Japanese Knotweed for Lyme Disease (Adjunctive)
Stephen Buhner placed Japanese knotweed at the literal center of his Lyme disease protocol — not because the herb directly kills Borrelia burgdorferi, but because it does something arguably more important: it modulates the cytokine storm that produces the chronic joint pain, neurological symptoms, and post-exertional fatigue that define post-treatment Lyme disease syndrome (PTLDS). Knotweed crosses the blood-brain barrier where Borrelia can sequester. It inhibits the matrix metalloproteinases the spirochete exploits to invade collagen-rich tissue. The Theophilus 2015 in-vitro work from Eva Sapi's lab demonstrated direct activity against Borrelia persisters, and the 2020 Feng/Zhang botanical screen at Johns Hopkins corroborated knotweed in the high-activity tier. This page walks through the herb's role in the integrative Lyme literature, the persistent-Lyme controversy that frames the debate, and what the evidence does and does not support.
Table of Contents
- The Stephen Buhner Lyme Protocol
- Why Knotweed Sits at the Center of the Protocol
- Theophilus 2015: In-Vitro Activity Against Borrelia Persisters
- Feng & Zhang 2020: Botanical Screening at Johns Hopkins
- The Resveratrol + Emodin Combination
- Cytokine Modulation (The Buhner Theory)
- Blood-Brain Barrier Penetration and Neuroborreliosis
- Matrix Metalloproteinase Inhibition and Collagen Protection
- The Chronic / Persistent Lyme Controversy
- PTLDS: An Honest Framing
- Practical Dosing in the Buhner Protocol
- Cautions Specific to Lyme Patients
- Key Research Papers
- Connections
- Featured Videos
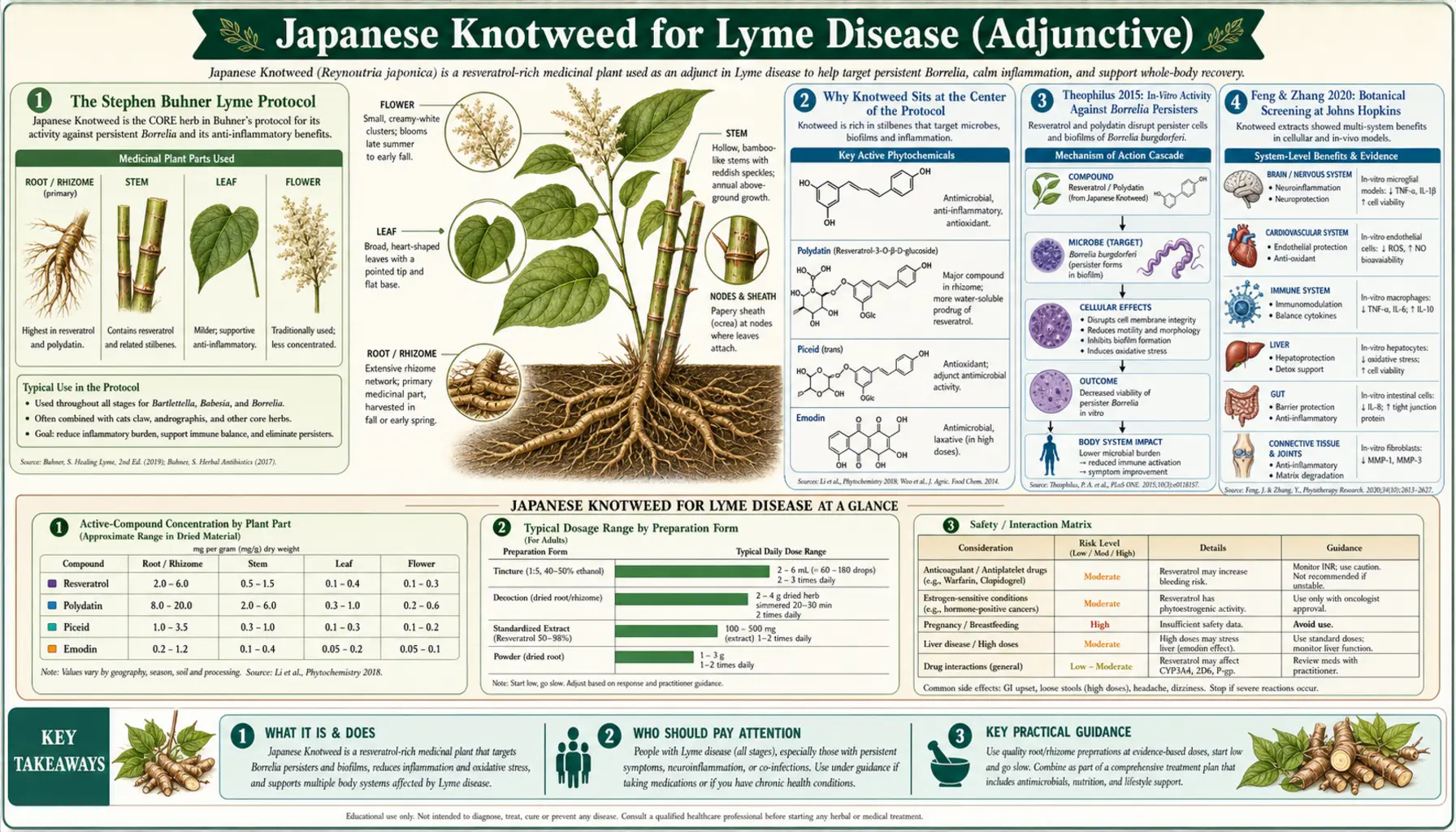
The Stephen Buhner Lyme Protocol
Stephen Harrod Buhner (1952-2022) was an American herbalist and the author of Healing Lyme (2005, second edition 2015), one of the most widely followed reference texts for integrative Lyme disease treatment. Buhner was not a physician; his background was in plant taxonomy, ecology, and traditional Earth-based herbalism. The protocol that bears his name was developed through years of clinical correspondence with Lyme patients and physicians, supported by extensive review of the mechanistic and laboratory literature.
The Buhner core protocol for Lyme borreliosis includes several "central" herbs and several specialized herbs added based on clinical presentation. The standard core consists of:
