Ginkgo Biloba for Circulation and Peripheral Artery Disease
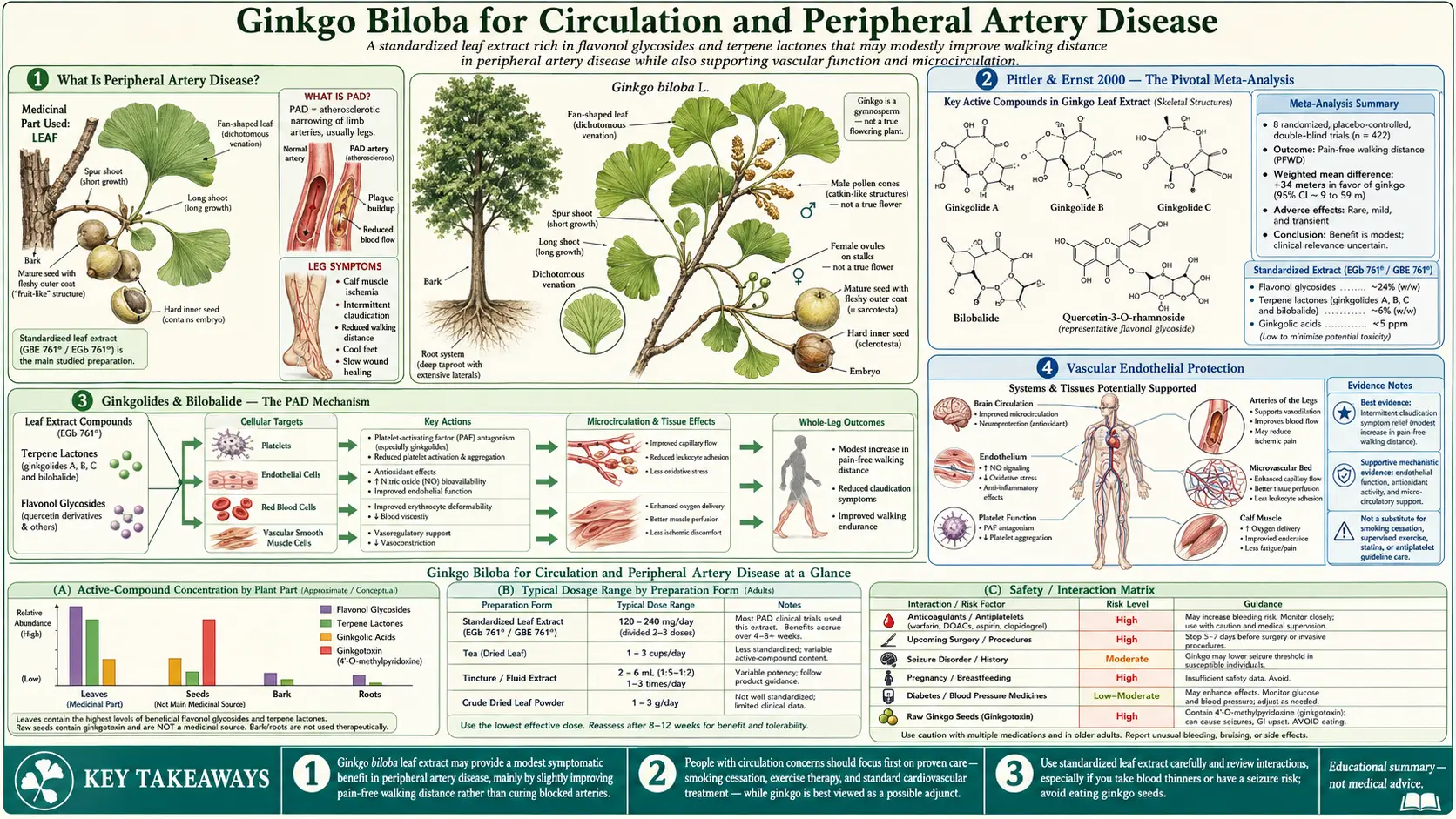
Peripheral artery disease (PAD) — the chronic narrowing of arteries supplying the legs — affects an estimated 8 to 12 million Americans and produces the disabling symptom of intermittent claudication: cramping leg pain that begins after walking a predictable distance and resolves with rest. Ginkgo biloba's most rigorously validated cardiovascular benefit is in this condition. The Pittler & Ernst 2000 American Journal of Medicine meta-analysis pooled 8 randomized placebo-controlled trials and concluded that EGb 761 120-160 mg/day produces a statistically significant and clinically meaningful increase in pain-free walking distance of approximately 34 meters — comparable in magnitude to the only two FDA-approved drugs for the indication, pentoxifylline (Trental) and cilostazol (Pletal). The underlying mechanism — PAF antagonism by ginkgolide B, flavonoid-mediated endothelial nitric oxide signaling, and improved erythrocyte deformability — is the same multifactorial microcirculation improvement that explains ginkgo's effects on cerebral, cochlear, and retinal blood flow. Understanding the PAD evidence is the key to understanding why ginkgo helps the under-perfused brain in mild cognitive impairment but does nothing for the healthy young brain.
