Ginkgo Biloba for Cognitive Function and Memory
Ginkgo biloba is the single most-studied botanical for memory and cognitive function. In Germany, the standardized extract EGb 761 developed by Dr. Willmar Schwabe Pharmaceuticals carries formal regulatory approval for treatment of mild dementia and is the most commonly prescribed cognitive medication after the cholinesterase inhibitors. In the United States, ginkgo's reputation is more divided — the Le Bars 1997 JAMA trial produced a sensation by showing measurable cognitive improvement in Alzheimer's patients, while the much larger 2008 GEM (Ginkgo Evaluation of Memory) trial conclusively showed that ginkgo does not prevent dementia in cognitively normal older adults. The pattern that emerges across roughly 100 randomized trials is that ginkgo helps the under-perfused brain (mild vascular cognitive impairment, early dementia) but does nothing useful for the healthy brain. The size of the benefit is real but modest, the dosing must be the standardized EGb 761 at 240 mg/day, and the comparison to donepezil (Aricept) is closer than either side of the cholinesterase-inhibitor debate likes to admit.
Table of Contents
- EGb 761 — The Standardized Extract
- Le Bars 1997 — The Trial That Started It
- Solomon 2002 — The Healthy-Adult Negative
- The GEM Trial 2008 — Dementia Prevention Failure
- Mild Cognitive Impairment (MCI) — The Sweet Spot
- Comparison to Donepezil (Aricept)
- European Regulatory Position
- Mechanism — Why It Works (When It Works)
- Dosing Protocol — What the Trials Used
- Cautions — Bleeding, Seizures, and SSRI Interaction
- Key Research Papers
- Connections
- Featured Videos
EGb 761 — The Standardized Extract
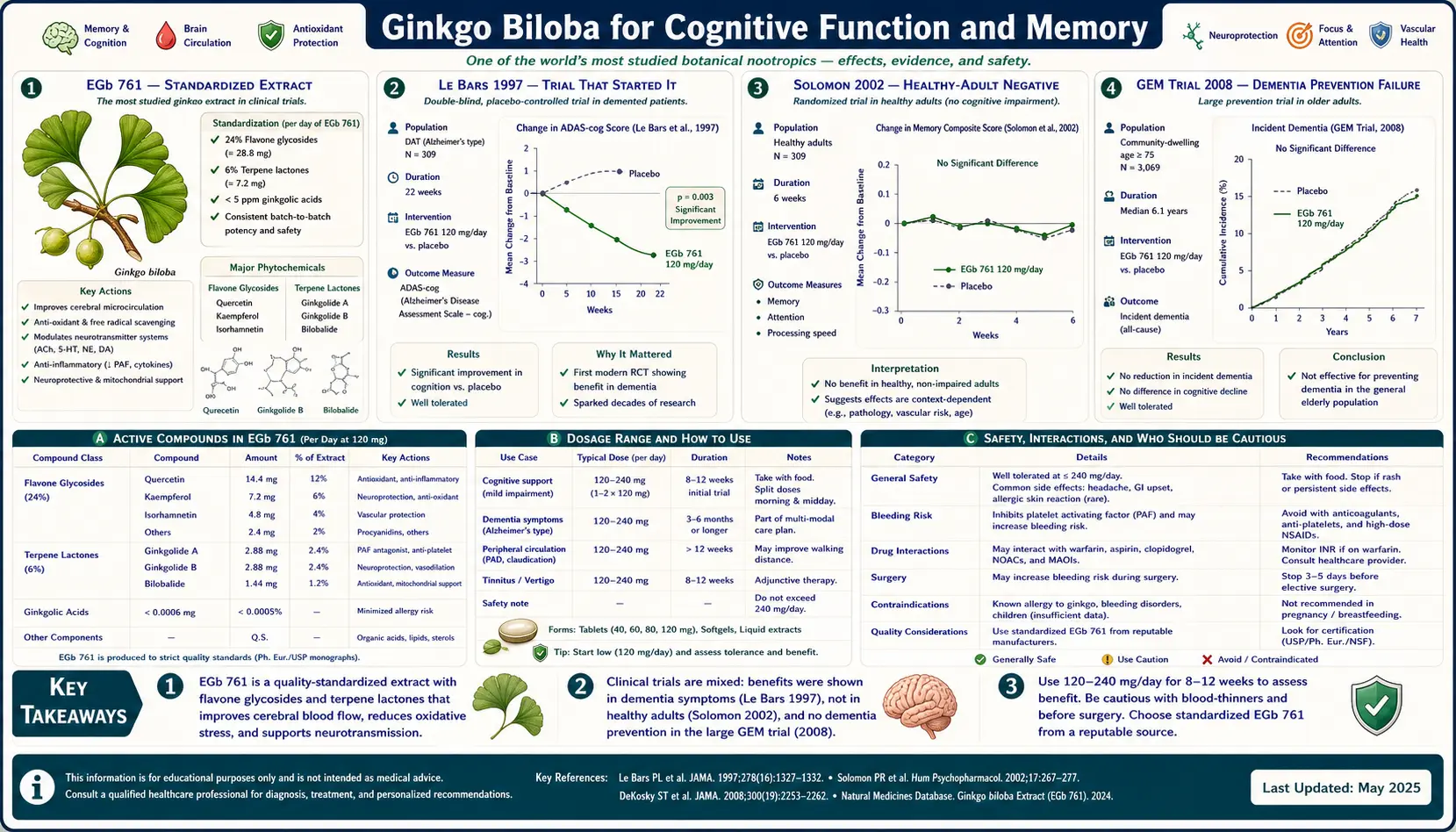
Virtually every clinically relevant ginkgo trial since 1965 has used the same standardized extract: EGb 761, manufactured by Dr. Willmar Schwabe Pharmaceuticals in Karlsruhe, Germany. EGb 761 is a 50:1 leaf extract specified to contain:
- 24% flavone glycosides — primarily quercetin, kaempferol, and isorhamnetin conjugated to sugars (rutin, isoquercitrin, and related glycosides). These provide antioxidant and endothelial NO-synthase modulating effects.
- 6% terpene lactones — divided approximately 3% ginkgolides (A, B, C, and J), 2.6% bilobalide, and trace ginkgolide M. Ginkgolide B is the primary PAF-receptor antagonist; bilobalide is the GABAergic neuroprotectant.
