Ginkgo Biloba for Vision and Macular Degeneration
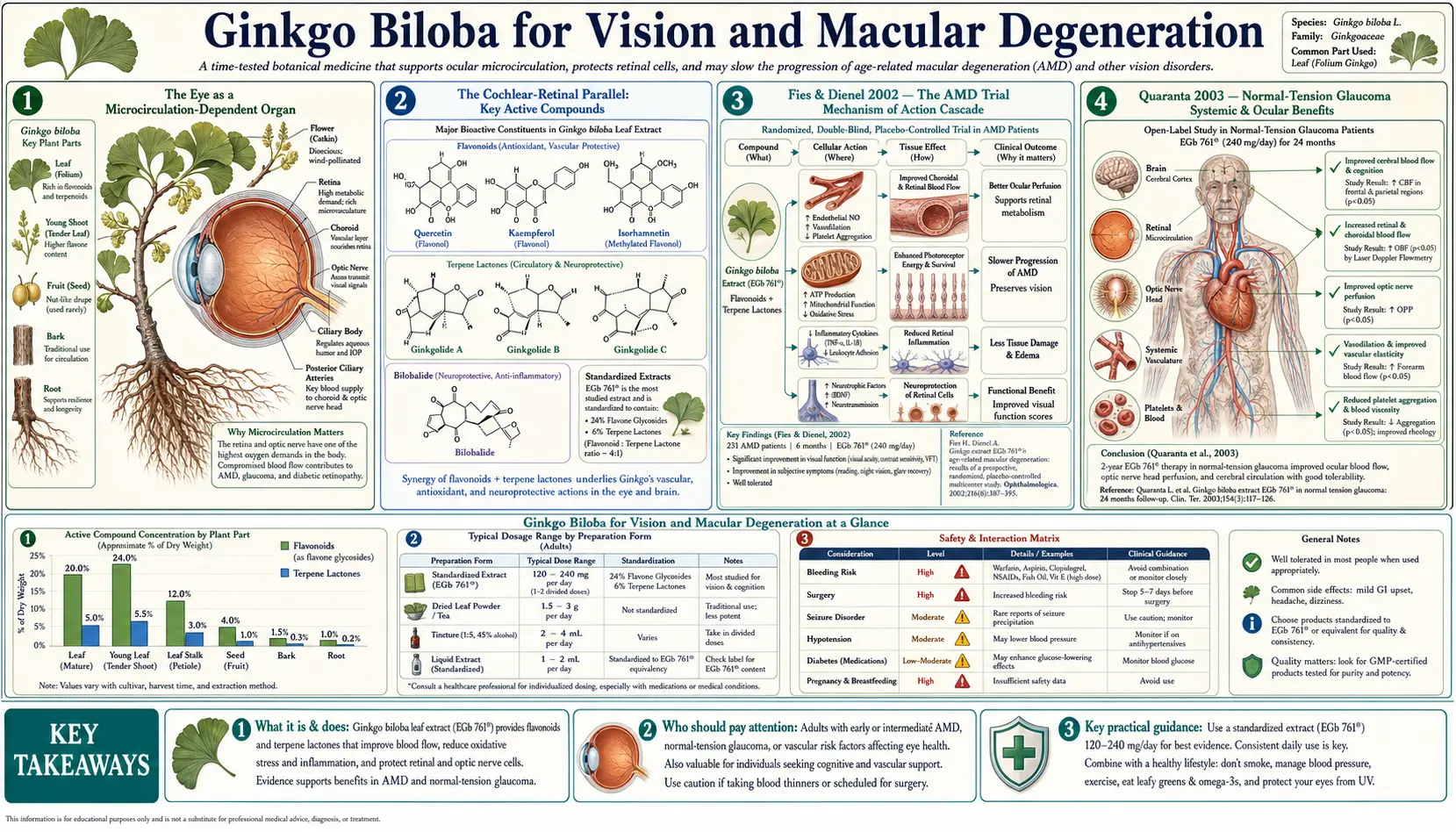
The eye, like the inner ear, is a microcirculation-dependent organ: the retina is the most metabolically active tissue in the body per unit weight, and the choroidal and retinal vessels supplying it are end-arteries with limited collateral reserve. This is the conceptual reason why ginkgo's mechanism — PAF antagonism, flavonoid antioxidant protection, and erythrocyte deformability improvement — has been hypothesized and tested in three distinct ophthalmologic conditions: normal-tension glaucoma (where the optic nerve is damaged despite normal intraocular pressure, implicating vascular insufficiency), age-related macular degeneration (where chronic choroidal microcirculatory dysfunction contributes to photoreceptor loss), and diabetic retinopathy (the classic microvascular endpoint of diabetes). The pivotal Fies & Dienel 2002 trial in dry AMD demonstrated measurable visual acuity improvement with EGb 761; the Quaranta 2003 crossover trial in normal-tension glaucoma documented visual field improvement; the cochlear-retinal microcirculation parallel ties the ophthalmologic evidence to the broader ginkgo mechanism. The evidence base is smaller and less consistent than for cognitive or PAD indications, but the mechanistic plausibility and the favorable safety profile of EGb 761 make ginkgo a reasonable adjunctive option in selected patients with ophthalmologic disease of microcirculatory origin.