Table of Contents
- What Is Peripheral Artery Disease?
- Pittler & Ernst 2000 — The Pivotal Meta-Analysis
- Ginkgolides & Bilobalide — The PAD Mechanism
- Vascular Endothelial Protection
- Walking-Distance Trials in Detail
- Comparison with Pentoxifylline and Cilostazol
- The Cochrane 2013 Update — Weakening Confidence
- Cerebral Microcirculation — The Cognitive Link
- Raynaud's, Vertigo, and Erectile Dysfunction
- Cautions — Bleeding and Antiplatelet Stacking
- Key Research Papers
- Connections
- Featured Videos
What Is Peripheral Artery Disease?
Peripheral artery disease (PAD) is the lower-extremity manifestation of the same systemic atherosclerotic process that produces coronary artery disease, carotid stenosis, and stroke. Plaque accumulates in the arteries supplying the legs — most commonly the superficial femoral, popliteal, and tibial arteries — progressively narrowing the lumen and reducing blood flow to the calf and foot muscles during exertion.
The dominant symptom is intermittent claudication — from the Latin claudicare, "to limp." The patient walks a predictable distance (typically 50-300 meters on flat ground), develops a cramping, aching, or burning pain in one or both calves, must stop and rest, the pain resolves over 2-5 minutes, and the cycle can be repeated. As disease advances, the pain-free walking distance shrinks. In advanced PAD, the patient develops rest pain (constant aching in the foot, worse at night when supine), non-healing ulcers, gangrene, and ultimately limb loss.
The Fontaine classification stages PAD: Stage I (asymptomatic but objectively reduced ABI), Stage IIa (claudication at >200 m), Stage IIb (claudication at <200 m, the population in most ginkgo trials), Stage III (rest pain), and Stage IV (tissue loss). The Rutherford classification is the parallel North American system.
Standard medical therapy includes statin therapy (improves walking distance independently), aggressive smoking cessation (the strongest risk factor), antiplatelet therapy (aspirin or clopidogrel for cardiovascular event reduction), supervised exercise training (the highest-evidence non-surgical intervention), and the two FDA-approved claudication-specific drugs:
- Cilostazol (Pletal) — a phosphodiesterase-3 inhibitor that produces vasodilation and platelet inhibition. Increases pain-free walking distance by approximately 50-65 meters in meta-analysis. Contraindicated in heart failure (FDA black-box warning).
- Pentoxifylline (Trental) — an older xanthine derivative that improves erythrocyte deformability and reduces blood viscosity. Effect size smaller than cilostazol (approximately 20-30 m walking distance increase). Generally well tolerated.
Ginkgo biloba (EGb 761 120-240 mg/day) sits in roughly the same effect-size range as pentoxifylline and below cilostazol. Its advantage is tolerability and the absence of contraindication in heart failure; its disadvantage is the antiplatelet stacking risk if combined with aspirin or clopidogrel, which is the standard therapy in PAD patients.