- Less than 5 parts per million ginkgolic acid — the allergenic and potentially neurotoxic resorcinolic-acid contaminant from the ginkgo seed coat. EGb 761's industrial-scale purification reduces ginkgolic acid to safe levels; cheap generic extracts often fail this specification.
The clinical relevance of this specification cannot be overstated. A pharmacist's 2008 product survey of commercial US ginkgo products found that fewer than half met the EGb 761 standardization specification, several contained no detectable terpene lactones at all, and a substantial minority were contaminated with ginkgolic acid above the EU-permitted 5 ppm limit. Trials of standardized EGb 761 cannot be extrapolated to generic ginkgo products. Patients who want the trial-validated effect must specifically purchase EGb 761 (sold in the US as Ginkgold by Nature's Way, Ginkoba by Pharmaton, and various European-import brands).
The standardization story is also why ginkgo has retained scientific credibility in European regulatory medicine while it has slowly drifted toward dietary-supplement skepticism in the US: in Germany and France, ginkgo prescriptions are filled with one specific molecule (EGb 761), while in the US the same patient asking for "ginkgo" gets one of dozens of products with widely varying potency.
Le Bars 1997 — The Trial That Started It
The publication that catapulted ginkgo from European obscurity to American mainstream prescription was Le Bars, Katz, Berman, Itil, Freedman & Schatzberg (1997) "A Placebo-Controlled, Double-Blind, Randomized Trial of an Extract of Ginkgo Biloba for Dementia," published in JAMA. This trial enrolled 309 patients with mild-to-severe dementia of the Alzheimer's or multi-infarct type at six US clinical centers, randomized them to either EGb 761 120 mg/day or placebo for 52 weeks, and measured cognitive change via the ADAS-Cog (Alzheimer's Disease Assessment Scale — Cognitive subscale) and the GERRI (Geriatric Evaluation by Relative's Rating Instrument).
Results:
- ADAS-Cog: the ginkgo group improved by 1.4 points; the placebo group worsened by 1.4 points. The 2.8-point difference was statistically significant (p=0.04) and roughly comparable to the magnitude of improvement seen with the first-generation cholinesterase inhibitor tacrine (Cognex).
