Holy Basil for Blood Sugar and Diabetes
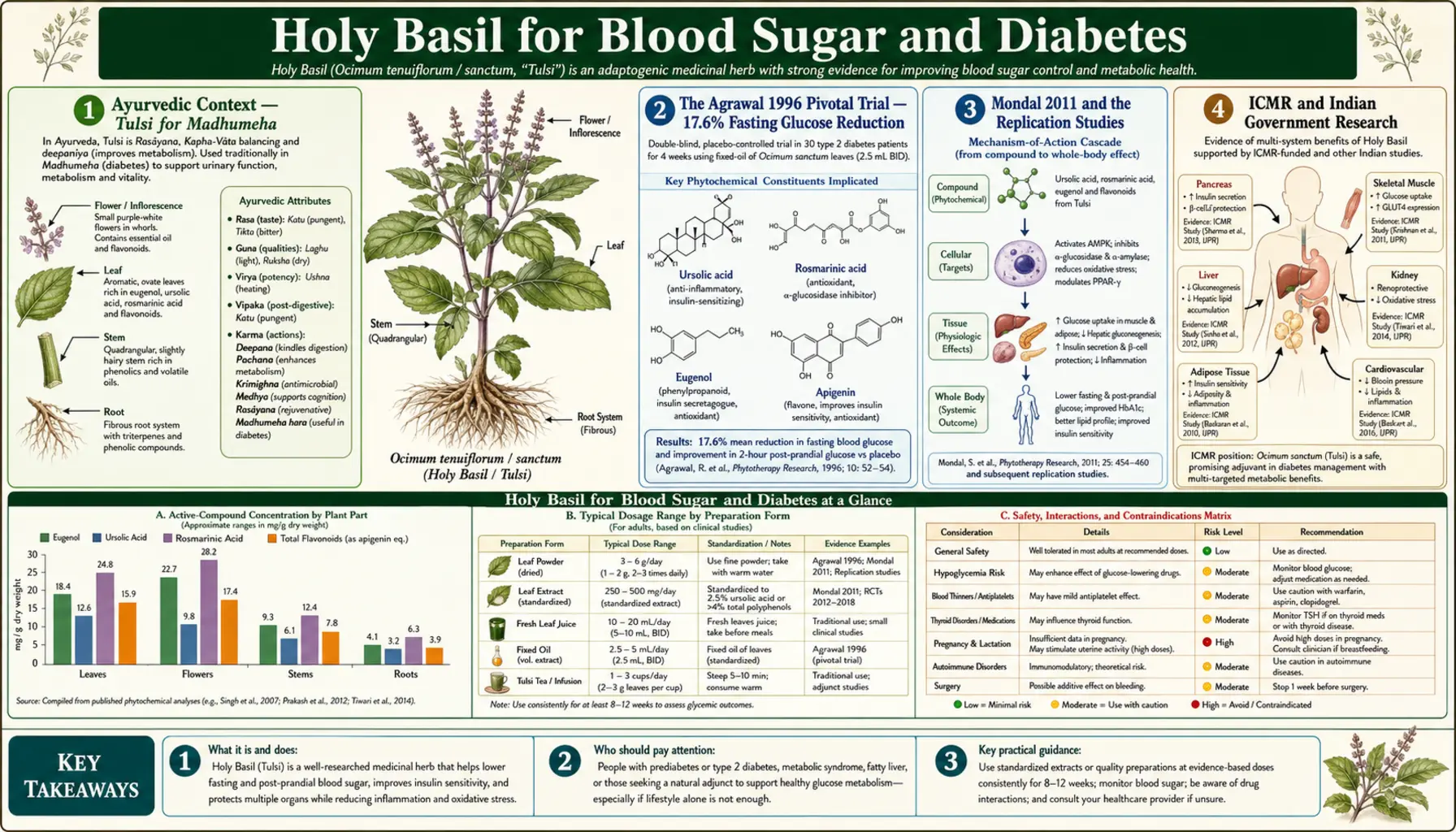
The glycemic effects of holy basil are not folklore. The Agrawal 1996 randomized, placebo-controlled, single-blind trial in the International Journal of Clinical Pharmacology and Therapeutics documented a 17.6% reduction in fasting blood glucose and a 7.3% reduction in postprandial glucose in patients with type 2 diabetes after just 4 weeks of tulsi leaf powder treatment. That is an effect size in the range of first-generation oral hypoglycemic medications — from a 2.5-gram daily dose of dried leaf powder. Subsequent trials by Mondal and others, the Indian Council of Medical Research (ICMR) reviews, and the Suanarunsawat group at Ramkhamhaeng University have replicated and extended the finding. The mechanism is multi-target: ursolic acid increases muscle and liver insulin sensitivity via AMPK activation, eugenol inhibits alpha-amylase and alpha-glucosidase (slowing carbohydrate digestion), the whole-plant matrix supports pancreatic beta-cell function, and the herb's anti-inflammatory action addresses the chronic low-grade inflammation that drives insulin resistance. This deep-dive walks through the trials, the mechanism, and the practical regimen for adults using tulsi as part of an integrated metabolic protocol.