Pittler & Ernst 2000 — The Pivotal Meta-Analysis
The reference meta-analysis for ginkgo in PAD is Pittler MH & Ernst E (2000) "Ginkgo biloba extract for the treatment of intermittent claudication: a meta-analysis of randomized trials," published in the American Journal of Medicine. Pittler and Ernst were systematic-review specialists at the Universities of Exeter and Plymouth (UK), and Ernst was at the time the world's leading academic critic of complementary medicine — not a sympathetic source for ginkgo claims.
They identified 8 randomized, double-blind, placebo-controlled trials of ginkgo extract for intermittent claudication that met methodological inclusion criteria, comprising 415 total patients. Trial duration ranged from 24 weeks to 6 months. The primary endpoint pooled across trials was increase in pain-free walking distance on standardized treadmill testing.
The pooled result: ginkgo extract produced a statistically significant increase in pain-free walking distance of 34 meters (95% confidence interval 26-43 m) compared to placebo. The effect was modest but consistent across trials and clinically meaningful — a 34-meter improvement converts a patient from "I can't make it to the mailbox" to "I can make it to the mailbox," or from one block to two blocks.
The authors' conclusion: "Ginkgo biloba extract is superior to placebo in the symptomatic treatment of intermittent claudication. However, the size of the overall treatment effect is modest and of uncertain clinical relevance." This was, characteristically for Ernst, a guarded conclusion — but importantly, it confirmed a real biological effect in a condition with an objective endpoint (treadmill walking distance) that is not susceptible to placebo response.
The Pittler & Ernst 2000 meta-analysis was the highest-quality evidence available at the time and remains the most-cited reference for ginkgo's vascular effects. Subsequent trials and the Cochrane 2013 update have somewhat attenuated the effect estimate, but the direction of effect is consistent.
Ginkgolides & Bilobalide — The PAD Mechanism
The pharmacological basis for ginkgo's PAD efficacy is one of the most elegantly worked out in herbal medicine, in large part because the German Schwabe research program invested heavily in pre-clinical characterization to support European drug-approval requirements. The mechanism has three independent but complementary components:
1. Ginkgolide B and platelet-activating factor (PAF) antagonism
Platelet-activating factor is a phospholipid mediator (1-O-alkyl-2-acetyl-sn-glycero-3-phosphocholine) produced by activated leukocytes, platelets, mast cells, and vascular endothelium. PAF binds to a specific G-protein-coupled receptor (PAFR) on platelets to trigger aggregation, on leukocytes to drive chemotaxis and adhesion, and on smooth muscle to produce bronchoconstriction. In the microcirculation, PAF-mediated leukocyte adhesion and platelet aggregation produce capillary plugging, which reduces effective tissue perfusion below what the apparent angiographic anatomy would predict.
Ginkgolide B is one of the most potent natural PAF receptor antagonists ever characterized. At clinically relevant plasma concentrations, ginkgolide B competitively blocks PAF binding to PAFR with an IC50 in the low micromolar range. The downstream consequence in the leg muscle microcirculation: less PAF-mediated leukocyte adhesion to capillary endothelium, less platelet aggregation in micro-thrombi, less capillary plugging, more effective perfusion per unit of bulk arterial blood flow.
2. Flavonoid-mediated endothelial nitric oxide signaling
The quercetin, kaempferol, and isorhamnetin glycoside fraction of EGb 761 modulates endothelial nitric oxide synthase (eNOS). The mechanism appears to involve both reduced eNOS uncoupling under oxidative stress (preserving NO production in the face of superoxide) and direct upregulation of eNOS expression. The net result is improved flow-mediated vasodilation in the limb arterioles, measurable as increased post-occlusion brachial artery diameter on ultrasound after EGb 761 administration.
