopamine transporter is the principal mechanism for clearing dopamine from the synaptic cleft after release; inhibition prolongs synaptic dopamine availability and increases postsynaptic stimulation.
The mechanism is the same as that of conventional stimulants (methylphenidate, amphetamines, cocaine) and atypical antidepressants like bupropion that produce mood elevation partly through this pathway. The pharmaceutical examples are all much stronger DAT inhibitors than kavain and methysticin; the kava effect appears mild based on in vitro data.
The behavioral signature is consistent with weak dopaminergic enhancement. Long-time kava users do not experience the stimulant rush of amphetamines or the euphoric peak of cocaine; they experience modestly elevated mood, slightly enhanced motivation for social engagement, and a sense of well-being. The absence of strong reinforcement explains the absence of abuse liability — kava is not subject to compulsive use patterns characteristic of dopamine-elevating drugs of abuse.
The convergence of weak MAO-B inhibition (less degradation of dopamine) plus weak DAT inhibition (less reuptake of dopamine) is mechanistically coherent: both increase synaptic dopamine, producing a mild and additive mood-elevating effect. The net result is the subjective experience of mood improvement without stimulation.
For broader context on dopamine and mood see our Depression page.
Mood Elevation Without Stimulant Character
The distinctive feature of kava's mood effect is that it is mood-elevating without being stimulating. This is unusual. Most mood-elevating agents fall into one of three classes:
- Stimulants — amphetamines, methylphenidate, caffeine; produce both mood elevation and energizing arousal
- Euphoriants — opioids, MDMA, alcohol; produce mood elevation with disinhibition and impairment
- Antidepressants — SSRIs, SNRIs, MAOIs, tricyclics, atypicals; produce mood normalization over weeks of treatment, with neutral or sedating acute effects
Kava is in none of these categories. Its acute effect is mood-elevating without arousal (unlike stimulants), without disinhibition or impairment (unlike alcohol or opioids), and without the multi-week delay of antidepressants. The closest pharmaceutical analog is selegiline (the MAO-B inhibitor) at low doses, which produces mild mood elevation without the cognitive or behavioral effects of typical antidepressants — consistent with the MAO-B mechanism being substantially responsible for kava's mood profile.
The practical implication is that kava occupies a clinical niche distinct from any pharmaceutical class. For the patient who wants mild mood elevation and reduced social anxiety without stimulation, without intoxication, without impairment, and without the multi-week onset of conventional antidepressants, kava is essentially the only available option.
Kava in Major Depressive Disorder Pilot Evidence
The Sarris KADSS depression sub-analysis (described above) was suggestive enough to motivate dedicated pilot investigation of kava in major depressive disorder. The 2018 Sarris et al. open-label pilot in adults with DSM-5 major depressive disorder treated 25 participants with aqueous noble-cultivar kava extract (250 mg kavalactones daily) for 4 weeks and measured changes in MADRS, HAM-D, and Bf-S scales.
Results:
- Mean MADRS reduction of approximately 7 points over 4 weeks
- Mean HAM-D reduction of approximately 6 points over 4 weeks
- Bf-S well-being scores improved significantly
- No significant changes in liver function tests over the 4-week period
- Minor adverse events (mild headache, fatigue) reported by approximately 30% of participants; no serious adverse events
The open-label design limits causal inference (no placebo control means the observed improvement cannot be attributed unambiguously to the kava effect). But the result is consistent with the depression sub-analysis from the placebo-controlled KADSS trial and motivates larger placebo-controlled investigation.
The clinical place for kava in depression is currently as an adjunct or alternative for patients with comorbid anxiety and depression who have not done well on first-line conventional therapy. It is not a replacement for SSRIs in severe major depressive disorder, where the effect size and time course of conventional therapy is better established. But for mild-to-moderate depression with prominent anxiety component, kava is a reasonable trial.
Cautions for the Mood Use Case
- MAOI antidepressants — absolute contraindication to combine with kava because of theoretical (though not well-documented in case reports) risk of hypertensive crisis or serotonin syndrome from the additive MAO inhibition
- SSRI antidepressants — relative contraindication; use combined therapy only with appropriate clinical oversight
- Bupropion — the dopaminergic enhancement is additive; theoretical risk of seizure threshold lowering; caution recommended
- Parkinson's disease — complex interaction with levodopa and other dopaminergic agents; case reports of worsened parkinsonian symptoms with chronic high-dose kava use; avoid in established Parkinson's disease
- Pre-existing mood disorder — bipolar disorder is a relative contraindication because of theoretical risk of mood destabilization from any agent affecting dopamine or MAO; use with psychiatric oversight if at all
- Substance use disorder — kava's subjective qualities, while not producing classical reinforcement or addiction, can become a focus of compulsive use in some individuals predisposed to behavioral addiction patterns. Caution in patients with history of alcohol use disorder or other substance use disorder.
- Concurrent benzodiazepines, z-drugs, opioids, or alcohol — additive CNS depression and (for alcohol) additive hepatic stress. Avoid the combinations.
- Hepatotoxicity from poor-quality extracts — the central caution, covered comprehensively on the Benefits hub page
- Pregnancy and breastfeeding — insufficient data; avoid
Key Research Papers
- Sarris J et al. (2013). Kava in the treatment of generalized anxiety disorder: depression sub-analysis (KADSS). Journal of Clinical Psychopharmacology. — PubMed
- Sarris J et al. (2009). The Kava Anxiety Depression Spectrum Study (KADSS) pilot. Psychopharmacology. — PubMed
- Uebelhack R et al. (1998). Inhibition of platelet MAO-B by kava pyrone-enriched extract from Piper methysticum Forster. Pharmacopsychiatry. — PubMed
- Baum SS, Böhler T, Krug M (1998). Modulation of mesolimbic dopamine release by kavain. Neuropsychopharmacology studies. — PubMed
- Heinze HJ et al. (1994). Pharmacopsychological effects of oxazepam and kava-extract in a visual search paradigm. Pharmacopsychiatry. — PubMed
- Münte TF et al. (1993). Effects of oxazepam and an extract of kava roots (Piper methysticum) on event-related potentials in a word recognition task. Neuropsychobiology. — PubMed
- Russell PN, Bakker D, Singh NN (1987). The effects of kava on alerting and speed of access of information from long-term memory. Bulletin of the Psychonomic Society. — PubMed
- Foo H, Lemon J (1997). Acute effects of kava, alone or in combination with alcohol, on subjective measures of impairment and intoxication and on cognitive performance. Drug and Alcohol Review. — PubMed
- Prescott J et al. (1993). Effects of acute doses of kava on cognitive performance. Drug and Alcohol Review. — PubMed
- LaPorte E et al. (2011). Neurocognitive effects of kava (Piper methysticum): a systematic review. Human Psychopharmacology. — PubMed
- Sarris J et al. (2018). Adjunctive nutraceuticals for depression: a systematic review and meta-analysis. American Journal of Psychiatry. — PubMed
- Smith K et al. (2018). Kava and the brain: a clinical and neuropsychopharmacological review. CNS Spectrums. — PubMed
PubMed Topic Searches
- PubMed: Kava and depression
- PubMed: Kava cognitive performance
- PubMed: Kavalactone MAO-B
- PubMed: Kava dopamine reuptake
- PubMed: Kava driving and psychomotor
Connections
- Kava Overview
- Kava Benefits Hub
- Kava for Anxiety
- Kava for Sleep
- Kava for Muscle Relaxation
- Depression
- Anxiety
- St. John's Wort
- Ashwagandha
- Rhodiola
- Valerian
- Passionflower
- Stress Management
- Natural Anxiety Relief
- Parkinson's Disease