Table of Contents
- The Eye as a Microcirculation-Dependent Organ
- The Cochlear-Retinal Parallel
- Fies & Dienel 2002 — The AMD Trial
- Quaranta 2003 — Normal-Tension Glaucoma
- Age-Related Macular Degeneration — Mechanism & Trials
- Glaucoma — NTG vs POAG
- Diabetic Retinopathy
- Direct Retinal Blood Flow Measurement
- The AREDS Question — Why Ginkgo Is Not in the Formula
- Dosing Protocol
- Cautions — Retrobulbar Hemorrhage and Glaucoma Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
The Eye as a Microcirculation-Dependent Organ
The retina's metabolic demand is exceptional. The outer retina (photoreceptors and retinal pigment epithelium) consumes oxygen at one of the highest rates of any tissue in the body — the photoreceptors maintain a continuous dark current that requires constant ATP supply, and the renewal of photoreceptor outer segments is one of the most metabolically demanding processes in adult cell biology. The retinal pigment epithelium phagocytizes shed outer segment discs daily, generating lipofuscin and reactive oxygen species at high rates.
This metabolic demand is supplied by two distinct vascular systems:
- The retinal vasculature — the central retinal artery and its branches supply the inner retina (ganglion cell layer, inner nuclear layer, inner plexiform layer). These vessels are visible on fundoscopy. Their dysfunction produces diabetic retinopathy, retinal vein occlusion, and the inner-retinal layer ischemia of arterial occlusive disease.
- The choroidal vasculature — a dense network of fenestrated capillaries (the choriocapillaris) supplies the outer retina (photoreceptors and retinal pigment epithelium) by diffusion across Bruch's membrane. The choroid has the highest blood flow per gram of tissue of any organ in the body. Choroidal microcirculatory dysfunction is implicated in age-related macular degeneration.
The optic nerve has its own distinct microcirculation, supplied by branches of the short posterior ciliary arteries. The optic nerve head circulation is exquisitely sensitive to perfusion pressure (the difference between blood pressure and intraocular pressure), and chronic optic nerve ischemia is the proposed mechanism behind normal-tension glaucoma.
All three vascular beds — retinal, choroidal, and optic nerve head — share the basic structural and functional properties that make them susceptible to ginkgo's microcirculatory mechanism: end-artery anatomy, high metabolic demand, sensitivity to viscosity and erythrocyte deformability, vulnerability to PAF-mediated platelet aggregation and leukocyte adhesion in capillaries, and dependence on adequate endothelial nitric oxide signaling for flow regulation. The clinical question is whether the mechanistic plausibility translates to measurable clinical benefit in patients with established ophthalmologic disease.
