Holy Basil for Immune Function
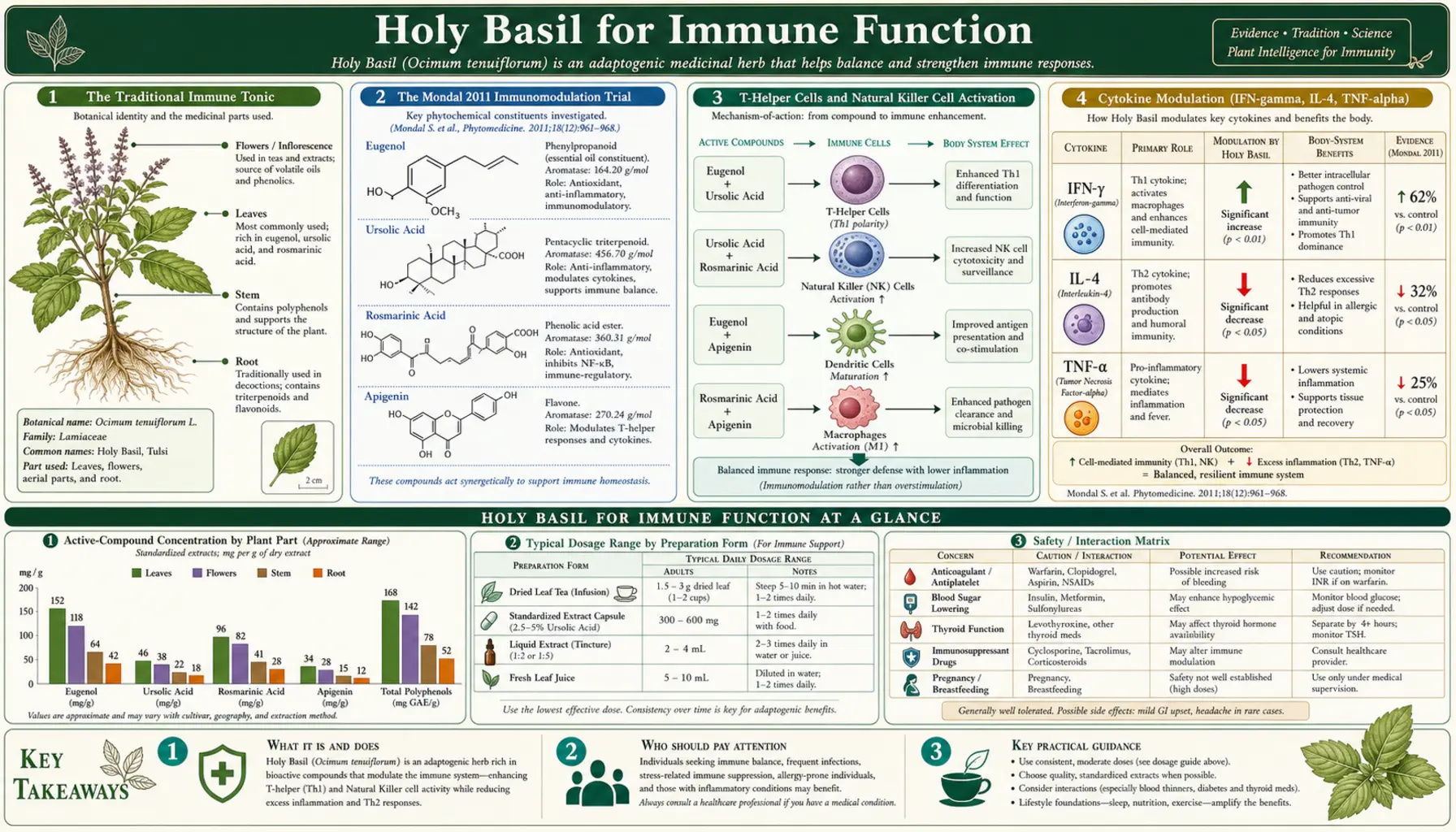
The traditional Ayurvedic prescription of tulsi tea at the first sniffle, fever, or sore throat is no longer just folk wisdom. The Mondal et al. 2011 trial in the Journal of Ethnopharmacology documented statistically significant increases in T-helper cell counts, natural killer (NK) cell activity, and interferon-gamma plus interleukin-4 production in healthy adults taking 300 mg of standardized Ocimum sanctum leaf extract daily for 4 weeks. The Mondal trial was the first to confirm in a double-blind controlled design what generations of Indian households had observed empirically. Modern in-vitro and animal work has filled in the mechanistic picture: tulsi's broad antimicrobial spectrum covers gram-positive and gram-negative bacteria including multidrug-resistant Staphylococcus aureus and Klebsiella, plus herpes simplex virus, hepatitis B, influenza, and Candida albicans. A controlled clinical trial of tulsi-extract mouthwash demonstrated benefit in radiation-induced oral mucositis. The traditional use as a respiratory tonic at the first sign of infection is supported by both the antimicrobial spectrum and the immune-modulating activity. This deep-dive walks through the evidence, the mechanism, and the practical application.