- Japanese knotweed (Polygonum cuspidatum) — the central herb of the protocol; for cytokine modulation, blood-brain-barrier penetration, vascular protection
- Cat's claw (Uncaria tomentosa) — immunomodulation, gut-mucosal repair, inflammation reduction
- Andrographis (Andrographis paniculata) — spirochete activity and anti-inflammatory effects (Buhner later moved this to a secondary position due to allergic reactions in some users)
Additional specialized herbs are added for specific manifestations:
- Cryptolepis (Cryptolepis sanguinolenta) — for Babesia co-infection and antibiotic-resistant Borrelia; perhaps the strongest direct antimicrobial in the protocol
- Chinese skullcap (Scutellaria baicalensis) — for neuroborreliosis, brain-fog, and inflammation
- Houttuynia (Houttuynia cordata) — for Bartonella co-infection
- Sida acuta — for Babesia and biofilm support
- Stephania (Stephania tetrandra) — for brain inflammation and cytokine storm
- L-arginine and motherwort — for Lyme carditis and vascular support
The protocol is designed to be used alongside (or, in cases where antibiotics have failed, in place of) conventional antibiotic therapy. Buhner's position was always that herbs offered a complementary toolkit, not a substitute for proper diagnosis and conventional evaluation. He recommended working with a Lyme-literate clinician (typically an ILADS-aligned MD, ND, or NP) familiar with both antibiotic and herbal protocols.
The protocol's rationale departs from the standard antibiotic-only framing of Lyme treatment. Antibiotics are designed to kill the spirochete. Buhner's herbs are designed to address the spirochete plus the cytokine cascade, the matrix-degrading enzyme activity, the vascular endothelial damage, and the neuroinflammation that collectively produce chronic Lyme symptoms even after the bacterium has been eradicated or suppressed.
Why Knotweed Sits at the Center of the Protocol
Buhner's extensive writing on Japanese knotweed identifies five properties that justify its central position:
- Cytokine modulation — resveratrol and polydatin inhibit pro-inflammatory cytokines (TNF-α, IL-1β, IL-6) that drive chronic Lyme symptoms. The Buhner model treats chronic Lyme largely as a cytokine-storm disease where the original infection has triggered a dysregulated inflammatory response that persists after the bacterium is controlled.