The Cochlear-Retinal Parallel
The most elegant conceptual frame for understanding ginkgo's ophthalmologic potential is the cochlear-retinal microcirculation parallel. The cochlea and the retina share an unusual set of structural features that no other major organs share:
- Both are supplied by end-arteries with limited collateral circulation (labyrinthine artery for the cochlea, central retinal artery and short posterior ciliary arteries for the retina)
- Both contain sensory cells (cochlear hair cells, retinal photoreceptors and ganglion cells) that are terminally differentiated and non-regenerating in mammals
- Both have exceptional metabolic demand relative to mass (stria vascularis in the cochlea, photoreceptors and RPE in the retina)
- Both are vulnerable to the same insults: aminoglycoside antibiotics damage cochlear hair cells and retinal ganglion cells; loop diuretics damage cochlear stria vascularis and can cause retinal toxicity at high IV dose; hyperviscosity syndromes affect both cochlear and retinal capillary perfusion; chronic hypertension produces both cochlear microvascular damage and retinal microvascular changes
- Both demonstrate age-related microcirculatory decline (presbycusis and presbyopia/age-related macular changes), and both are vulnerable to the same systemic conditions (diabetes, hyperlipidemia, atherosclerosis)
The clinical correlate of this anatomical parallel is the well-documented epidemiologic association between hearing loss and visual impairment in aging populations (dual sensory impairment increases dramatically after age 70), and the parallel mechanistic case for ginkgo in both cochlear ischemia (tinnitus, sudden sensorineural hearing loss) and retinal ischemia (normal-tension glaucoma, age-related macular degeneration). For the cochlear side of this parallel, see our Tinnitus page.
Fies & Dienel 2002 — The AMD Trial
The reference trial for ginkgo in age-related macular degeneration is Fies P & Dienel A (2002) "Ginkgo extract in impaired vision — treatment with special extract EGb 761 of impaired vision due to dry senile macular degeneration," published in Wiener Medizinische Wochenschrift. This was a randomized double-blind dose-comparison trial of two EGb 761 doses (60 mg/day vs 240 mg/day) in 99 patients with dry (non-neovascular) age-related macular degeneration over 6 months.
The primary outcome was change in best-corrected distance visual acuity. Secondary outcomes included near visual acuity, contrast sensitivity, and patient-reported visual function.
Results:
- The 240 mg/day arm showed mean visual acuity improvement of approximately 2.7 letters on the standard ETDRS chart; the 60 mg/day arm showed approximately 1.4 letters improvement. The between-dose difference was statistically significant.
- Contrast sensitivity improved more in the 240 mg/day arm
- Patient-reported visual function (reading speed, recognition of faces, ability to perform fine visual tasks) improved more in the 240 mg/day arm
- Adverse events were no more frequent in the 240 mg/day arm than the 60 mg/day arm, and overall the EGb 761 was well tolerated
The Fies & Dienel trial has several methodologic limitations: there was no placebo arm (both dose groups received active drug, which limits inference about absolute effect size); the trial was relatively short (6 months) for an AMD outcome; the sample size was modest; the visual acuity improvement, while statistically significant, was small enough that its clinical significance is debatable in the context of a slowly progressive degenerative disease.
Nonetheless, the trial established the EGb 761 240 mg/day dose as the appropriate dose for ophthalmologic applications (consistent with the cognitive and PAD trials), demonstrated a dose-response relationship, and provided proof-of-principle for ginkgo as an adjunct in dry AMD. It has not been followed by large definitive placebo-controlled trials, partly because the modern AMD treatment landscape has been dominated by AREDS supplementation and (for wet AMD) anti-VEGF intravitreal injections.
Quaranta 2003 — Normal-Tension Glaucoma
The reference trial for ginkgo in glaucoma is Quaranta L, Bettelli S, Uva MG, Semeraro F, Turano R, Gandolfo E (2003) "Effect of Ginkgo biloba extract on preexisting visual field damage in normal tension glaucoma," published in Ophthalmology. This was a randomized double-blind crossover trial in 27 patients with bilateral normal-tension glaucoma (NTG), comparing EGb 761 120 mg/day vs placebo for 4 weeks each, with an 8-week washout between phases.
Normal-tension glaucoma is the variant of primary open-angle glaucoma in which intraocular pressure is consistently within the statistically normal range (under 22 mmHg) but progressive optic nerve damage and visual field loss occur. The proposed mechanism is vascular dysregulation at the optic nerve head — impaired autoregulation of optic nerve perfusion, vasospasm of the short posterior ciliary arteries, and impaired endothelial function. NTG is the glaucoma subtype with the strongest mechanistic case for ginkgo benefit.
The primary outcome was change in Humphrey visual field mean defect (a quantitative measure of visual field loss; more negative numbers mean more loss).