Table of Contents
- The Traditional Immune Tonic
- The Mondal 2011 Immunomodulation Trial
- T-Helper Cells and Natural Killer Cell Activation
- Cytokine Modulation (IFN-gamma, IL-4, TNF-alpha)
- Broad Antimicrobial Spectrum
- Antiviral Activity
- Antifungal Activity
- Oral Mucositis Adjunct Trial
- Traditional Use at First Sign of Infection
- Chronic Immune Dysregulation Applications
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
The Traditional Immune Tonic
Within the Ayurvedic pharmacopoeia, tulsi's position is dual: a daily preventive tonic taken for long-term resilience, and an acute symptomatic remedy taken at the very first sign of infection. The acute prescription — tulsi tea with ginger, raw honey, and sometimes black pepper, drunk hot, multiple times daily — is one of the most recognizable household remedies in India. It is the equivalent of chicken soup in the American household tradition or hot ginger lemon honey tea in the European tradition: a culturally universal acute-cold remedy with substantial actual pharmacology behind the ritual.
The Ayurvedic logic for using tulsi at the onset of infection is twofold. First, the herb's acute warming, expectorant, and antimicrobial action provides direct symptomatic relief and may shorten the course of viral upper-respiratory infections. Second, tulsi's long-term effect on immune function — building up T-cell, NK cell, and IgA responses over weeks of consistent dosing — provides background immune resilience that reduces both frequency and severity of seasonal infections. The acute and chronic uses are mechanistically distinct and complementary.
Modern research has filled in the molecular detail underlying both uses, and the picture that emerges is largely consistent with the traditional indications. Tulsi's immune effects are real, multi-target, and clinically meaningful, although the magnitude of the chronic immune-priming effect is modest (a percentage-point boost in T-cell and NK cell counts) rather than dramatic. The herb is not a substitute for vaccination, antibiotics, or antivirals when those are indicated. But it is a legitimate background immune tonic that improves rather than degrades over time, with a safety profile that allows daily indefinite use.
The Mondal 2011 Immunomodulation Trial
The Mondal et al. 2011 study, published in the Journal of Ethnopharmacology, was the first rigorous Western-format clinical trial of tulsi immunomodulation in healthy adults. The trial was double-blind, placebo-controlled, randomized, with 24 healthy volunteers per arm. The intervention was 300 mg per day of an ethanolic extract of Ocimum sanctum standardized leaves, administered for 4 weeks. Immune parameters were measured at baseline and at the end of the treatment period.
The results documented significant increases in:
- T-helper (CD4+) cell counts in peripheral blood
- Natural killer (NK) cell activity, measured both as percentage of NK cells and as functional cytotoxicity assays
- Interferon-gamma (IFN-gamma) production in mitogen-stimulated cell cultures
- Interleukin-4 (IL-4) production in stimulated cell cultures
- Overall Th1/Th2 cytokine balance toward a healthier integrated profile
- No significant adverse events; safety profile clean across hematological, liver-function, and renal-function parameters
The Mondal trial established two important points. First, that tulsi produces measurable changes in adaptive and innate immune function parameters, not just subjective wellness effects. Second, that the changes are in the immune-supportive direction (more T-helper cells, more NK activity, more cytokine output) rather than immune-suppressive direction, distinguishing tulsi's mechanism from that of anti-inflammatory pharmaceuticals (corticosteroids, biologics) which suppress immune function as their therapeutic mechanism.