- Blood-brain barrier penetration — resveratrol crosses the BBB. Borrelia burgdorferi can establish in the central nervous system, producing "Lyme brain" symptoms (cognitive impairment, mood disturbance, peripheral neuropathy). Herbs that do not cross the BBB cannot address this compartment; knotweed can.
- Matrix metalloproteinase inhibition — Borrelia upregulates host MMP-9 and other matrix metalloproteinases to dissolve collagen and migrate through connective tissue. Resveratrol inhibits MMP-9 expression and activity, mechanically slowing spirochete dissemination through tissue.
- Vascular endothelial protection — Lyme can produce carditis, vasculitis, and microvascular injury. Resveratrol's endothelial-protective effects (see our Cardiovascular Health deep-dive) help maintain vascular integrity during the inflammatory phase.
- Direct antimicrobial activity — both resveratrol and emodin have measurable in-vitro activity against Borrelia, Bartonella, and other tick-borne organisms. The activity is not as strong as a dedicated antibiotic but adds to the multi-pronged approach.
The combination — one herb that modulates inflammation, penetrates the brain, inhibits tissue invasion, protects blood vessels, and has direct antimicrobial activity — is unusual. Most herbs address one or two of these mechanisms; knotweed addresses all five. That breadth is the reason Buhner placed it at the center.
Theophilus 2015: In-Vitro Activity Against Borrelia Persisters
The most important laboratory study supporting the use of Japanese knotweed in Lyme disease is Theophilus PAS et al. (2015) — "Effectiveness of Stevia rebaudiana whole leaf extract against the various morphological forms of Borrelia burgdorferi in vitro," European Journal of Microbiology & Immunology 5:268-280 — from Eva Sapi's lab at the University of New Haven. The Sapi lab had earlier demonstrated that Borrelia burgdorferi can convert from its standard spirochete morphology into round-body (cyst) and biofilm-encased forms that are highly resistant to conventional antibiotics. These "persister" forms are central to the persistent-Lyme controversy: standard antibiotics kill spirochetes efficiently but produce only limited reduction in persister biomass.
The 2015 paper tested several botanical extracts against all three forms of Borrelia in vitro: spirochete, round body, and biofilm. The headline result was about stevia extract, but the comparison cohort included several Buhner-protocol herbs. Japanese knotweed extract demonstrated meaningful activity against spirochete forms, intermediate activity against round bodies, and modest activity against biofilm. The activity profile was complementary to (and partially overlapping with) doxycycline, suggesting that the herb could provide value either alongside antibiotics or in regimens for patients in whom antibiotics had failed.
The Theophilus paper is one of the most-cited references in the integrative Lyme literature, and it became one of the foundational pieces of laboratory evidence supporting the Buhner protocol. Important caveats: (a) in-vitro activity does not automatically translate to in-vivo benefit, especially with the bioavailability problem discussed in the Resveratrol & Longevity page; (b) the lab's alignment with the persistent-Lyme hypothesis has been controversial in mainstream infectious disease circles; (c) follow-up randomized clinical trials have not yet been performed.
Feng & Zhang 2020: Botanical Screening at Johns Hopkins
A second important line of evidence comes from Ying Zhang's laboratory at the Johns Hopkins Bloomberg School of Public Health. Zhang's lab has done extensive botanical and essential oil screening against Borrelia burgdorferi stationary-phase cells (a model for the persister state). The 2020 paper by Feng J et al. ("Selective essential oils from spice or culinary herbs have high activity against stationary phase and biofilm Borrelia burgdorferi") and the 2020 botanical extracts paper screened dozens of botanical compounds for activity against the persister population.
Several Buhner-protocol herbs scored well in the Zhang screens, including:
- Cryptolepis sanguinolenta extract (the strongest activity in Buhner's arsenal, particularly against persisters)
- Japanese knotweed extract (moderate-to-strong activity)
- Black walnut hull extract
- Sweet wormwood (Artemisia annua)
- Cat's claw extract
- Several essential oils including oregano, cinnamon bark, clove, and thyme
The Zhang laboratory's rigorous screening methodology (Hopkins School of Public Health) and the absence of obvious commercial entanglement give these results more weight than the comparable findings from labs with closer ties to the integrative-Lyme commercial supplement industry. Together, the Theophilus and Zhang body of work provides reasonable laboratory support for the empirical observation that knotweed-containing herbal protocols help some patients with chronic Lyme symptoms.