Results:
- EGb 761 phase: mean visual field defect improved by approximately 2.4 dB (from baseline -11.50 dB to -9.10 dB)
- Placebo phase: no significant change in visual field defect
- The between-phase difference was statistically significant
- Intraocular pressure did not change in either phase (excluding IOP-lowering as the mechanism)
- No significant adverse events on EGb 761 at 120 mg/day for 4 weeks
This was a striking result — visual field improvement in a chronic neurodegenerative condition is uncommon. The trial's limitations are the small sample size (n=27), the short treatment duration (4 weeks per arm), and the crossover design (which can be vulnerable to carryover effects in glaucoma trials). Nonetheless, the result has been broadly cited as supporting the NTG-specific ginkgo indication and has been partially replicated in subsequent smaller trials.
The clinical translation: in normal-tension glaucoma patients who are already on maximum tolerable IOP-lowering therapy (prostaglandin analogs, beta-blockers, alpha agonists, carbonic anhydrase inhibitors, rho kinase inhibitors) and who continue to show visual field progression, adding EGb 761 240 mg/day is a reasonable adjunct with the explicit understanding that the evidence base is small and the patient should be co-managed with an ophthalmologist familiar with the glaucoma literature.
Age-Related Macular Degeneration — Mechanism & Trials
Age-related macular degeneration (AMD) is the leading cause of irreversible vision loss in adults over 65 in developed countries. It exists in two major forms:
- Dry (non-neovascular) AMD — the more common form. Characterized by accumulation of drusen (extracellular lipid-rich deposits) beneath the retinal pigment epithelium, with progressive loss of RPE cells and overlying photoreceptors in the macula. Slowly progressive over years. No effective treatment to halt progression; the AREDS / AREDS2 supplementation regimen reduces risk of advanced AMD by approximately 25% in patients with intermediate-stage disease.
- Wet (neovascular) AMD — the less common but more rapidly visually devastating form. Characterized by choroidal neovascularization — new abnormal blood vessels growing through Bruch's membrane into the subretinal space, leaking fluid and blood that disrupts retinal architecture. Treatment is intravitreal anti-VEGF injection (ranibizumab, bevacizumab, aflibercept, brolucizumab, faricimab) on monthly to quarterly intervals indefinitely.
The mechanistic case for ginkgo in dry AMD has several components:
- Choroidal microcirculation — choroidal blood flow declines progressively with age, and impaired choroidal perfusion has been documented in dry AMD using ICG angiography and OCT angiography. Ginkgo's PAF-antagonist and flavonoid-NO mechanisms target the same microcirculation
- Oxidative stress reduction — oxidative damage to the RPE is a major driver of dry AMD progression. Flavonoid antioxidant scavenging of reactive oxygen species in the RPE is mechanistically protective
- Reduced inflammatory cell adhesion — chronic low-grade choroidal inflammation contributes to AMD progression. Ginkgolide-B's PAF antagonism reduces PAF-mediated leukocyte adhesion and chemotaxis
- Iron and copper chelation — iron accumulation in the RPE contributes to oxidative stress through Fenton-reaction free-radical generation. Flavonoid metal chelation may modestly reduce this oxidative burden
The Cochrane 2013 review of ginkgo for AMD (Evans 2013) included only 2 trials with 119 patients and concluded that the evidence is "limited" and "inconclusive." The Fies & Dienel 2002 trial and the Lebuisson 1986 trial (the original French trial that showed visual acuity improvement with EGb 761 vs placebo) are the most-cited individual trials, but neither was large or definitive.
The practical positioning: ginkgo is not a substitute for AREDS / AREDS2 supplementation (which has high-quality evidence in the appropriate AMD population). It is not a substitute for anti-VEGF injection in wet AMD. It is a reasonable adjunct in dry AMD patients who want to optimize their non-AREDS supplementation, with the explicit understanding that the evidence is modest. For more on AMD see our Macular Degeneration page.
Glaucoma — NTG vs POAG
The ginkgo glaucoma literature has produced more consistent positive results in normal-tension glaucoma than in primary open-angle glaucoma. This pattern is consistent with the underlying mechanism — NTG is the glaucoma subtype with the strongest vascular component, while elevated-pressure POAG is dominated by mechanical injury to retinal ganglion cell axons at the optic nerve head.
- Normal-tension glaucoma (NTG) — intraocular pressure consistently below 22 mmHg with progressive optic nerve damage. Vascular dysregulation (vasospasm, impaired autoregulation, endothelial dysfunction) is the dominant proposed mechanism. The Quaranta 2003 trial is the key positive trial. The Park 2011 trial measured peripapillary retinal blood flow on color Doppler imaging and documented increased flow with EGb 761. The Cybulska-Heinrich 2012 series in Switzerland reported visual field stabilization or improvement in 80% of NTG patients on EGb 761 240 mg/day as adjunct.