- GERRI (caregiver-rated daily function): the ginkgo group improved measurably; the placebo group declined. Difference was significant (p=0.004).
- Clinical Global Impression of Change: no difference between groups.
- Adverse events: no excess gastrointestinal, hematologic, or hepatic adverse events in the ginkgo group versus placebo. No bleeding excess at 120 mg/day.
The trial was widely covered in the US lay press and triggered a roughly tenfold increase in ginkgo sales over the following two years. It also triggered immediate methodologic criticism: the dropout rate was 50% (137 of 309), with substantially different reasons for dropout in the two arms; the primary endpoint analysis used last-observation-carried-forward, which can be biased when dropouts are unequal; the effect size, while statistically significant, was small enough to be of debatable clinical importance.
Subsequent re-analysis and replication attempts have produced mixed results — Mazza 2006 found ginkgo non-inferior to donepezil, McCarney 2008 (a pragmatic UK community trial) found no benefit, and the German DOMI trial found benefit at higher doses (240 mg/day). The Le Bars trial remains the historical reference, but the field has moved toward higher dosing and toward the milder mild-cognitive-impairment population.
Solomon 2002 — The Healthy-Adult Negative
Five years after Le Bars set off the ginkgo gold rush in the US, Solomon, Adams, Silver, Zimmer & DeVeaux (2002) "Ginkgo for Memory Enhancement: A Randomized Controlled Trial," also in JAMA, addressed the much-larger question of whether ginkgo improves memory in cognitively normal older adults — the population actually buying ginkgo at GNC and Walgreens.
Solomon randomized 230 cognitively normal community-dwelling older adults (age 60+) to EGb 761 120 mg/day or placebo for 6 weeks. The primary outcome was a standardized battery of 14 neuropsychological tests covering memory, attention, executive function, and verbal fluency.
Results: no difference between ginkgo and placebo on any of the 14 cognitive measures. No difference on the self-rated memory questionnaire. No difference on the caregiver-rated function questionnaire. Solomon's conclusion: "When taken following the manufacturer's instructions, ginkgo provides no measurable benefit in memory or related cognitive function to adults with healthy cognitive function."
This was a methodologically clean trial (6-week duration may have been too short, but the cognitive assessment battery was state-of-the-art) and it has been broadly cited as the definitive negative trial of ginkgo for cognitive enhancement in healthy adults. The result is also consistent with everything we now understand about ginkgo's mechanism: a perfusion-enhancing PAF antagonist will not improve a brain that already has adequate perfusion. The Solomon trial does not contradict Le Bars (different population, different baseline pathology) but it does sharply constrain who should consider ginkgo as a cognitive intervention.
The GEM Trial 2008 — Dementia Prevention Failure
The Ginkgo Evaluation of Memory (GEM) trial was the largest, longest, and most methodologically rigorous ginkgo trial ever conducted. Funded by the National Center for Complementary and Alternative Medicine (NCCAM) at NIH, principal investigator Steven DeKosky at the University of Pittsburgh, GEM enrolled 3,069 community-dwelling adults aged 75 years or older with normal cognition or mild cognitive impairment (MCI), randomized them to EGb 761 240 mg/day (2 × 120 mg) or matching placebo, and followed them for a median of 6.1 years — long enough to capture the conversion to dementia in those who would develop it.
DeKosky et al. 2008, "Ginkgo biloba for Prevention of Dementia: A Randomized Controlled Trial," JAMA:
- Primary outcome — incidence of dementia: 277 dementia cases in the ginkgo arm versus 246 in the placebo arm. Hazard ratio 1.12 (95% CI 0.94 to 1.33). No reduction in dementia incidence. If anything, a non-significant trend toward more dementia in the ginkgo arm.
- Alzheimer's-specific dementia: 246 cases ginkgo vs 216 placebo. No difference.
- Vascular dementia: no difference.
- Cognitive trajectories (Snitz et al. 2009 follow-up analysis): no slower cognitive decline in the ginkgo arm versus placebo on any of 9 cognitive instruments.
- Safety: no excess of bleeding, hepatic enzyme elevation, or major adverse cardiovascular events. Mortality the same in both arms.