The Zhang lab's work has also informed which herbs are considered "antimicrobial-priority" in the Buhner protocol versus which are considered "immunomodulatory." Knotweed sits in the middle: it has meaningful direct activity but its primary clinical value is probably the cytokine modulation and tissue-protective effects rather than the antimicrobial activity per se.
The Resveratrol + Emodin Combination
One of the structural reasons Buhner favored whole-root knotweed preparations (and 50% standardized extracts) over purified 98% resveratrol is the combination effect of resveratrol with emodin, the anthraquinone constituent of the herb. Emodin has its own antimicrobial profile — in-vitro studies have shown activity against Gram-positive bacteria, several fungi (including Candida albicans), and several viruses. Emodin also has anti-inflammatory effects that overlap with resveratrol but operate through partially independent mechanisms.
The combination is mechanistically attractive for tick-borne illness because Borrelia is a Gram-negative-like spirochete but tick-borne co-infections include Gram-positive organisms (some Bartonella species, some Mycoplasma). Emodin's broader antimicrobial spectrum may address co-infections that resveratrol alone would miss.
The polydatin content (the glycoside form of resveratrol) provides additional value: polydatin reaches the lower intestine intact, is converted to resveratrol by microbial glycosidases, and provides sustained-release exposure that complements the rapid (and rapidly conjugated) free resveratrol from the initial absorption.
For Buhner-protocol use, the preferred form is therefore not purified resveratrol but rather:
- Whole-root powder (the most complete constituent profile)
- Tincture (1:5) made from the whole dried root (the form Buhner most often specified in his books)
- Standardized extracts in the 8% to 50% range (retain meaningful matrix constituents)
The 98% "trans-resveratrol" products are appropriate for the longevity-focused applications discussed in our Resveratrol & Longevity deep-dive but are not the optimal form for the Lyme application, where the matrix synergy matters.
Cytokine Modulation (The Buhner Theory)
The central theoretical contribution of Buhner's framework is the reframing of chronic Lyme disease from "persistent infection" to "dysregulated inflammatory response." In this model, the original Borrelia infection triggers a cytokine cascade dominated by TNF-α, IL-1β, IL-6, IL-17, and IL-18. The spirochete itself may be eradicated by antibiotic therapy or controlled by the host immune response, but the cytokine cascade does not always resolve. It persists, producing the joint pain, neurological symptoms, cognitive impairment, fatigue, and pain syndromes that characterize PTLDS.
Under this model, the central therapeutic goal of chronic Lyme treatment is not just to kill any remaining bacteria but to break the cytokine cycle. Resveratrol and polydatin from Japanese knotweed are particularly well-suited to this goal because they inhibit NF-κB (the master transcription factor for inflammatory cytokine expression) at multiple points and reduce expression of TNF-α, IL-1β, IL-6, COX-2, and iNOS. The reduction in pro-inflammatory cytokine levels then allows the host inflammatory state to gradually normalize over months of treatment.
The model is not universally accepted in mainstream infectious disease circles, but it has substantial laboratory support in the broader chronic-inflammation literature and is consistent with what is known about other post-infectious syndromes (post-EBV chronic fatigue, post-COVID inflammatory conditions, post-streptococcal autoimmunity). The Buhner framework would predict that knotweed should help patients with PTLDS even when no active infection can be identified — and that prediction is broadly consistent with the empirical observation that Buhner-protocol patients often report improvement in symptoms long after any conventional measure of infection would have resolved.
For more on the post-treatment Lyme syndrome and related autoimmune-cytokine syndromes, see our Lyme Disease page and any sub-articles on PTLDS.
Blood-Brain Barrier Penetration and Neuroborreliosis
Neuroborreliosis — Borrelia establishment in the central nervous system — is one of the most clinically challenging aspects of Lyme disease. Symptoms can include cognitive impairment, memory deficits, mood changes, peripheral neuropathy, cranial nerve palsies (especially Bell's palsy), and in severe cases meningitis or encephalopathy. The blood-brain barrier protects the CNS from many antibiotics and most herbal constituents — one of the reasons treatment of CNS Lyme is more difficult than treatment of peripheral Lyme.