- Primary open-angle glaucoma (POAG) — elevated intraocular pressure with progressive optic nerve damage. Mechanical pressure-induced injury is the dominant mechanism. Ginkgo trials in pure POAG have shown smaller and less consistent benefits. Ginkgo is not a substitute for IOP-lowering therapy in POAG.
- Acute angle-closure glaucoma — medical and surgical emergency requiring urgent IOP reduction. Ginkgo has no role.
- Pseudoexfoliation and pigmentary glaucoma — secondary open-angle glaucomas with specific mechanical drainage system pathology. Ginkgo is not a primary therapy but may be a reasonable adjunct after IOP control is optimized.
- Neovascular glaucoma — caused by retinal ischemia (diabetic, post-CRVO). Ginkgo is not a primary therapy; treatment is anti-VEGF and panretinal photocoagulation.
The Ritch 2000 hypothesis paper "Potential role for Ginkgo biloba extract in the treatment of glaucoma" in Medical Hypotheses is the most-cited theoretical framework for ginkgo in NTG and remains the conceptual basis for clinical use in this specific subtype. For more on glaucoma management, see our Glaucoma page.
Diabetic Retinopathy
Diabetic retinopathy is the leading cause of vision loss in working-age adults in developed countries. It is fundamentally a microvascular disease of the retina, with two major stages:
- Non-proliferative diabetic retinopathy (NPDR) — microaneurysms, dot-blot hemorrhages, hard exudates, cotton-wool spots, retinal edema, intraretinal microvascular abnormalities. Driven by hyperglycemia-induced endothelial damage, pericyte loss, capillary basement membrane thickening, and capillary nonperfusion.
- Proliferative diabetic retinopathy (PDR) — new vessel growth from the optic disc or elsewhere in response to retinal ischemia. Treatment is panretinal photocoagulation or anti-VEGF injection.
The mechanistic case for ginkgo in early NPDR is the same as in other microvascular indications: PAF antagonism reduces microvascular thrombosis and leukocyte adhesion, flavonoid antioxidant scavenging reduces hyperglycemia-induced oxidative damage, and improved erythrocyte deformability improves flow through narrowed capillaries.
The Lanthony & Cosson 1988 trial in early diabetic retinopathy measured color vision (an early functional marker of retinal dysfunction in diabetes) and documented improvement with EGb 761. Subsequent small trials have suggested benefit on visual field, retinal sensitivity, and microaneurysm count. The evidence base is too small to be definitive.
The clinical positioning: in patients with established diabetes and early NPDR (no center-involving edema, no proliferative changes), ginkgo at 240 mg/day is a reasonable adjunct to optimal glycemic control, statin therapy, blood pressure control, and ACE inhibitor therapy. It is not a substitute for the established interventions. In proliferative disease, ginkgo has no documented role and the bleeding-risk concern is amplified by the underlying retinal vascular fragility.
Direct Retinal Blood Flow Measurement
One of the strongest pieces of mechanistic evidence for ginkgo's ophthalmologic effects is the direct measurement of retinal blood flow before and after EGb 761 administration. Multiple studies using color Doppler imaging, laser Doppler velocimetry, and OCT angiography have documented:
- Chung 1999 — increased end-diastolic flow velocity in the ophthalmic artery after acute EGb 761 administration
- Park 2011 — increased peripapillary retinal blood flow on color Doppler imaging in NTG patients after EGb 761 treatment
- Wimpissinger 2007 — increased ocular blood flow in healthy subjects after acute EGb 761 dosing
- Cybulska-Heinrich 2012 — documented retinal vessel diameter and flow improvements correlating with visual field stabilization
The OCT angiography era (post-2014) has enabled quantitative measurement of macular and peripapillary capillary perfusion at much higher resolution than was previously possible. Modern OCT-A studies of ginkgo's effects on retinal capillary perfusion are still emerging but consistently support the mechanistic prediction that EGb 761 improves microvascular perfusion in tissues with baseline reduced perfusion.