3. Bilobalide and erythrocyte deformability
Bilobalide modestly enhances the deformability of red blood cells — the capacity of the biconcave erythrocyte to fold and squeeze through capillaries of smaller diameter than the cell itself. In aged and atherosclerotic patients, baseline erythrocyte deformability is reduced (membrane stiffening due to oxidative damage, glycation, and lipid composition changes), which contributes to functional microcirculatory failure independent of macroscopic vessel stenosis. Bilobalide partially restores deformability, allowing more efficient passage of red cells through narrowed capillary beds.
The integrated effect of all three mechanisms is improved tissue oxygen delivery for any given level of bulk arterial flow, which is exactly what the TcPO2 (transcutaneous oxygen tension) studies of EGb 761 have documented — Mouren et al. 1994 measured increased TcPO2 in the lower extremities of PAD patients after EGb 761 administration, confirming the mechanistic prediction.
Vascular Endothelial Protection
Beyond the acute microcirculatory effects, EGb 761 produces chronic protective effects on vascular endothelium that may slow PAD progression independent of its symptomatic walking-distance benefit. Mechanistic studies in cultured human endothelial cells and animal models of atherosclerosis have shown:
- Reduced expression of endothelial adhesion molecules VCAM-1, ICAM-1, and E-selectin under inflammatory stimulation, reducing leukocyte adhesion and infiltration that drives atherosclerotic plaque progression
- Inhibition of LDL oxidation by the flavonoid antioxidant component, reducing the foam-cell-forming oxidized LDL that drives early atherogenesis
- Preservation of endothelial barrier function under oxidative stress, reducing the endothelial leak that contributes to plaque inflammation
- Reduced platelet-endothelial adhesion via PAF antagonism, which is a precursor step in both thrombosis and chronic inflammatory plaque progression
- Modulation of vascular smooth muscle cell proliferation, the cellular event that drives intimal hyperplasia after vascular injury
Whether these mechanistic effects translate to slowed clinical PAD progression in humans remains unclear — no large, long-duration trial has evaluated EGb 761 as primary PAD prevention or progression-modifying therapy. The existing PAD trials are uniformly symptomatic-improvement trials of 12-26 week duration. The case for ginkgo as a vascular-disease-modifying agent remains preclinical.
Walking-Distance Trials in Detail
The individual trials included in the Pittler & Ernst meta-analysis varied in dose, duration, and population, which is part of why the pooled effect estimate has wide confidence intervals. The most methodologically informative individual trials:
- Peters et al. 1998 (Germany, n=111, 24 weeks, EGb 761 160 mg/day) — mean pain-free walking distance increased by 45 m in ginkgo arm vs 21 m in placebo arm. Maximum walking distance also improved more in the ginkgo arm.
- Bauer 1984 (Germany, n=79, 24 weeks, EGb 761 120 mg/day) — foundational early trial. Demonstrated significant walking-distance improvement with EGb 761 versus placebo, and was one of the studies that secured German Commission E approval for the indication.
- Blume et al. 1996 (Germany, n=60, 24 weeks, EGb 761 160 mg/day vs 120 mg/day) — head-to-head dose comparison showing the higher 160 mg/day dose produced larger walking-distance improvement.
- Schweizer & Hautmann 1999 (Germany, n=74, 24 weeks, EGb 761 240 mg/day vs 120 mg/day) — further dose-response confirmation, with the 240 mg/day arm showing approximately twice the walking-distance improvement of the 120 mg/day arm.
- Mouren et al. 1994 (France, n=20, 8 weeks, EGb 761 320 mg/day, TcPO2 primary endpoint) — mechanistic trial documenting increased transcutaneous oxygen tension in the lower extremity with EGb 761, confirming the microcirculatory mechanism.
The consistent dose-response signal across these trials suggests that 240 mg/day is a more clinically appropriate dose for PAD than the 120 mg/day used in the Le Bars dementia trial. Modern European practice has converged on 240 mg/day for vascular indications, typically split as 120 mg twice daily with meals.