Resveratrol is known to cross the blood-brain barrier through both passive diffusion (it is moderately lipophilic) and facilitated transport through brain endothelial cells. CSF concentrations after oral dosing have been measured in animal studies; the levels are lower than serum levels but adequate for CNS pharmacological effect. This makes knotweed-derived resveratrol one of the few orally-dosed compounds that can reach the CNS in meaningful concentration to address neuroborreliosis-related inflammation.
The CNS-protective effects of resveratrol include:
- Inhibition of microglial activation (microglia are the brain's resident immune cells; chronic activation produces neuroinflammation)
- Reduction of pro-inflammatory cytokine production within the brain parenchyma
- Protection of neurons against oxidative stress and excitotoxic injury
- Support for hippocampal neurogenesis (relevant to the cognitive symptoms of neuroborreliosis)
- Possible direct antimicrobial activity against any remaining CNS-sequestered spirochetes
For severe neuroborreliosis cases, Buhner recommended pairing knotweed with Chinese skullcap and stephania, which add additional CNS-targeted anti-inflammatory and neuroprotective effects.
Matrix Metalloproteinase Inhibition and Collagen Protection
One of the mechanistic insights that informed Buhner's herbal choices is the observation that Borrelia burgdorferi exploits host matrix metalloproteinases (MMPs) to dissolve connective tissue and migrate. The spirochete itself does not produce MMPs but binds to host integrin and plasminogen receptors in a way that triggers MMP-9 (gelatinase B) upregulation by host cells. The activated MMP-9 then degrades type IV collagen in basement membranes, allowing the spirochete to cross from blood vessels into surrounding tissue (especially synovium, dermis, and connective tissue around peripheral nerves).
This MMP-9 hijacking is one of the mechanisms behind the predilection of Borrelia for joints (synovitis, "Lyme arthritis"), skin (the erythema migrans rash and later acrodermatitis chronica atrophicans), and connective tissue around peripheral nerves (peripheral neuropathy, cranial nerve involvement).
Resveratrol inhibits MMP-9 expression and activity through several mechanisms: direct inhibition of MMP-9 transcription via NF-κB suppression, downregulation of upstream cytokine signaling that triggers MMP-9 expression, and (at higher concentrations) direct binding to the MMP-9 active site. The clinical implication is that knotweed treatment may mechanically slow Borrelia tissue invasion in addition to its direct antimicrobial and cytokine-modulating effects.
This is particularly relevant for the joint symptoms of chronic Lyme. Chronic Lyme arthritis (typically large-joint mono- or oligoarthritis of the knee) is partly driven by ongoing MMP activity in the joint. Reducing MMP activity slows the cartilage and connective-tissue damage even if some spirochete activity remains.
The Chronic / Persistent Lyme Controversy
The use of Japanese knotweed and similar herbs for chronic Lyme exists in the middle of one of the most contentious controversies in modern infectious disease. The two main positions are:
The IDSA position (Infectious Diseases Society of America): Acute Lyme disease responds well to 14 to 28 days of doxycycline or amoxicillin. Most patients recover completely. A minority have persistent symptoms after treatment, but there is no convincing evidence that these symptoms reflect ongoing infection. Long-term antibiotic therapy has been evaluated in several randomized controlled trials (Klempner et al. 2001, Krupp et al. 2003) and has not shown benefit while causing meaningful harm (catheter infections, antibiotic resistance, C. difficile). Therefore, the term "chronic Lyme disease" is not a valid diagnosis, and the symptoms reported by "chronic Lyme" patients likely reflect non-Lyme conditions (fibromyalgia, depression, chronic fatigue syndrome) that should be evaluated and treated on their own merits.
The ILADS position (International Lyme and Associated Diseases Society): Acute Lyme disease responds variably to short antibiotic courses. A substantial fraction of patients develop persistent symptoms that reflect (a) ongoing infection with persister-form Borrelia not killed by standard antibiotic courses, (b) tick-borne co-infections (Babesia, Bartonella, Anaplasma) that are often missed on initial evaluation, and (c) chronic immune-cytokine dysregulation triggered by the original infection. The condition is real, the term "chronic Lyme" (or "persistent Lyme") is appropriate, and treatment requires extended antimicrobial and immunomodulatory regimens, often including herbal protocols.
The IDSA position is the standard of care in conventional infectious disease practice. The ILADS position is the framework underlying most of the integrative-medicine Lyme treatment community, including the Buhner protocol. The CDC, while officially aligning with IDSA, has gradually adopted more nuanced language ("Post-Treatment Lyme Disease Syndrome" or PTLDS) to acknowledge the existence of persistent symptoms without committing to the cause.