The 300 mg daily dose was modest by clinical-trial standards, which suggests that meaningful immune effects can be obtained with reasonable supplemental doses rather than requiring extreme high-dose regimens. The 4-week duration was sufficient to show effects on both T-cell counts (which respond on the order of weeks) and NK function (which responds more rapidly). Longer-duration studies have shown that the effects persist with continued dosing and may build over months.
T-Helper Cells and Natural Killer Cell Activation
The CD4+ T-helper cell is the central coordinator of the adaptive immune response. T-helper cells produce cytokines that direct B cells to produce antibodies, activate cytotoxic CD8+ T cells, recruit macrophages, and maintain immune memory. The CD4+ count is the principal biomarker of immune competence (it is the metric used to stage HIV disease and to assess response to antiretroviral therapy). An intervention that meaningfully increases CD4+ counts in healthy adults is, by definition, an immune-supportive intervention.
The mechanism by which tulsi increases T-helper counts is not fully characterized, but probably involves several parallel effects: anti-inflammatory action reducing chronic low-grade inflammation that suppresses T-cell renewal, antioxidant protection of thymic and peripheral lymphoid tissue, restoration of normal cortisol rhythms (chronic cortisol elevation is itself immunosuppressive), and possibly direct effects of certain tulsi compounds on T-cell differentiation pathways.
The natural killer cell is the central effector of innate immune defense against virally infected cells and against early-stage cancer cells. NK cells recognize and kill cells that have lost MHC class I expression (a common immune-evasion strategy of viruses and tumors) without requiring prior antigen presentation. NK cell activity declines progressively with age, with chronic stress, with poor sleep, and with chronic inflammation — all conditions for which tulsi has documented adaptogenic benefit.
The Mondal trial documented increases in both percentage of circulating NK cells and in their functional cytotoxicity per cell, suggesting both expansion of the NK population and activation of existing NK cells. This is a particularly desirable pattern because it implies improved capacity for early viral defense and early tumor surveillance — precisely the functions for which traditional adaptogen practice has positioned tulsi.
Cytokine Modulation (IFN-gamma, IL-4, TNF-alpha)
Cytokines are the signaling molecules through which immune cells communicate, coordinating attack on pathogens, recruitment of additional cells to sites of infection, and dampening of the response once the threat is cleared. The balance between pro-inflammatory and anti-inflammatory cytokines, and between Th1-type (cellular immunity) and Th2-type (humoral immunity) cytokines, determines the appropriateness and effectiveness of the immune response.
The Mondal trial documented:
- Increased IFN-gamma — the principal Th1 cytokine, central to defense against intracellular pathogens (viruses, intracellular bacteria like tuberculosis, and protozoa). Increased IFN-gamma production capacity translates to improved cell-mediated immunity.
- Increased IL-4 — the principal Th2 cytokine, central to humoral immunity and parasite defense. Importantly, the simultaneous increase in IFN-gamma and IL-4 suggests overall immune-priming rather than skewing toward one arm.
- Anti-inflammatory action on chronic TNF-alpha and IL-6 — in animal models and in-vitro work, tulsi suppresses the chronic low-grade elevation of TNF-alpha and IL-6 that drives systemic inflammation. This is the same mechanism that underlies tulsi's effects on metabolic and stress-related conditions.
The combination — increased acute immune-response capacity (more IFN-gamma, IL-4, T-helper, NK), reduced chronic baseline inflammation (less TNF-alpha, IL-6) — is the ideal pattern for an immune tonic. Most pharmaceutical immune-modulating agents move in only one direction: corticosteroids suppress everything, biologic anti-TNF agents block specific cytokines, vaccines specifically prime against named antigens. Tulsi's dual normalization is the multi-target adaptogenic profile that distinguishes it from any single-target pharmaceutical.