Table of Contents
- Ayurvedic Context — Tulsi for Madhumeha
- The Agrawal 1996 Pivotal Trial — 17.6% Fasting Glucose Reduction
- Mondal 2011 and the Replication Studies
- ICMR and Indian Government Research
- Mechanism: Insulin Sensitivity (Ursolic Acid & AMPK)
- Mechanism: Pancreatic Beta-Cell Support
- Mechanism: Carbohydrate Digestion (Alpha-Glucosidase Inhibition)
- Mechanism: Inflammation as Root Driver of Insulin Resistance
- Tulsi vs Metformin, Sulfonylureas, and Other Oral Agents
- Practical Dosing Regimen for Diabetes Support
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
Ayurvedic Context — Tulsi for Madhumeha
In classical Ayurveda, diabetes is madhumeha — literally "sweet urine." The condition is described in detail in the Sushruta Samhita (circa 600 BCE), which subdivides it into twenty subtypes by humoral predominance and includes recognizably modern symptom descriptions: polyuria, polydipsia, polyphagia, weight loss, recurrent infections, slow wound healing, and complications affecting the eyes, kidneys, and peripheral nerves. The Ayurvedic understanding of diabetes long predated insulin's 1921 discovery and produced a substantial herbal pharmacopoeia for the condition. Holy basil sits within that pharmacopoeia, alongside jamun (Indian blackberry seeds), methi (fenugreek), karela (bitter melon), and vijaysar (Pterocarpus marsupium).
Tulsi's specific role in madhumeha treatment was as a daily preventive tonic for individuals with constitutional risk and as an adjunct in established disease alongside diet and other herbs. The classical prescription was 5 to 8 fresh leaves chewed daily on an empty stomach, often combined with neem leaves and turmeric. This regimen produced — centuries before the molecular basis was understood — what modern clinical trials would later confirm: meaningful reductions in fasting and postprandial blood glucose, with no toxicity at the dose used.
The modern integration of Ayurvedic herbal medicine with conventional diabetes care in India is well-established. Hospitals attached to AYUSH (Ministry of Ayurveda, Yoga, Unani, Siddha and Homoeopathy) routinely use tulsi in protocols for early type 2 diabetes, often as part of multi-herb formulations, and the Government of India Pharmacopoeia of Ayurveda includes tulsi monographs with quality and purity standards. This integration has produced the clinical-trial literature that established tulsi's glycemic credentials in Western scientific terms.
The Agrawal 1996 Pivotal Trial — 17.6% Fasting Glucose Reduction
The Agrawal et al. 1996 study, published in the International Journal of Clinical Pharmacology and Therapeutics, is the foundation of the modern tulsi-and-diabetes literature. It was a randomized, placebo-controlled, single-blind crossover trial in 40 patients with non-insulin-dependent diabetes (type 2). The intervention was 2.5 grams per day of fresh holy basil leaf powder, taken on an empty stomach, for 4 weeks. The control phase was 4 weeks on placebo. Each patient served as their own control via the crossover design.