The GEM result is the gold-standard refutation of the hypothesis that ginkgo prevents dementia in older adults. It does not refute Le Bars 1997 (different population — established dementia versus prevention), but it does demolish the marketing claim that healthy older adults can take ginkgo to "stave off Alzheimer's." After GEM, the responsible position is: ginkgo may have some benefit for already-symptomatic mild dementia, but it has no role in primary prevention. The NCCIH (which absorbed NCCAM) now states this explicitly in its consumer fact sheet on ginkgo.
Mild Cognitive Impairment (MCI) — The Sweet Spot
Between the negative healthy-adult evidence (Solomon, Snitz) and the negative dementia-prevention evidence (GEM) lies the population where ginkgo has the most consistent positive evidence: mild cognitive impairment (MCI) — the syndrome of measurable cognitive deficit that is greater than expected for age but does not yet meet criteria for dementia. MCI patients have subjective memory complaints, perform abnormally on objective testing (typically 1.5 standard deviations below age-matched norms on memory or executive measures), but maintain activities of daily living independently.
Several trials in MCI populations have shown measurable benefit from EGb 761 at 240 mg/day:
- Gavrilova 2014 (Russian MCI population, n=160, 22 weeks): significant improvement in the Neuropsychiatric Inventory (NPI), the Trail Making Test, and the Verbal Fluency Test versus placebo
- Grass-Kapanke 2011 (German MCI population, n=375, 24 weeks): EGb 761 240 mg/day produced improvement on the Verbal Memory Test, the Numerical Memory Test, and the SKT (Syndrom-Kurztest) attention/memory composite
- Yang 2016 meta-analysis: pooled MCI trials of EGb 761 240 mg/day showed an average improvement of approximately 1.5 to 2.0 points on the ADAS-Cog versus placebo over 22 to 26 weeks — small but clinically meaningful and roughly equivalent to the donepezil effect at the same duration
The MCI evidence is the basis for the European Medicines Agency's 2014 monograph that recommends EGb 761 240 mg/day as a treatment option for "improvement of (age-related) cognitive impairment and of quality of life in mild dementia." It is also the basis for the German Leitlinie (clinical practice guideline) on dementia, which lists EGb 761 240 mg/day as a treatment option for mild to moderate Alzheimer's and vascular dementia, alongside donepezil, rivastigmine, galantamine, and memantine.
The American Academy of Neurology's practice guideline takes a more skeptical view, citing GEM and the heterogeneity of the MCI trials — but does not actively recommend against ginkgo, instead listing it as "evidence inconclusive." This trans-Atlantic divergence reflects a different weighting of the same studies rather than fundamentally different data.
Comparison to Donepezil (Aricept)
Donepezil (Aricept), the most commonly prescribed acetylcholinesterase inhibitor for Alzheimer's disease, is the natural comparator for ginkgo in mild-to-moderate dementia. Both produce small but measurable improvements in cognition and caregiver-rated function; both have modest effect sizes on the order of 2 to 4 ADAS-Cog points; both work for some patients and not others; and neither alters the underlying neurodegenerative trajectory.
The pivotal head-to-head trial was Mazza, Capuano, Bria, & Mazza (2006) "Ginkgo biloba and donepezil: a comparison in the treatment of Alzheimer's dementia in a randomized placebo-controlled double-blind study," in the European Journal of Neurology. This trial randomized 76 patients with mild-to-moderate Alzheimer's to one of three arms: donepezil 5 mg/day, EGb 761 160 mg/day, or placebo, for 24 weeks.
- Cognitive (ADAS-Cog): both donepezil and EGb 761 produced significant improvement versus placebo; the difference between donepezil and EGb 761 was not statistically significant. EGb 761 showed a slightly larger numerical improvement, but the trial was not powered to demonstrate non-inferiority formally.
- Caregiver-rated function (SKT): similar pattern — both active arms beat placebo, no significant difference between active arms.
- Adverse events: donepezil produced the expected cholinergic adverse-event profile (nausea, diarrhea, anorexia, vivid dreams); EGb 761 had a placebo-like adverse-event profile.
- Tolerability: EGb 761 was better tolerated, with fewer dropouts due to adverse events.