Comparison with Pentoxifylline and Cilostazol
A practical question for clinicians is how EGb 761 compares to the two FDA-approved claudication-specific pharmacotherapies, pentoxifylline (Trental) and cilostazol (Pletal). The available evidence is indirect (no large head-to-head trial against pentoxifylline; no head-to-head against cilostazol at all), but the pooled effect-size estimates allow a rough comparison:
- Cilostazol 100 mg twice daily: pooled mean improvement in pain-free walking distance approximately 50-65 m vs placebo (CASTLE registry; Strandness 2002 meta-analysis). The largest evidence base. FDA-approved. Contraindicated in heart failure (black-box warning — oral phosphodiesterase-3 inhibitors increase mortality in heart failure).
- Pentoxifylline 400 mg three times daily: pooled mean improvement approximately 21-30 m vs placebo. FDA-approved but the effect size is modest enough that the 2016 AHA/ACC PAD guideline downgrades it to Class IIb (may be considered).
- EGb 761 120-240 mg/day: pooled mean improvement approximately 34 m vs placebo (Pittler 2000). Not FDA-approved. Higher doses (240 mg/day) appear to produce larger effects, potentially approaching cilostazol's effect size in the Schweizer 1999 trial.
- Supervised exercise training: the highest-evidence non-pharmacologic intervention. Pooled improvement of 150-200 m in pain-free walking distance — substantially larger than any drug. The catch: requires patient adherence to a structured 3-times-weekly walking program for at least 12 weeks. Underutilized because of patient drop-off.
The practical positioning: for a PAD patient already on optimal medical therapy (statin, aspirin, smoking cessation, supervised exercise), adding EGb 761 240 mg/day is reasonable for symptomatic improvement, with the major caveat being the antiplatelet stacking risk discussed below. The patient should be counseled that ginkgo is a modest-effect intervention, not a substitute for vascular risk factor management.
For more on PAD risk factor management, see our Peripheral Artery Disease page.
The Cochrane 2013 Update — Weakening Confidence
Nicolai et al. 2013, "Ginkgo biloba for intermittent claudication," in the Cochrane Database of Systematic Reviews, updated the Pittler & Ernst meta-analysis with the addition of newer trials and a stricter methodologic appraisal framework. The Cochrane review pooled 14 trials with 739 patients and concluded:
- The pooled effect estimate for pain-free walking distance was attenuated to approximately 10-30 m (down from Pittler & Ernst's 34 m)
- Heterogeneity across trials was substantial
- The newer (and methodologically stronger) trials showed smaller effect sizes than the older trials, raising concerns about publication bias and/or trial-quality drift
- Overall quality of evidence was rated low to moderate
- The Cochrane conclusion: "Ginkgo biloba has no statistically significant effect on the walking distance of patients with intermittent claudication when compared with placebo, based on the most recent (and methodologically stronger) studies."
This was a substantial downgrade from the Pittler & Ernst conclusion. It does not eliminate the case for ginkgo in PAD — the mechanistic plausibility remains strong, the older trials did show effect, and the heterogeneity may reflect dosing or population differences rather than pure noise — but it does suggest that the magnitude of ginkgo's PAD benefit is smaller than the early enthusiasm implied.
The honest summary for a clinician or patient: ginkgo at 240 mg/day produces a small but real improvement in claudication walking distance in some patients, comparable in magnitude to pentoxifylline. It is not a substitute for cilostazol where cilostazol is tolerated. It is a reasonable add-on to optimal medical therapy if the patient is not on antiplatelet drugs that would create a dangerous stacking interaction.