The AREDS Question — Why Ginkgo Is Not in the Formula
A frequent patient question is why ginkgo is not included in the AREDS or AREDS2 supplementation formula, given its plausibility for AMD. The answer reflects the trial-design history rather than a definitive judgment about ginkgo's efficacy:
- The original AREDS formula (2001) was developed in the late 1990s by NEI investigators who selected antioxidants and zinc based on the prevailing epidemiologic evidence at the time — Vitamin C, Vitamin E, beta-carotene, zinc, and copper. Ginkgo was not on the candidate list because the dry AMD efficacy trials were still pending.
- The AREDS2 formula (2013) modified the original by substituting lutein and zeaxanthin for beta-carotene (which had increased lung cancer risk in former smokers) and added omega-3 fatty acids in one arm (which did not show additional benefit). Ginkgo was again not included because no large definitive trial had been performed in AMD.
- No pharmaceutical or supplement sponsor has funded a large definitive trial of EGb 761 in AMD — the patent has long expired, the regulatory pathway in the US is the dietary supplement framework rather than the drug framework, and the AMD treatment landscape has been dominated by intravitreal anti-VEGF for wet AMD.
- The German practice pattern of adding EGb 761 240 mg/day to AREDS for dry AMD patients is reasonable but does not have RCT support comparable to AREDS itself.
The practical implication: AREDS or AREDS2 is the evidence-based first-line nutritional intervention for intermediate-stage dry AMD. EGb 761 is a reasonable adjunct with smaller and less consistent evidence. Patients who pursue both should ensure they are using a quality AREDS2 formula and a standardized EGb 761 product, not generic substitutes.
Dosing Protocol
- Dose: EGb 761 240 mg/day, split as 120 mg twice daily with meals. The Fies & Dienel 2002 dose-response data in AMD support 240 mg/day over 60 mg/day.
- Duration: minimum 12 weeks before initial response assessment; ophthalmologic outcomes typically require 6 months or longer to demonstrate stable change. For chronic indications (NTG, dry AMD), ginkgo is typically continued indefinitely if tolerated and producing benefit.
- Form: standardized EGb 761 extract. Brand names include Tebonin (Germany), Tanakan (France), Ginkgold (Nature's Way), Ginkoba (Pharmaton).
- Combination with AREDS2: no significant interaction; the two are reasonably combined in dry AMD with appropriate supplementation.
- Population most likely to respond: dry AMD with baseline preserved central acuity, NTG with documented visual field progression on maximum IOP-lowering therapy, early NPDR with optimal glycemic control.
- Population unlikely to respond: end-stage dry AMD with severe geographic atrophy, wet AMD without anti-VEGF therapy, advanced POAG, proliferative diabetic retinopathy.
- Response assessment: serial Humphrey visual fields for glaucoma; OCT macular thickness and ETDRS visual acuity for AMD; serial fundus photography and color vision testing for early diabetic retinopathy.
Cautions — Retrobulbar Hemorrhage and Glaucoma Drug Interactions
- Retrobulbar hemorrhage risk during ocular procedures — case reports document retrobulbar hemorrhage during cataract surgery, vitrectomy, and intravitreal injection in ginkgo users. Discontinue ginkgo at least 14 days before any planned ocular procedure, including cataract surgery, vitreoretinal surgery, glaucoma drainage device implantation, and corneal transplant. For intravitreal injections (anti-VEGF), the risk is less but bleeding-augmented complications such as suprachoroidal hemorrhage have been described.
- Bleeding risk in patients on antiplatelet therapy for cardiovascular disease — older AMD patients are commonly on aspirin or clopidogrel. The ginkgo-plus-aspirin combination has been associated with spontaneous bleeding including intraocular hemorrhage. Risk-benefit assessment should be explicit.
- Interaction with topical glaucoma drugs — no clinically significant pharmacokinetic interaction with prostaglandin analogs, beta-blockers, alpha agonists, carbonic anhydrase inhibitors, rho kinase inhibitors, or topical pilocarpine. Ginkgo is compatible with maximum tolerable medical IOP-lowering therapy.
- Interaction with anti-VEGF intravitreal therapy — no documented pharmacokinetic interaction. Bleeding-risk concerns argue for ginkgo discontinuation 14 days before scheduled injection.
- Subconjunctival hemorrhage — mild spontaneous subconjunctival bleeding is occasionally reported with ginkgo and is benign but cosmetically distressing. Frequent recurrence should prompt discontinuation.