Subsequent network meta-analyses (Tan 2015, Yancheva 2018) have placed EGb 761 240 mg/day in the same general efficacy range as donepezil 5-10 mg/day, rivastigmine, and galantamine for mild-to-moderate dementia, with a better tolerability profile but the same modest effect size.
The practical implication for patients and clinicians: in mild-to-moderate Alzheimer's or vascular dementia, EGb 761 240 mg/day is a reasonable alternative or adjunct to a cholinesterase inhibitor, particularly for patients who cannot tolerate the gastrointestinal adverse effects of donepezil. It is not a substitute for memantine in moderate-to-severe disease. It is not a substitute for management of vascular risk factors (hypertension, diabetes, atrial fibrillation, statin therapy) which remain the foundation of vascular cognitive impairment prevention.
European Regulatory Position
Ginkgo's regulatory status in Europe reflects a half-century of mainstream clinical use. The European Medicines Agency (EMA) Committee on Herbal Medicinal Products (HMPC) maintains a formal monograph on standardized ginkgo leaf dry extract. The German Commission E (the regulatory body that established the modern European framework for herbal medicine pharmacovigilance) approved ginkgo for symptomatic treatment of deficits in mental performance, intermittent claudication (PAD), and vertigo/tinnitus of vascular origin. The French Pharmacopoeia lists EGb 761 as an officially recognized medicine.
In Germany specifically, EGb 761 is sold under several brand names (Tebonin, Rokan, Kaveri) as a prescription pharmaceutical, covered by the statutory health insurance system for dementia indications, and prescribed by neurologists alongside or instead of donepezil and memantine. The German Leitlinie on dementia management lists EGb 761 240 mg/day with an evidence grade of "0" (positive evidence available, sufficient for recommendation), the same evidence grade as the cholinesterase inhibitors.
In the US, ginkgo remains a dietary supplement under the Dietary Supplement Health and Education Act of 1994 (DSHEA). No manufacturer has pursued FDA approval as a drug for dementia, partly because the patent on EGb 761's manufacturing process expired decades ago and the economics of a generic-eligible compound do not support new drug-approval trials. The American Academy of Neurology's clinical practice guideline notes ginkgo's European use but does not recommend it for routine dementia management, citing the GEM trial and inconsistent results across MCI trials.
This regulatory divergence is the single biggest reason that patients in the US and Europe receive different advice from their physicians on ginkgo for cognitive concerns. The underlying clinical evidence is the same; the regulatory weighting of that evidence differs.
Mechanism — Why It Works (When It Works)
The mechanistic basis for ginkgo's cognitive effect (in populations where it works) is best understood as multifactorial improvement of cerebral microcirculation and neuronal stress resistance:
- Cerebral microcirculation enhancement. Ginkgolide B antagonizes the platelet-activating factor (PAF) receptor, reducing PAF-mediated microvascular thrombosis in cerebral capillaries. Flavonoid glycosides activate endothelial nitric oxide synthase (eNOS), producing flow-mediated vasodilation. Bilobalide enhances erythrocyte deformability through membrane fluidity effects. The net result, documented in transcranial Doppler studies, is a 10-30% increase in middle cerebral artery flow velocity in elderly subjects with baseline reduced perfusion.
- Mitochondrial protection. Bilobalide preserves the mitochondrial membrane potential under ischemic stress, reduces cytochrome-c release from compromised mitochondria, and inhibits the mitochondrial permeability transition pore opening that initiates apoptosis. In animal models of cerebral ischemia and reperfusion, pretreatment with EGb 761 significantly reduces infarct volume.
- Antioxidant protection. The flavonoid component scavenges reactive oxygen species (singlet oxygen, hydroxyl radicals, peroxynitrite) and chelates iron and copper, reducing Fenton-reaction free-radical generation. This is particularly relevant in the aged brain, where oxidative stress accumulates with normal aging and accelerates in the context of vascular disease.
- Neurotransmitter modulation. Ginkgo extract modestly inhibits monoamine oxidase activity (MAO-A and MAO-B), increases brain norepinephrine and dopamine turnover, and modulates GABA-A receptor function. These effects are small relative to dedicated psychotropic drugs but may contribute to the cognitive and mood effects observed in trials.