Cerebral Microcirculation — The Cognitive Link
The PAD evidence base is the mechanistic bridge to the cognitive function evidence in mild dementia. The same microcirculatory mechanisms that improve leg muscle perfusion under exertion improve cerebral perfusion in the under-perfused aged brain. Transcranial Doppler studies in elderly subjects have documented:
- 10-30% increases in middle cerebral artery flow velocity after EGb 761 administration in subjects with baseline reduced perfusion
- Improved CO2 reactivity (the vasodilatory response of cerebral arteries to hypercapnia, a marker of endothelial function) after chronic EGb 761 dosing
- Increased regional cerebral blood flow on SPECT imaging in patients with mild cognitive impairment, particularly in temporal and parietal regions that are first affected in early Alzheimer's
- No measurable change in cerebral blood flow in younger healthy subjects with already-normal perfusion (consistent with Solomon 2002's negative cognitive trial in healthy adults)
This is the unifying explanation for the otherwise puzzling pattern that ginkgo helps the elderly demented brain (Le Bars 1997, MCI trials) and the elderly claudicating leg (Pittler 2000) but does nothing for the healthy young brain (Solomon 2002). Ginkgo is fundamentally a microcirculation-rehabilitating agent in tissues that have lost adequate microcirculation. It cannot enhance perfusion above the ceiling that healthy endothelium and patent capillaries already provide.
Raynaud's, Vertigo, and Erectile Dysfunction
Ginkgo's vascular indication has been extended in clinical practice (though with thinner evidence) to several other conditions with a microcirculatory component:
- Raynaud's phenomenon — the episodic digital arteriolar vasospasm that produces white-blue-red color changes in the fingers on cold exposure or emotional stress. Several small trials have shown reduced attack frequency and severity with EGb 761 240 mg/day. Effect is modest and inconsistent. Calcium channel blockers (nifedipine) remain first-line.
- Vertigo of vascular origin — for vertigo attributable to vertebrobasilar insufficiency or labyrinthine ischemia (not for benign paroxysmal positional vertigo, Meniere's disease, or vestibular migraine), EGb 761 has been used in European practice for decades. Evidence is modest but consistent. The German Commission E formally approves EGb 761 for vertigo of vascular origin.
- Erectile dysfunction — the corpus cavernosum is fundamentally a vascular tissue, and several small trials have evaluated ginkgo for erectile dysfunction, particularly in the context of SSRI-induced sexual dysfunction. Results have been mixed; PDE-5 inhibitors (sildenafil, tadalafil) remain first-line. The combination of ginkgo plus PDE-5 inhibitor has not been well-studied and the bleeding-risk additive effect of ginkgo with the platelet inhibition that occurs with PDE-5 inhibitors is theoretically concerning.
- Diabetic microvascular complications — preliminary evidence for ginkgo in diabetic retinopathy, diabetic peripheral neuropathy, and diabetic microvascular disease in general. Mechanistically plausible. Clinically underpowered.
- Idiopathic sudden sensorineural hearing loss (SSNHL) — the parallel cochlear microcirculatory rescue indication. See the Tinnitus page for detailed discussion.
Cautions — Bleeding and Antiplatelet Stacking
- Bleeding risk in PAD patients specifically. The PAD population has a particularly concerning bleeding-risk profile for ginkgo because they are almost universally on aspirin or clopidogrel for cardiovascular event reduction. Adding ginkgo's PAF antagonism on top of an established antiplatelet drug compounds the bleeding risk. Case reports document spontaneous subdural hematoma, GI bleeding, and intracranial hemorrhage in PAD patients on aspirin who added ginkgo. Do not combine ginkgo with aspirin, clopidogrel, prasugrel, ticagrelor, or any DOAC without explicit physician supervision and an explicit risk-benefit decision.
- Surgical and procedural risk. PAD patients frequently undergo vascular procedures (angioplasty, stenting, bypass grafting, amputation). Discontinue ginkgo at least 14 days before any vascular procedure, dental extraction, or other invasive intervention. Failure to disclose ginkgo use to the surgeon is a documented cause of unexpected intra-operative and post-operative bleeding.
- Combination with cilostazol. Cilostazol independently inhibits platelet aggregation through phosphodiesterase-3 inhibition. Combining ginkgo with cilostazol is theoretically additive in bleeding risk and is not advised.
- Statin interaction. No clinically significant interaction with statins. Both can be used safely together. Ginkgo's antioxidant flavonoid effect may complement statin pleiotropy.
- Antihypertensive interaction. No clinically significant interaction, though ginkgo's mild vasodilator effect may produce modest additive blood pressure lowering. Monitor in patients with already-controlled blood pressure starting ginkgo.