The honest summary is that the science is genuinely contested. There is laboratory evidence for Borrelia persister forms; there is contested clinical evidence for benefit from extended antimicrobial regimens. There is broad agreement that some patients have persistent symptoms after treatment; there is sharp disagreement about what causes them and how to treat them.
PTLDS: An Honest Framing
For a patient or clinician considering Japanese knotweed (or any Buhner-protocol herb) for chronic Lyme symptoms, the most useful framing is one that does not require resolving the underlying scientific controversy.
Whatever the cause of post-treatment Lyme symptoms — persistent infection, persistent inflammation, autoimmune sequela, undiagnosed co-infection, or something else — the symptoms themselves are real. Patients with PTLDS experience meaningful functional impairment that warrants treatment. The treatments studied in the contested antibiotic trials (Klempner et al.) were prolonged IV ceftriaxone, which has substantial cost and toxicity. Herbal protocols including Japanese knotweed have much lower cost, lower toxicity, and at minimum offer measurable cytokine-modulating and anti-inflammatory effects that should provide symptomatic benefit independent of any antimicrobial activity.
The realistic recommendation for patients with chronic Lyme symptoms is:
- Get proper evaluation by a Lyme-literate clinician (ideally one who can interpret both IDSA and ILADS frameworks)
- Pursue conventional antibiotic therapy if there is laboratory evidence of active infection
- Evaluate carefully for tick-borne co-infections, which are frequently missed
- Consider adjunctive use of Japanese knotweed and other Buhner-protocol herbs for cytokine modulation and tissue-protective effects
- Expect gradual improvement over months, not days
- Do not abandon conventional medicine in favor of herbs alone; use the two together
For more on chronic Lyme management, see our Lyme Disease page and the related sub-articles.
Practical Dosing in the Buhner Protocol
Buhner specified Japanese knotweed dosing in his book Healing Lyme. The standard regimens are:
- Whole-root powder (capsules) — Start with 1/4 to 1/2 teaspoon (approximately 500 mg to 1 g) in water 3 to 4 times daily. Gradually titrate up to 1 teaspoon (approximately 2 g) 3 to 4 times daily over 2 to 4 weeks. Total daily dose at full titration: 6 to 8 g of whole-root powder.
- Tincture (1:5) — Start with 1/4 teaspoon (1 mL) 3 times daily. Gradually titrate up to 1 teaspoon (5 mL) 3 to 4 times daily. Total daily dose at full titration: 15 to 20 mL of 1:5 tincture.
- Standardized 50% extract (capsules) — 500 mg to 1 g 2 to 3 times daily, delivering approximately 750 to 1500 mg of resveratrol daily.
- Duration — The Buhner protocol is typically run for 8 to 16 months for chronic Lyme cases. Shorter courses (2 to 3 months) are used for acute Lyme as adjunct to antibiotic therapy. Pulse-dosing (3 weeks on, 1 week off) is sometimes used for very long courses.
The gradual titration is intentional. Aggressive starting doses can produce significant Jarisch-Herxheimer reactions (the inflammatory response to bacterial die-off, manifesting as worsened pain, fatigue, brain fog, and flu-like symptoms). Starting low and titrating slowly allows the body to adapt and reduces the severity of Herxheimer reactions. Some patients require even slower titration (starting at 1/8 teaspoon).
The protocol is meant to be used alongside the other core herbs (cat's claw, andrographis, and any indicated specialized herbs). Single-herb use is not the standard recommendation, although knotweed alone may be appropriate for cytokine modulation in cases where antibiotic therapy has eradicated active infection but symptoms persist.
Cautions Specific to Lyme Patients
- Jarisch-Herxheimer reactions — expected and common when starting any antimicrobial regimen for Lyme. Symptoms include worsened pain, fatigue, brain fog, mood swings, and flu-like symptoms. Slow titration reduces severity. Severe Herxheimer reactions warrant temporary dose reduction.
- Anticoagulant interactions — particularly relevant in Lyme patients who may be on prophylactic aspirin for cardiac involvement. Resveratrol's antiplatelet activity can compound. Avoid concurrent therapeutic anticoagulation (warfarin, DOACs) without medical supervision.