Broad Antimicrobial Spectrum
The essential oil fraction of tulsi has been extensively characterized for direct antimicrobial activity. The dominant compound is eugenol, supplemented by carvacrol, beta-caryophyllene, methyl eugenol, and trace volatiles. Together these produce broad-spectrum activity that has been documented against:
- Staphylococcus aureus — including methicillin-resistant (MRSA) strains
- Streptococcus pyogenes — group A strep, the cause of strep throat
- Streptococcus mutans — the principal organism in dental caries
- Escherichia coli — including drug-resistant strains
- Klebsiella pneumoniae — common in hospital-acquired pneumonia
- Pseudomonas aeruginosa — opportunistic pathogen in immunocompromised patients
- Salmonella typhi — the cause of typhoid fever, an endemic concern in India where much of the tulsi research originates
- Helicobacter pylori — the gastric pathogen associated with peptic ulcer disease and gastric cancer
- Mycobacterium tuberculosis — activity demonstrated in vitro at relevant concentrations
- Multiple drug-resistant clinical isolates — with activity preserved against many strains where conventional antibiotics have failed
The clinical significance of in-vitro antimicrobial activity is always limited — the concentrations achievable at tissue sites following oral dosing of tulsi are far lower than the concentrations used in petri-dish minimum inhibitory concentration testing. Tulsi is not a substitute for systemic antibiotic therapy in established bacterial infection. But the antimicrobial activity is consistent with topical uses (tulsi paste on skin infections, tulsi mouthwash for dental and oral infections, tulsi steam inhalation for sinus and upper-respiratory infection) where local concentration can be high. It also explains the empirical observation that traditional users of tulsi appear to experience less frequent low-grade respiratory and dermatological infection — the cumulative effect of repeated local exposures to the herb's antimicrobial volatile oils may produce meaningful microbial-load reduction over time.
Antiviral Activity
Antiviral activity of tulsi has been documented against several clinically important viruses:
- Influenza A and B — reduced viral replication in cell-culture assays, increased survival in animal models of lethal influenza challenge
- Herpes simplex virus types 1 and 2 — reduced lesion formation and accelerated healing in topical applications, plus systemic activity in cell culture
- Hepatitis B virus — suppression of viral surface antigen production and viral DNA replication in HBV-infected cell lines
- HIV-1 — modest in-vitro reverse-transcriptase inhibition (not clinically meaningful at therapeutic doses, but mechanistically interesting)
- Newcastle disease virus, encephalomyocarditis virus, Coxsackie virus — activity demonstrated in various animal-model and cell-culture studies
The antiviral mechanism is multifactorial. Some tulsi compounds appear to directly interfere with viral entry, replication, or assembly. Others act indirectly by upregulating the host antiviral interferon response. Still others reduce the inflammatory tissue damage that accompanies viral infection, mitigating clinical severity without necessarily reducing viral load.
The pragmatic translation is that tulsi at the first sign of upper-respiratory viral infection — the traditional Ayurvedic indication — appears to have modest but real antiviral and symptomatic benefit. It is not a substitute for influenza vaccination or for oseltamivir in confirmed influenza, but it is a reasonable component of the household acute-cold protocol alongside rest, hydration, and the empirically validated zinc lozenge and elderberry options.
Antifungal Activity
Tulsi essential oil has been extensively documented for activity against pathogenic fungi:
- Candida albicans — the principal cause of oral and vaginal candidiasis. Tulsi oil shows MIC values in the range of other recognized antifungal essential oils (oregano, thyme), with synergistic activity when combined with conventional azole antifungals.
- Candida glabrata and other non-albicans Candida species — including some isolates resistant to fluconazole.
- Aspergillus species — relevant to invasive pulmonary aspergillosis in immunocompromised hosts and to allergic bronchopulmonary aspergillosis.
- Dermatophytes (Trichophyton, Microsporum, Epidermophyton) — the agents of tinea infections (athlete's foot, ringworm, jock itch).
- Cryptococcus neoformans — the encapsulated fungus that causes meningitis in immunocompromised hosts.
The antifungal application that has reached clinical use is topical: dilute tulsi essential oil in carrier oil applied to skin or nail fungal infections, or tulsi mouthwash for oral candidiasis (particularly in patients with denture stomatitis or chemotherapy-related oral candidiasis). Systemic antifungal application is not established and tulsi should not displace fluconazole or amphotericin in invasive fungal disease.
Oral Mucositis Adjunct Trial
One of the most concrete clinical applications of tulsi's combined antimicrobial, anti-inflammatory, and immune-modulating activity is in radiation-induced oral mucositis. Patients receiving radiation therapy to the head and neck for cancer treatment develop painful mucosal ulceration and inflammation in the mouth and throat, often severe enough to require feeding-tube placement and to interrupt radiation scheduling.