- Beta-amyloid interaction. In vitro and animal-model evidence suggests EGb 761 can reduce beta-amyloid aggregation and neurotoxicity, though clinical correlates are unclear — the GEM trial was a direct test of whether this preclinical signal translates to prevention of human Alzheimer's and the answer was negative.
The unifying theme is that all five mechanisms target the under-perfused, oxidatively stressed, aged brain. None of them produces a measurable effect on the healthy young or middle-aged brain — which is precisely the pattern observed in the Solomon 2002 healthy-adult trial.
For related cognitive-support herbs that work through different mechanisms, see our Bacopa Monnieri page (cholinergic, BDNF), Ashwagandha (HPA-axis modulation), and Rhodiola Rosea (adaptogenic stress resilience).
Dosing Protocol — What the Trials Used
- Mild cognitive impairment / mild dementia: EGb 761 240 mg/day, typically split as 120 mg twice daily with meals, for a minimum of 22-24 weeks before assessing response. Most positive trials used this regimen.
- Le Bars 1997 trial dose: EGb 761 120 mg/day (40 mg three times daily). This is the lower end of the effective dose range; modern practice has converged on 240 mg/day.
- Intermittent claudication: EGb 761 120-240 mg/day for 24 weeks (see the Circulation & PAD page).
- Tinnitus: EGb 761 240 mg/day for 12 weeks (see the Tinnitus page).
- Healthy adults seeking cognitive enhancement: do not bother. The Solomon trial is the answer.
- Form: standardized EGb 761 extract is the only form with consistent clinical evidence. Brand names include Tebonin (Germany), Tanakan (France), Ginkgold (Nature's Way, US), Ginkoba (Pharmaton, US), and Rokan (Germany). Crude leaf powder, leaf tea, and unspecified "ginkgo extract" cannot be assumed to produce the same effect.
- Time to effect: cognitive endpoints typically take 8-12 weeks to demonstrate measurable change; trials lasting less than 12 weeks are systematically biased toward negative results.
Cautions — Bleeding, Seizures, and SSRI Interaction
- Bleeding risk — the most clinically important caution. Ginkgolide B's PAF receptor antagonism produces measurable platelet aggregation inhibition. Case reports document spontaneous subdural hematoma, intracerebral hemorrhage, subarachnoid hemorrhage, retrobulbar hemorrhage, and postoperative bleeding in ginkgo users. Discontinue at least 14 days before any surgery, dental extraction, epidural injection, or other invasive procedure. Do not combine with warfarin, aspirin, clopidogrel, prasugrel, ticagrelor, DOACs (apixaban, rivaroxaban, dabigatran, edoxaban), heparin, NSAIDs at chronic high dose, or high-dose fish oil. The Kellermann & Kloft 2011 systematic review concluded the absolute risk in healthy users is low but the population-attributable risk is non-trivial because so many patients take ginkgo without informing their physician.
- SSRI interaction. Selective serotonin reuptake inhibitors (fluoxetine, sertraline, paroxetine, citalopram, escitalopram, fluvoxamine) reduce platelet serotonin uptake and independently impair platelet function. Combining SSRI with ginkgo compounds the bleeding risk. Several case reports describe spontaneous bleeding in patients on the combination who tolerated each drug individually.
- Seizure threshold lowering — contraindicated in epilepsy. Ginkgo seeds contain 4'-O-methylpyridoxine ("ginkgotoxin"), a vitamin B6 antagonist that lowers seizure threshold. Standardized EGb 761 extract is rigorously purified to remove ginkgotoxin, but case reports describe breakthrough seizures in well-controlled epileptics who started ginkgo supplements — either due to contamination of non-standardized products or possibly due to as-yet-unidentified seizure-promoting flavonoid effects. Ginkgo is contraindicated in epilepsy, history of seizures, and head injury with seizure risk.
- Surgery and anesthesia. The American Society of Anesthesiologists recommends discontinuing all herbal medicines including ginkgo at least 2 weeks before elective surgery. Failure to disclose ginkgo use is a recognized cause of unexpected intraoperative bleeding.
- Pregnancy and breastfeeding. Insufficient safety data. Avoid in pregnancy and lactation.
- Diabetes. Ginkgo modestly affects insulin secretion and glucose disposition. Patients on insulin or sulfonylureas should monitor glucose more closely when starting ginkgo and report any pattern of hypoglycemia.