The primary outcomes at the end of the treatment phase, compared to baseline, were:
- Fasting blood glucose: 17.6% reduction (mean reduction approximately 21 mg/dL from a starting mean of 134 mg/dL)
- Postprandial blood glucose: 7.3% reduction
- Mean total cholesterol: mild reduction
- Urine glucose (Benedict's test): reduction in semiquantitative score
- Safety: no adverse events reported; lipid profile, liver function, and kidney function unchanged
For context, the 17.6% fasting glucose reduction is in the range expected from a low-to-moderate dose of metformin (which typically produces 20 to 30% reduction in fasting glucose) or a first-generation sulfonylurea like glibenclamide (which typically produces 15 to 25% reduction). This is not the magnitude of effect you would expect from a dietary supplement — it is in the pharmacological range. The Agrawal trial used a modest 4-week intervention, and longer-duration studies have shown that effects increase over time as cumulative insulin sensitization develops.
The trial had limitations: single-blind rather than double-blind, modest sample size, single-center, and outcomes measured by blood glucose rather than HbA1c (which had not yet become the standard glycemic biomarker). But the magnitude of effect was so striking and the safety profile so clean that the paper became the founding citation for modern tulsi diabetes research.
Mondal 2011 and the Replication Studies
The Mondal et al. 2011 trial published in the Journal of Ethnopharmacology was primarily focused on immune outcomes (covered on the Immune Function deep-dive) but also documented metabolic effects. The trial used 300 mg of Ocimum sanctum ethanolic leaf extract daily for 4 weeks in healthy volunteers. Glycemic outcomes included modest reductions in fasting glucose even in non-diabetic subjects, consistent with the herb's overall insulin-sensitizing rather than insulin-secretory mechanism.
Other modern glycemic studies include:
- Rai et al. 1997 — Indian study showing reductions in fasting and post-meal blood sugar in type 2 diabetics on 1 to 2 grams of tulsi leaf powder daily over 1 month, replicating the Agrawal direction and magnitude.
- Somasundaram et al. 2012 — comparison of tulsi leaf juice versus glibenclamide in alloxan-induced diabetic rats, finding comparable glycemic reduction with tulsi at clinically reasonable doses.
- Suanarunsawat et al. 2010, 2011, 2014 — Thai research group documenting effects of tulsi essential oil on lipid metabolism, hepatic glucose handling, and oxidative-stress markers in high-fat-diet-fed rats, providing extensive mechanistic detail.
- Kochhar et al. 2009 — combination trial of tulsi with neem leaf powder in type 2 diabetics, showing greater glycemic effect than either herb alone, consistent with the traditional Ayurvedic practice of combining the two.
- Devra et al. 2012 — prospective study of tulsi extract in metabolic syndrome, documenting improvements in fasting glucose, HOMA-IR (insulin resistance index), triglycerides, and HDL.
- Satapathy et al. 2017 — double-blind RCT in type 2 diabetics, with the tulsi arm showing statistically significant reductions in fasting glucose, postprandial glucose, and HbA1c over 12 weeks. This is one of the few trials to include HbA1c as an outcome and is the strongest replication of the Agrawal effect to date.
The trials use different preparations (fresh leaves, dried leaf powder, ethanolic extract, standardized extract), different doses, and different patient populations, which complicates direct comparison. But the direction of effect is consistent across studies, populations, and preparation types — tulsi produces meaningful reduction in fasting and postprandial glucose with effect sizes in the lower pharmaceutical range.