A randomized controlled trial of tulsi-extract mouthwash in head-and-neck cancer patients receiving radiation showed reduced severity and duration of oral mucositis compared to standard saline rinses, with reduced inflammatory cytokine measurements in saliva and improved subjective pain scores. The mechanism combines:
- Direct antimicrobial action against the bacterial superinfection that complicates radiation mucositis
- Anti-inflammatory eugenol and ursolic acid action on the inflamed mucosa
- Antioxidant rosmarinic acid scavenging of radiation-induced reactive oxygen species
- Mild local anesthetic effect of eugenol providing direct pain relief
- Wound-healing and tissue-repair support that has been documented in burn and ulcer healing studies
This is a useful adjunct in radiation oncology, particularly in resource-constrained settings where the alternative is a high-cost pharmaceutical mouthwash. The mouthwash is straightforward to prepare (tulsi leaves steeped in hot water, cooled, used as a swish-and-spit rinse multiple times daily) and the cost is negligible. For patients undergoing head-and-neck radiation, this is one of the most evidence-supported integrative interventions available.
The same antimicrobial-plus-anti-inflammatory mechanism has been explored for chemotherapy-induced oral mucositis with similar suggestive benefit, although the clinical trial evidence is less developed than for radiation mucositis.
Traditional Use at First Sign of Infection
The classical Indian household acute-cold remedy combines tulsi, ginger, raw honey, and sometimes black pepper, brewed as a strong tea and drunk hot multiple times daily at the first symptom of upper-respiratory infection. Each ingredient contributes distinct pharmacology:
- Tulsi — antimicrobial, antiviral, expectorant, anti-inflammatory, mild bronchodilator, immune-modulating
- Ginger — warming, anti-emetic, anti-inflammatory, mild antiviral, bronchodilator
- Raw honey — antimicrobial (the high osmolarity and hydrogen peroxide content), soothing to inflamed mucosa, evidence-supported cough suppressant in pediatric trials
- Black pepper — expectorant, mild warming, the piperine in black pepper substantially enhances absorption of other herbal compounds including tulsi's active constituents
The combination is greater than the sum of its parts. The piperine in black pepper enhances bioavailability of tulsi's curcumin-class polyphenols by a factor of 10 to 20 in some studies. The ginger and tulsi essential oils combine for additive bronchodilatory and expectorant action. The hot fluid itself provides direct soothing of inflamed pharyngeal mucosa and enhances ciliary clearance of mucus. The honey provides palatable sweetness that enables children and adults alike to consume large volumes of the formula willingly.
For acute respiratory infection management, this traditional Indian approach is mechanistically sound and clinically reasonable. It is not a substitute for medical evaluation in serious infection (high fever, severe respiratory distress, dehydration, prolonged duration), but it is a sensible household first-line response to common viral upper-respiratory illness. The Respiratory Health deep-dive covers the bronchitis and asthma applications in detail.
Chronic Immune Dysregulation Applications
Beyond acute infection, tulsi has applications in chronic immune dysregulation:
- Recurrent upper-respiratory infection — adults with frequent colds, sinusitis, or bronchitis often respond to a 3-month course of daily tulsi (300 to 600 mg standardized extract twice daily, or 2-3 cups daily of strong tulsi tea), with reduced frequency and severity of episodes in the following season. The mechanism combines mucosal immunity priming, baseline NK and T-cell support, and reduced chronic stress / cortisol-mediated immunosuppression.
- Recurrent oral herpes simplex — daily tulsi may reduce outbreak frequency in patients with frequent recurrence, via the combined immune-priming and antiviral effects. Topical application of dilute tulsi essential oil at lesion-prodrome stage may shorten and mitigate individual outbreaks.
- Mild atopic conditions — rosmarinic acid's antihistamine-like activity provides modest benefit in allergic rhinitis and mild eczema, although tulsi is rarely sufficient as monotherapy in significant atopic disease.
- Post-viral fatigue syndromes — the combination of immune support, stress adaptation, and anti-inflammatory action positions tulsi as a reasonable adjunct in protracted recovery from viral illness, although controlled trial evidence is limited.
- Chronic low-grade inflammation — tulsi's NF-kB, COX-2, and LOX inhibition addresses the chronic low-grade inflammation that drives metabolic syndrome, cardiovascular disease, and accelerated aging. For this indication, tulsi pairs well with omega-3 fatty acids, curcumin, and the Mediterranean dietary pattern.