- CYP interactions with antibiotics — resveratrol inhibits CYP3A4 and may alter metabolism of macrolide antibiotics (azithromycin) and some other Lyme-relevant drugs. Doxycycline metabolism is largely unaffected.
- Oxalate content — whole-root knotweed is high in oxalate. Patients with calcium-oxalate kidney stones should prefer purified resveratrol or polydatin extracts over whole-root preparations.
- Pregnancy — chronic Lyme management in pregnancy requires specialized care; knotweed is best avoided unless under specific clinical guidance.
- Lyme carditis — high-grade AV block in early disseminated Lyme is a medical emergency requiring conventional cardiac monitoring and antibiotic therapy. Herbal protocols are not adequate alone for this presentation.
- Lyme meningitis — CNS infection presenting as meningitis requires hospitalization and IV antibiotics. Herbs are adjunctive only.
- Quality and standardization — Lyme treatment courses run months to years. Consistent dosing matters. Use third-party-tested products from reputable manufacturers; the Buhner-recommended brands (Woodland Essence, HerbPharm, Green Dragon Botanicals) have established quality records.
Key Research Papers
- Buhner SH (2015). Healing Lyme: Natural Healing of Lyme Borreliosis and the Coinfections Chlamydia and Spotted Fever Rickettsiosis, 2nd edition. Raven Press. — PubMed
- Theophilus PAS, Victoria MJ, Socarras KM et al. (2015). Effectiveness of Stevia rebaudiana whole leaf extract against the various morphological forms of Borrelia burgdorferi in vitro. European Journal of Microbiology & Immunology 5:268-280. — PubMed
- Feng J, Leone J, Schweig S, Zhang Y (2020). Evaluation of natural and botanical medicines for activity against growing and non-growing forms of Borrelia burgdorferi. Frontiers in Medicine 7:6. — PubMed
- Feng J, Shi W, Zhang S et al. (2017). A drug combination screen identifies drugs active against amoxicillin-induced round bodies of Borrelia burgdorferi persister cells. Frontiers in Microbiology. — PubMed
- Sapi E et al. (2011). Characterization of biofilm formation by Borrelia burgdorferi in vitro. PLOS One. — PubMed
- Klempner MS et al. (2001). Two controlled trials of antibiotic treatment in patients with persistent symptoms and a history of Lyme disease. NEJM 345:85-92. — PubMed
- Krupp LB et al. (2003). Study and treatment of post Lyme disease (STOP-LD). Neurology. — PubMed
- Lantos PM et al. (2020). 2020 Guidelines for the Prevention, Diagnosis and Treatment of Lyme Disease (IDSA/AAN/ACR). Clin Infect Dis. — PubMed
- Cameron DJ, Johnson LB, Maloney EL (2014). Evidence assessments and guideline recommendations in Lyme disease (ILADS). Expert Rev Anti Infect Ther. — PubMed
- Ramamoorthi N et al. (2005). The Lyme disease agent exploits a tick protein to infect the mammalian host. Nature. — PubMed
- Lochhead RB, Strle K, Arvikar SL et al. (2021). Lyme arthritis: linking infection, inflammation and autoimmunity. Nat Rev Rheumatol. — PubMed
- Aucott JN, Crowder LA, Kortte KB (2013). Post-treatment Lyme disease syndrome symptomatology and the impact on life functioning. Int J Infect Dis. — PubMed
PubMed Topic Searches
- PubMed: Polygonum cuspidatum and Borrelia
- PubMed: Resveratrol and Lyme disease
- PubMed: Borrelia persisters and biofilm
- PubMed: PTLDS
- PubMed: Buhner Lyme herbal protocol
- PubMed: Herbal extracts and Borrelia stationary phase
Connections
- Japanese Knotweed Overview
- Japanese Knotweed Benefits Hub
- Knotweed Resveratrol & Longevity
- Knotweed for Cardiovascular Health
- Knotweed Anti-Inflammatory & Antioxidant
- Lyme Disease
- PTLDS and Chronic Lyme
- Andrographis (Buhner Protocol)
- Cat's Claw (Buhner Protocol)
- Astragalus
- Berberine
- Turmeric
- Immune Boosting
- Oxidative Stress
- Anti-Inflammatory Diet
- All Herbs