ICMR and Indian Government Research
The Indian Council of Medical Research (ICMR), India's premier government biomedical research body, has been a major sponsor of tulsi pharmacology research over the past four decades. ICMR-funded work has included:
- Bulk-scale chemical characterization of tulsi extracts and identification of the principal bioactive compounds
- Standardization protocols for tulsi leaf powder and extracts to support quality control in pharmaceutical manufacturing
- Multi-center clinical trials in type 2 diabetes, hypertension, and stress-related conditions
- Safety pharmacology and toxicology studies establishing the upper-bound dosing for safe chronic use
- Integration protocols for tulsi within standard diabetic care, published as ICMR guidance for AYUSH-affiliated hospitals
The ICMR position, summarized in successive editions of the Pharmacopoeia of Ayurveda, is that tulsi is an established adjunct in the management of early type 2 diabetes, with evidence supporting its use alongside dietary modification, exercise, and standard pharmacological care. The ICMR does not position tulsi as a substitute for insulin or oral hypoglycemics in advanced disease — the evidence does not support that — but as a useful adjunct that can sometimes reduce required pharmaceutical dosing and may delay progression from impaired fasting glucose to overt diabetes in at-risk individuals.
This integrated approach reflects the broader Indian medical model, where Ayurvedic and conventional approaches coexist in a regulated framework, with each having defined roles. The Indian experience over decades of integration provides clinical evidence that complements the formal randomized-trial literature.
Mechanism: Insulin Sensitivity (Ursolic Acid & AMPK)
Insulin resistance — the failure of peripheral tissues (muscle, liver, adipose) to respond normally to insulin signaling — is the central pathophysiologic defect of type 2 diabetes. Restoring insulin sensitivity is the central therapeutic target, and is the principal mechanism by which metformin (the first-line oral diabetic agent) produces benefit. Holy basil targets this same mechanism through ursolic acid.
Ursolic acid, a pentacyclic triterpenoid concentrated in holy basil leaves and stems, activates AMP-activated protein kinase (AMPK) in muscle and liver tissue. AMPK is a cellular energy sensor that responds to low ATP availability by switching metabolism toward catabolic, energy-producing pathways. When AMPK is activated:
- GLUT4 glucose transporters translocate to the muscle cell surface, increasing insulin-independent glucose uptake
- Insulin signaling downstream of the insulin receptor is enhanced, restoring sensitivity
- Hepatic gluconeogenesis (the production of new glucose by the liver) is suppressed, reducing fasting glucose
- Fat oxidation increases at the expense of fat storage, gradually improving body composition
- Inflammatory cytokine production is suppressed, addressing the inflammatory driver of insulin resistance
This is essentially the same mechanism by which metformin produces its glycemic effect (metformin also activates AMPK, by a different upstream mechanism). The ursolic-acid effect in tulsi is modest in magnitude compared to a full pharmacological dose of metformin, but it is mechanistically the same kind of intervention — insulin sensitization rather than insulin secretion. This explains why tulsi tends not to cause hypoglycemia even at high doses in non-diabetic subjects (it does not push insulin output; it enhances tissue response to existing insulin) and why it pairs well with metformin without producing additive hypoglycemia.
Mechanism: Pancreatic Beta-Cell Support
Type 2 diabetes is also characterized by progressive failure of pancreatic beta cells — the islet cells that produce insulin. By the time most patients are diagnosed, they have already lost 40 to 50% of beta-cell function, and the failure continues progressively under glucotoxicity and lipotoxicity. Standard pharmaceutical agents have varying effects on beta-cell health: sulfonylureas (glibenclamide, glipizide) flog the beta cells to produce more insulin but accelerate their failure; metformin is beta-cell neutral; GLP-1 agonists and SGLT2 inhibitors may preserve beta-cell function; thiazolidinediones do as well.
Holy basil compounds appear to support beta-cell function through several mechanisms. Tulsi leaf extracts have been shown in animal models of streptozotocin-induced diabetes to preserve beta-cell mass, reduce beta-cell apoptosis under glucotoxic conditions, and increase beta-cell insulin content. The protective effect appears to be mediated by the herb's antioxidant compounds (rosmarinic acid, eugenol) reducing the oxidative-stress damage that drives beta-cell loss, plus possible direct effects of certain triterpenes on beta-cell regeneration pathways.