- Anticoagulation in atrial fibrillation. Many PAD patients have concurrent atrial fibrillation and are anticoagulated with warfarin or a DOAC. Ginkgo is contraindicated in this population — the bleeding risk from combining ginkgo's PAF antagonism with full-dose anticoagulation is unacceptable.
- Pregnancy and breastfeeding. Insufficient safety data. PAD is rare in reproductive-age women but the caution applies.
- Allergic reaction. Standardized EGb 761 (with ginkgolic acid <5 ppm) rarely produces allergic reactions; whole-leaf or whole-seed products can produce severe contact dermatitis and oral mucositis.
Key Research Papers
- Pittler MH, Ernst E (2000). Ginkgo biloba extract for the treatment of intermittent claudication: a meta-analysis of randomized trials. American Journal of Medicine 108(4):276-281. — PubMed
- Nicolai SPA, Kruidenier LM, Bendermacher BLW et al. (2013). Ginkgo biloba for intermittent claudication. Cochrane Database of Systematic Reviews (6):CD006888. — PubMed
- Mouren X, Caillard P, Schwartz F (1994). Study of the antiischemic action of EGb 761 in the treatment of peripheral arterial occlusive disease by TcPo2 determination. Angiology 45(6 Pt 1):413-417. — PubMed
- Schweizer J, Hautmann C (1999). Comparison of two dosages of ginkgo biloba extract EGb 761 in patients with peripheral arterial occlusive disease Fontaine stage IIb. Arzneimittel-Forschung 49(11):900-904. — PubMed
- Peters H, Kieser M, Holscher U (1998). Demonstration of the efficacy of Ginkgo biloba special extract EGb 761 on intermittent claudication. VASA 27(2):106-110. — PubMed
- Blume J, Kieser M, Holscher U (1996). Placebo-controlled double-blind study of the effectiveness of Ginkgo biloba special extract EGb 761 in trained patients with intermittent claudication. VASA 25(3):265-274. — PubMed
- Smith PF, Maclennan K, Darlington CL (1996). The neuroprotective properties of the Ginkgo biloba leaf: a review of the possible relationship to platelet-activating factor (PAF). Journal of Ethnopharmacology 50(3):131-139. — PubMed
- Wu Y, Li S, Cui W, Zu X, Du J, Wang F (2008). Ginkgo biloba extract improves coronary blood flow in healthy elderly adults: role of endothelium-dependent vasodilation. Phytomedicine 15(3):164-169. — PubMed
- Mehlsen J, Drabaek H, Wiinberg N, Winther K (2002). Effects of a Ginkgo biloba extract on forearm haemodynamics in healthy volunteers. Clinical Physiology and Functional Imaging 22(6):375-378. — PubMed
- Kellermann AJ, Kloft C (2011). Is there a risk of bleeding associated with standardized Ginkgo biloba extract therapy? A systematic review and meta-analysis. Pharmacotherapy 31(5):490-502. — PubMed
- Bent S, Goldberg H, Padula A, Avins AL (2005). Spontaneous bleeding associated with Ginkgo biloba: a case report and systematic review. Journal of General Internal Medicine 20(7):657-661. — PubMed
- Bone KM (2008). Potential interaction of Ginkgo biloba leaf with antiplatelet or anticoagulant drugs. Molecular Nutrition & Food Research 52(7):764-771. — PubMed
PubMed Topic Searches
- PubMed: Ginkgo for intermittent claudication
- PubMed: Ginkgo and PAD
- PubMed: Ginkgolide PAF antagonism
- PubMed: Ginkgo endothelial / NO
- PubMed: Ginkgo microcirculation
Connections
- Ginkgo Biloba Overview
- Ginkgo Biloba Benefits Hub
- Ginkgo for Cognitive Function
- Ginkgo for Tinnitus
- Ginkgo for Vision
- Peripheral Artery Disease
- Cardiology
- All Herbs
- Turmeric
- Rosemary
- Taurine
- Vitamin E
- Magnesium
- Methylene Blue
- Stress Management