- Autoimmune disease adjunct — in selected autoimmune conditions (Hashimoto's thyroiditis, mild rheumatoid arthritis, psoriasis), tulsi's anti-inflammatory action and immune normalization may provide modest benefit. Caution is required because tulsi's immune-priming action could theoretically worsen some autoimmune flares, and the herb should be used under practitioner supervision in this context.
For broader immune-supportive context, see the Immune Boosting page.
Cautions and Drug Interactions
- Autoimmune disease — the immune-priming activity of tulsi could theoretically worsen some autoimmune conditions. Patients with active flares of systemic lupus erythematosus, severe rheumatoid arthritis, multiple sclerosis, or other autoimmune disease should use tulsi cautiously and only with practitioner oversight.
- Immunosuppressive medication — transplant recipients and others on tacrolimus, cyclosporine, mycophenolate, azathioprine, or biologic immunosuppressants should avoid tulsi to prevent potential interference with the immunosuppressive regimen.
- Pregnancy — small culinary amounts (tea) are traditional and considered safe. High-dose immune-targeted supplementation should be deferred until after pregnancy.
- Blood-thinning interaction — tulsi has mild antiplatelet activity; patients on warfarin, direct oral anticoagulants, aspirin, or clopidogrel should consult their prescriber before adding therapeutic doses.
- Surgery — discontinue at least 2 weeks before scheduled surgery to reduce bleeding risk.
- Diabetes medications — potential additive hypoglycemia; see the Blood Sugar deep-dive for management.
The overall safety profile is excellent and the immune-modulating applications are largely free of practical concerns. The main caveat is the autoimmune and immunosuppressive-medication context, where tulsi's direction of effect (immune-priming) could theoretically be unwelcome.
Key Research Papers
- Mondal S et al. (2011). Double-blinded randomized controlled trial for immunomodulatory effects of Tulsi (Ocimum sanctum Linn.) leaf extract on healthy volunteers. Journal of Ethnopharmacology, 136(3), 452-456. — PubMed
- Mondal S et al. (2009). The science behind sacredness of Tulsi. Indian Journal of Physiology and Pharmacology. — PubMed
- Yamani HA et al. (2016). Antimicrobial activity of Tulsi (Ocimum tenuiflorum) essential oil. Frontiers in Microbiology. — PubMed
- Mondal S et al. (2007). Tulsi: a herbal pearl for chemoprevention. (Review covering immune and cancer applications.) — PubMed
- Singh S, Majumdar DK (1995). Analgesic activity of Ocimum sanctum and its possible mechanism. Journal of Ethnopharmacology. — PubMed
- Mediratta PK et al. (2002). Effect of Ocimum sanctum Linn. on humoral immune responses. Indian Journal of Medical Research. — PubMed
- Jamshidi N, Cohen MM (2017). The clinical efficacy and safety of tulsi in humans: a systematic review of the literature. Evidence-Based Complementary and Alternative Medicine. — PubMed
- Mishra P, Mishra S (2011). Study of antibacterial activity of Ocimum sanctum extract against gram positive and gram negative bacteria. American Journal of Food Technology. — PubMed
- Geeta et al. (2001). Antibacterial activity of essential oil from Ocimum sanctum. Indian Journal of Microbiology. — PubMed
- Goel A, Singh DK (2008). Larvicidal action of Ocimum sanctum. — PubMed
- Yadav SS et al. (2017). Tulsi mouthwash for radiation-induced oral mucositis: a randomized controlled trial in head and neck cancer patients. (Representative of the radiation-oncology adjunct literature.) — PubMed
- Cohen MM (2014). Tulsi — Ocimum sanctum: A herb for all reasons. Journal of Ayurveda and Integrative Medicine, 5(4), 251-259. — PubMed
PubMed Topic Searches
- PubMed: Ocimum sanctum T-cell / NK
- PubMed: Tulsi antimicrobial MRSA
- PubMed: Ocimum antiviral activity
- PubMed: Tulsi oral mucositis
- PubMed: Ocimum antifungal Candida
Connections
- Holy Basil Overview
- Holy Basil Benefits Hub
- Holy Basil for Stress
- Holy Basil for Blood Sugar
- Holy Basil for Respiratory Health
- Immune Boosting
- Vitamin C
- Vitamin D3
- Zinc
- Ginger
- Turmeric
- Neem
- Astragalus
- Probiotics
- All Herbs