The clinical translation is that tulsi is plausibly disease-modifying rather than just glycemic-symptom-controlling, although this has not been formally demonstrated in long-duration human trials. The mechanism supports the traditional Ayurvedic positioning of tulsi as a preventive tonic in pre-diabetic individuals and as a beta-cell-preserving adjunct in early type 2 diabetes — both contexts where slowing the progression of beta-cell loss has more value than glycemic symptom control alone.
Mechanism: Carbohydrate Digestion (Alpha-Glucosidase Inhibition)
A third mechanism contributing to the postprandial-glucose effect is direct inhibition of carbohydrate-digesting enzymes in the gut lumen. Tulsi extracts demonstrate significant inhibition of alpha-amylase (which breaks down starches) and alpha-glucosidase (which breaks down disaccharides into absorbable monosaccharides). This is the same mechanism used by the pharmaceutical class of alpha-glucosidase inhibitors (acarbose, miglitol) used in some diabetes regimens.
The clinical effect is to slow postprandial glucose absorption, blunting the post-meal glucose spike. This is mechanistically distinct from insulin sensitization or insulin secretion — tulsi's alpha-glucosidase inhibition acts in the gut lumen before glucose has been absorbed, while the AMPK and beta-cell effects act after glucose enters circulation. The 7.3% postprandial glucose reduction in the Agrawal trial is likely driven primarily by this gut-luminal mechanism, while the 17.6% fasting glucose reduction is driven primarily by the insulin-sensitization and beta-cell-supportive mechanisms.
This three-mechanism convergence — AMPK-mediated insulin sensitization, beta-cell preservation, and alpha-glucosidase inhibition — is unusual for a single herb. Most pharmaceutical antidiabetic agents act through one mechanism. The multi-target action of tulsi explains why the glycemic effects appear durable and additive with conventional therapy rather than redundant with any single existing class.
Mechanism: Inflammation as Root Driver of Insulin Resistance
The modern understanding of type 2 diabetes positions chronic low-grade inflammation as a root upstream driver of insulin resistance. Adipose tissue in obesity becomes inflamed, releasing TNF-alpha, IL-6, and resistin into circulation. These cytokines interfere with insulin signaling at the receptor level, producing systemic insulin resistance. The inflammatory hypothesis is supported by the success of anti-inflammatory interventions (salicylates, IL-1 blockade) at improving glycemic control in patients with type 2 diabetes and inflammatory comorbidities.
Holy basil's broad anti-inflammatory action — ursolic acid suppressing NF-kB activation, eugenol inhibiting COX-2, rosmarinic acid inhibiting LOX and scavenging ROS, all working through different pathways — provides a mechanistically coherent route to addressing this upstream driver. The effect is not specific to diabetes; it is a general anti-inflammatory tone restoration. But because chronic low-grade inflammation is the upstream driver of insulin resistance, the general anti-inflammatory action produces specific glycemic benefit.
This is part of why the glycemic effects of tulsi tend to build over weeks rather than producing acute drops, and why they appear durable even after dose reduction — the anti-inflammatory effect requires time to develop and the resulting insulin sensitization persists. It is also why tulsi pairs well with other anti-inflammatory interventions (omega-3 fatty acids, curcumin, regular exercise, weight loss) for additive benefit in the metabolic syndrome / pre-diabetic / early diabetic population.
Tulsi vs Metformin, Sulfonylureas, and Other Oral Agents
Tulsi is best understood as a complementary intervention, not a replacement, for standard oral antidiabetic agents in established type 2 diabetes:
- vs metformin — mechanistically similar (both AMPK activators), with metformin producing a larger glycemic effect. Tulsi pairs well with metformin without additive hypoglycemia, can sometimes reduce required metformin dosing, and may add insulin-sensitization, beta-cell-preservation, and anti-inflammatory benefits beyond metformin alone. Tulsi may be a useful first-line alternative for patients who cannot tolerate metformin (GI side effects, vitamin B12 depletion concerns, renal function limits).
- vs sulfonylureas (glibenclamide, glipizide) — mechanistically opposite (sulfonylureas push insulin secretion; tulsi sensitizes tissues to existing insulin). Tulsi avoids the beta-cell-burning and weight-gain effects of sulfonylureas. Co-administration risks additive hypoglycemia and should be done with blood-sugar monitoring; sulfonylurea dose reductions are sometimes possible.