- Pregnancy and breastfeeding — insufficient safety data. AMD and glaucoma are rare in reproductive-age women but the caution applies.
- Diabetes — ginkgo modestly affects insulin secretion and glucose disposition. Diabetic patients starting ginkgo should monitor glucose patterns and report hypoglycemia. Tight glycemic control is the foundation of diabetic retinopathy prevention; ginkgo is an adjunct.
- Seizure threshold — ginkgo is contraindicated in epilepsy. Glaucoma patients on topiramate (a carbonic anhydrase inhibitor with anticonvulsant properties) for either glaucoma or seizure management should not add ginkgo.
- Pre-operative anesthesia disclosure — failure to disclose ginkgo use to the ophthalmologist before any planned procedure is a documented cause of intra-operative bleeding. Always include ginkgo (and all herbal supplements) in the surgical pre-operative medication list.
Key Research Papers
- Quaranta L, Bettelli S, Uva MG, Semeraro F, Turano R, Gandolfo E (2003). Effect of Ginkgo biloba extract on preexisting visual field damage in normal tension glaucoma. Ophthalmology 110(2):359-362. — PubMed
- Fies P, Dienel A (2002). Ginkgo extract in impaired vision — treatment with special extract EGb 761 of impaired vision due to dry senile macular degeneration. Wiener Medizinische Wochenschrift 152(15-16):423-426. — PubMed
- Evans JR (2013). Ginkgo biloba extract for age-related macular degeneration. Cochrane Database of Systematic Reviews (1):CD001775. — PubMed
- Lebuisson DA, Leroy L, Rigal G (1986). Treatment of senile macular degeneration with Ginkgo biloba extract. A preliminary double-blind drug versus placebo study. Presse Med 15(31):1556-1558. — PubMed
- Park JW, Kwon HJ, Chung WS, Kim CY, Seong GJ (2011). Short-term effects of Ginkgo biloba extract on peripapillary retinal blood flow in normal tension glaucoma. Korean Journal of Ophthalmology 25(5):323-328. — PubMed
- Cybulska-Heinrich AK, Mozaffarieh M, Flammer J (2012). Ginkgo biloba: an adjuvant therapy for progressive normal and high tension glaucoma. Molecular Vision 18:390-402. — PubMed
- Ritch R (2000). Potential role for Ginkgo biloba extract in the treatment of glaucoma. Medical Hypotheses 54(2):221-235. — PubMed
- Chung HS, Harris A, Kristinsson JK, Ciulla TA, Kagemann C, Ritch R (1999). Ginkgo biloba extract increases ocular blood flow velocity. Journal of Ocular Pharmacology and Therapeutics 15(3):233-240. — PubMed
- Hirooka K, Tokuda M, Miyamoto O, Itano T, Baba T, Shiraga F (2004). The Ginkgo biloba extract (EGb 761) provides a neuroprotective effect on retinal ganglion cells in a rat model of chronic glaucoma. Current Eye Research 28(3):153-157. — PubMed
- Lanthony P, Cosson JP (1988). The course of color vision in early diabetic retinopathy treated with Ginkgo biloba extract. Journal Français d'Ophtalmologie 11(10):671-674. — PubMed
- Wimpissinger B, Berisha F, Garhoefer G, Polak K, Schmetterer L (2007). Influence of Ginkgo biloba on ocular blood flow. Acta Ophthalmologica Scandinavica 85(4):445-449. — PubMed
- Mozaffarieh M, Flammer J (2007). Is there more to glaucoma treatment than lowering IOP? Survey of Ophthalmology 52 Suppl 2:S174-179. — PubMed
PubMed Topic Searches
- PubMed: Ginkgo for macular degeneration
- PubMed: Ginkgo for glaucoma (NTG)
- PubMed: Ginkgo retinal/ocular blood flow
- PubMed: Ginkgo for diabetic retinopathy
- PubMed: RGC neuroprotection
Connections
- Ginkgo Biloba Overview
- Ginkgo Biloba Benefits Hub
- Ginkgo for Cognitive Function
- Ginkgo for Circulation & PAD
- Ginkgo for Tinnitus
- Macular Degeneration
- Glaucoma
- Ophthalmology
- Vitamin A for Vision
- Vitamin E
- Zinc
- All Herbs
- Turmeric
- Methylene Blue
- Diabetes