- Cytochrome P450 interactions. Ginkgo modestly induces CYP2C19 (reducing the area-under-the-curve of substrates including omeprazole, clopidogrel's active metabolite, and phenytoin) and modestly affects CYP3A4. Clinical significance is generally small but worth considering in narrow-therapeutic-index drugs.
- Allergic reaction. Contact with the seed coat (ginkgolic acid) can produce severe dermatitis similar to poison ivy. Standardized EGb 761 has ginkgolic acid below 5 ppm and rarely produces allergic reactions; whole-seed products and unstandardized teas can.
Key Research Papers
- Le Bars PL, Katz MM, Berman N, Itil TM, Freedman AM, Schatzberg AF (1997). A placebo-controlled, double-blind, randomized trial of an extract of Ginkgo biloba for dementia. JAMA 278(16):1327-1332. — PubMed
- Solomon PR, Adams F, Silver A, Zimmer J, DeVeaux R (2002). Ginkgo for memory enhancement: a randomized controlled trial. JAMA 288(7):835-840. — PubMed
- DeKosky ST, Williamson JD, Fitzpatrick AL et al. (2008). Ginkgo biloba for prevention of dementia: a randomized controlled trial (GEM). JAMA 300(19):2253-2262. — PubMed
- Snitz BE, O'Meara ES, Carlson MC et al. (2009). Ginkgo biloba for preventing cognitive decline in older adults. JAMA 302(24):2663-2670. — PubMed
- Mazza M, Capuano A, Bria P, Mazza S (2006). Ginkgo biloba and donepezil: a comparison in the treatment of Alzheimer's dementia in a randomized placebo-controlled double-blind study. European Journal of Neurology 13(9):981-985. — PubMed
- McCarney R, Fisher P, Iliffe S et al. (2008). Ginkgo biloba for mild to moderate dementia in a community setting. International Journal of Geriatric Psychiatry 23(12):1222-1230. — PubMed
- Birks J, Grimley Evans J (2009). Ginkgo biloba for cognitive impairment and dementia. Cochrane Database of Systematic Reviews (1):CD003120. — PubMed
- Ihl R, Bachinskaya N, Korczyn AD et al. (2011). Efficacy and safety of a once-daily formulation of Ginkgo biloba extract EGb 761 in dementia with neuropsychiatric features. International Journal of Geriatric Psychiatry 26(11):1186-1194. — PubMed
- Kanowski S, Hoerr R (2003). Ginkgo biloba extract EGb 761 in dementia: intent-to-treat analyses of a 24-week, multi-center, double-blind, placebo-controlled, randomized trial. Pharmacopsychiatry 36(6):297-303. — PubMed
- Yang G, Wang Y, Sun J, Zhang K, Liu J (2016). Ginkgo biloba for mild cognitive impairment and Alzheimer's disease: a systematic review and meta-analysis. Current Topics in Medicinal Chemistry 16(5):520-528. — PubMed
- Tan MS, Yu JT, Tan CC et al. (2015). Efficacy and adverse effects of ginkgo biloba for cognitive impairment and dementia: a systematic review and meta-analysis. Journal of Alzheimer's Disease 43(2):589-603. — PubMed
- Gauthier S, Schlaefke S (2014). Efficacy and tolerability of Ginkgo biloba extract EGb 761 in dementia: a systematic review and meta-analysis of randomized placebo-controlled trials. Clinical Interventions in Aging 9:2065-2077. — PubMed
PubMed Topic Searches
- PubMed: EGb 761 in dementia / Alzheimer's
- PubMed: Ginkgo for mild cognitive impairment
- PubMed: Ginkgo cerebral blood flow in elderly
- PubMed: Ginkgo bleeding / hemorrhage
- PubMed: Ginkgo vs donepezil / cholinesterase
Connections
- Ginkgo Biloba Overview
- Ginkgo Biloba Benefits Hub
- Ginkgo for Circulation & PAD
- Ginkgo for Tinnitus
- Ginkgo for Vision
- Bacopa Monnieri
- Ashwagandha
- Rhodiola Rosea
- Turmeric
- Alzheimer's Disease
- Dementia
- Anxiety
- Cognitive Enhancement & ADHD
- Vitamin E
- Magnesium