- vs SGLT2 inhibitors (empagliflozin, dapagliflozin) — complementary mechanisms (SGLT2 inhibitors increase urinary glucose excretion; tulsi addresses insulin sensitivity and inflammation). SGLT2 inhibitors carry recently-recognized cardiovascular and renal protective benefits that tulsi does not match in pharmaceutical-grade evidence. Tulsi remains a sensible adjunct.
- vs GLP-1 agonists (semaglutide, liraglutide) — GLP-1 agonists are highly effective injectable agents with significant weight-loss benefit but high cost, gastrointestinal side effects, and contraindications. Tulsi is mechanistically distinct, lower cost, and tolerable; it does not substitute for GLP-1 effect but can complement it.
- vs insulin — insulin is required when endogenous insulin production has failed substantially. Tulsi does not substitute for insulin therapy in insulin-dependent diabetes (whether type 1 or advanced type 2). It may modestly reduce insulin requirements in some patients via improved peripheral insulin sensitivity, but should not displace insulin therapy.
- vs other glycemic herbs — bitter melon, fenugreek, gymnema, jamun (Indian blackberry), berberine, and cinnamon all have research support for glycemic effects of various magnitudes. Tulsi has perhaps the cleanest safety profile and the most documented multi-target mechanism. Many traditional Ayurvedic protocols combine several of these.
For a broader treatment of natural metabolic approaches, see the Blood Sugar page and the Diabetes page.
Practical Dosing Regimen for Diabetes Support
For glycemic effect, dose ranges from the clinical trials provide reasonable guidance:
- Fresh leaf powder — 2 to 5 grams (approximately 1 to 2 teaspoons) daily of dried tulsi leaf powder, taken on an empty stomach 30 minutes before breakfast. This matches the Agrawal trial dose closely and produces the most consistent fasting-glucose effect.
- Tulsi tea — 2 to 3 cups daily of strong tulsi tea, ideally one cup 30 minutes before breakfast and additional cups before lunch and dinner. The pre-meal timing matters because the alpha-glucosidase inhibition effect requires the herb to be present in the gut when carbohydrates arrive.
- Standardized extract — 300 to 600 mg twice daily of a standardized extract (OciBest, Holy Basil Force from New Chapter, KSM-66 holy basil, or similar). Convenient for travel and dose-adjustment.
- Fresh leaves — 8 to 10 fresh tulsi leaves chewed on an empty stomach in the morning, the most traditional preparation. Requires access to fresh plants but provides the most concentrated essential-oil fraction.
- Combination protocols — traditional Indian combinations include tulsi with fenugreek seed powder, bitter melon (karela), and turmeric. Western integrative practitioners often add berberine (500 mg twice daily), cinnamon, and Vitamin D3 to baseline tulsi regimens for metabolic-syndrome patients.
Expect to see modest improvements in fasting glucose within 2 to 4 weeks, with continuing improvement over 12 weeks as anti-inflammatory and insulin-sensitization effects accumulate. Monitor with home glucose testing (especially if on insulin or sulfonylureas), with periodic HbA1c every 3 months. As glycemic control improves, expect that prescribed pharmaceutical doses may need downward adjustment to avoid hypoglycemia — coordinate with the prescribing physician rather than self-adjusting.
Cautions and Drug Interactions
- Hypoglycemia in combination with insulin or sulfonylureas — the most important practical caution. Patients on glibenclamide, glimepiride, glipizide, repaglinide, or insulin who add therapeutic doses of tulsi should monitor blood glucose closely and may need pharmaceutical dose reduction. Tulsi alone does not typically cause hypoglycemia, but it adds to existing hypoglycemic agents.
- Blood-thinning interaction — tulsi's antiplatelet effects can add to warfarin, direct oral anticoagulants, aspirin, or clopidogrel. Patients on these medications should consult their prescriber before adding therapeutic-dose tulsi.
- Surgery — discontinue tulsi at least 2 weeks before scheduled surgery due to both bleeding risk and hypoglycemia risk under anesthesia.
- Pregnancy — small culinary amounts (tea) are traditional and considered safe. High-dose supplementation is not recommended in pregnancy due to insufficient safety data.
- Pre-existing low blood pressure — tulsi has mild antihypertensive effects via eugenol's calcium-channel blocking action. Patients with baseline hypotension should monitor and start at low dose.
- Fertility — animal studies at very high doses (well above human therapeutic doses) have shown reduced sperm count. Couples actively trying to conceive may wish to use lower doses.
- Thyroid medications — mild anti-thyroid effects have been reported at high doses. Monitor TSH in patients on levothyroxine if adding sustained high-dose tulsi.
The overall safety profile is excellent and the drug interactions are manageable with awareness. The dominant practical issue is the hypoglycemia interaction with insulin and sulfonylureas, which is genuinely additive and requires monitoring.
Key Research Papers
- Agrawal P et al. (1996). Randomized placebo-controlled, single-blind trial of holy basil leaves in patients with noninsulin-dependent diabetes mellitus. International Journal of Clinical Pharmacology and Therapeutics, 34(9), 406-409. — PubMed
- Rai V et al. (1997). Effect of Ocimum sanctum leaf powder on blood lipoproteins, glycated proteins and total amino acids in patients with non-insulin-dependent diabetes mellitus. Journal of Nutritional Environmental Medicine. — PubMed
- Satapathy S et al. (2017). Effect of tulsi (Ocimum sanctum Linn.) supplementation on metabolic parameters and liver enzymes in young overweight and obese subjects. Indian Journal of Clinical Biochemistry. — PubMed
- Mondal S et al. (2011). Double-blinded randomized controlled trial for immunomodulatory effects of tulsi leaf extract on healthy volunteers. Journal of Ethnopharmacology, 136(3), 452-456. (Includes glycemic outcomes.) — PubMed
- Suanarunsawat T et al. (2010). Antihyperlipidemic and cardioprotective effects of Ocimum sanctum Linn. fixed oil. Journal of Lipids. — PubMed
- Kochhar A et al. (2009). Effect of supplementation of tulsi and neem leaves on blood glucose and lipid profile in diabetic patients. — PubMed
- Devra DK et al. (2012). Effect of tulsi on metabolic syndrome. Indian Journal of Clinical Practice. — PubMed
- Hannan JMA et al. (2006). Ocimum sanctum leaf extracts stimulate insulin secretion from perfused pancreas, isolated islets and clonal pancreatic beta-cells. Journal of Endocrinology. — PubMed
- Patil R et al. (2011). Isolation and characterization of antidiabetic component from Ocimum sanctum. Indian Journal of Pharmaceutical Sciences. — PubMed
- Bhattacharyya P et al. (2014). Tulsi: A review on bioactive constituents and antidiabetic mechanisms. International Journal of Pharma Bio Sciences. — PubMed
- Jamshidi N, Cohen MM (2017). The clinical efficacy and safety of tulsi in humans: a systematic review of the literature. Evidence-Based Complementary and Alternative Medicine. — PubMed
- Sundaram RS et al. (2013). Ursolic acid as a natural insulin sensitizer. Phytotherapy Research. — PubMed
PubMed Topic Searches
- PubMed: Ocimum sanctum diabetes RCT
- PubMed: Tulsi fasting glucose
- PubMed: Ursolic acid AMPK insulin
- PubMed: Holy basil HbA1c
- PubMed: Ocimum beta-cell protection
Connections
- Holy Basil Overview
- Holy Basil Benefits Hub
- Holy Basil for Stress
- Holy Basil for Immune Function
- Holy Basil for Respiratory Health
- Diabetes
- Blood Sugar
- Coffee and Type 2 Diabetes
- Turmeric
- Ginger
- Neem
- Oxidative Stress
- Fasting
- Continuous Glucose Monitor
- All Herbs
- Metformin — the first-line oral diabetes drug tulsi's glucose effect is benchmarked against.