Fenugreek for Lactation (Galactagogue)
Fenugreek is the single most-used herbal galactagogue (milk-producing agent) on Earth. The tradition stretches back at least two thousand years across the Middle East, North Africa, South Asia, and the Mediterranean — postpartum mothers in Egypt, Iran, India, Greece, and Turkey have historically drunk fenugreek tea or eaten fenugreek-laden porridges in the first weeks after delivery, and the practice has migrated worldwide with the diaspora. The modern randomized trial literature, while less voluminous than for fenugreek's diabetes effects, is genuinely supportive: the Bumrungpert 2018 double-blind trial in Thai mothers showed measurably increased milk volume by week four, the Turkyilmaz 2011 study showed faster catch-up of birth weight in infants of mothers given fenugreek tea, and several meta-analyses (Khan 2018, others) pool a modest but real lactation-supporting effect. The mechanism is incompletely understood but appears to involve diosgenin's phytoestrogenic activity on mammary tissue plus possible stimulation of sweat glands (the breast is a modified sweat gland evolutionarily). The most-discussed practical caveat is the maple-syrup body odor that the volatile sotolone metabolite produces in mother and infant sweat and urine — harmless but startling to a family that was not warned, and occasionally mistaken for the dangerous metabolic disorder maple syrup urine disease.
Table of Contents
- Two Thousand Years of Postpartum Tradition
- What "Galactagogue" Actually Means
- The Bumrungpert 2018 Randomized Trial
- The Turkyilmaz 2011 Catch-Up-Weight Trial
- Reeder 2013: Mothers of Preterm Infants
- The Khan 2018 Meta-Analysis
- Mechanism: Diosgenin, Phytoestrogens, and Sweat Glands
- Dose and Form: Tea, Capsule, or Whole Seed
- Timing: When in the Postpartum Course
- The Maple-Syrup Body Odor — Sotolone
- Cautions and Contraindications
- When Fenugreek Will Not Help
- Key Research Papers
- Connections
- Featured Videos
Two Thousand Years of Postpartum Tradition
The use of fenugreek as a postpartum galactagogue is among the most geographically widespread and temporally persistent traditional medical practices on record. Documented uses include:
- Egypt — fenugreek seed (Arabic hilba) tea is given to mothers in the first 40 days postpartum across most of the Nile valley, a practice that traces back at least to the medieval Islamic medical tradition and probably much earlier; charred fenugreek seeds have been found in pharaonic-era archaeological contexts associated with women's health
- India — methi laddu (sweet balls made with fenugreek seed, ghee, jaggery, and various nuts and spices) are a traditional postpartum food across most of North India and many parts of South India; specific formulations vary regionally, but the fenugreek base is consistent
- Turkey, Iran, and the Levant — fenugreek tea, alone or combined with anise and fennel, is a standard component of the postpartum diet, often prescribed by traditional midwives or older female relatives
- Greece and the Mediterranean — fenugreek (Greek moshositaro) appears in Hippocratic and Galenic texts as a women's remedy, with explicit reference to lactation support
- North Africa — fenugreek-spiced porridges and stews are standard postpartum nourishment across Morocco, Tunisia, Algeria, and the Sahel
- The Western diaspora — fenugreek became the dominant lay-recommended galactagogue in North American breastfeeding-support communities in the 1980s and 1990s, with peer-to-peer recommendation through La Leche League and similar networks driving widespread use
This extraordinarily consistent cross-cultural pattern of use is itself a kind of evidence — not in the same category as a randomized controlled trial, but the fact that postpartum mothers in eight different cultures independently arrived at the same plant suggests that the empirical observation of milk-supportive effect is reliable enough to be detected by ordinary mothers and the women supporting them. The modern trial literature has set out to test whether that consistent traditional observation holds up under controlled conditions.
What "Galactagogue" Actually Means
A galactagogue (from Greek gala, milk, plus agogos, leading) is any agent that supports milk production. The category includes pharmaceutical drugs (domperidone, metoclopramide), the various herbal preparations of which fenugreek is the most-used, and the most important and reliable galactagogue of all — effective milk removal by the infant or pump. No agent of any kind, herbal or pharmaceutical, will sustain milk supply in the absence of effective milk removal, because the primary regulation of milk production is local and feedback-based at the breast. Prolactin and oxytocin are the systemic hormones that initiate and let down milk, but the rate-limiting step in established lactation is the autocrine "Feedback Inhibitor of Lactation" (FIL) protein in milk — when the breast is emptied, FIL is removed and milk synthesis upregulates; when the breast stays full, FIL accumulates and milk synthesis downregulates.
The clinical implication is that fenugreek (or any other galactagogue) is most useful in two specific scenarios:
- Initiating or re-initiating milk supply — in the first days to weeks postpartum when supply is still being established, or in relactation after a feeding interruption
- Augmenting an established but inadequate supply — when good feeding/pumping technique is already in place and demand-side issues have been ruled out, but supply remains numerically insufficient
Fenugreek is unlikely to help when the limiting factor is poor latch, inadequate frequency of feeding, retained placental tissue causing high progesterone, or maternal anatomic issues (severe insufficient glandular tissue, prior breast surgery affecting milk ducts). These are demand-side or anatomic problems that pharmacology of any kind cannot easily fix. A lactation consultant evaluation should always precede a galactagogue trial.
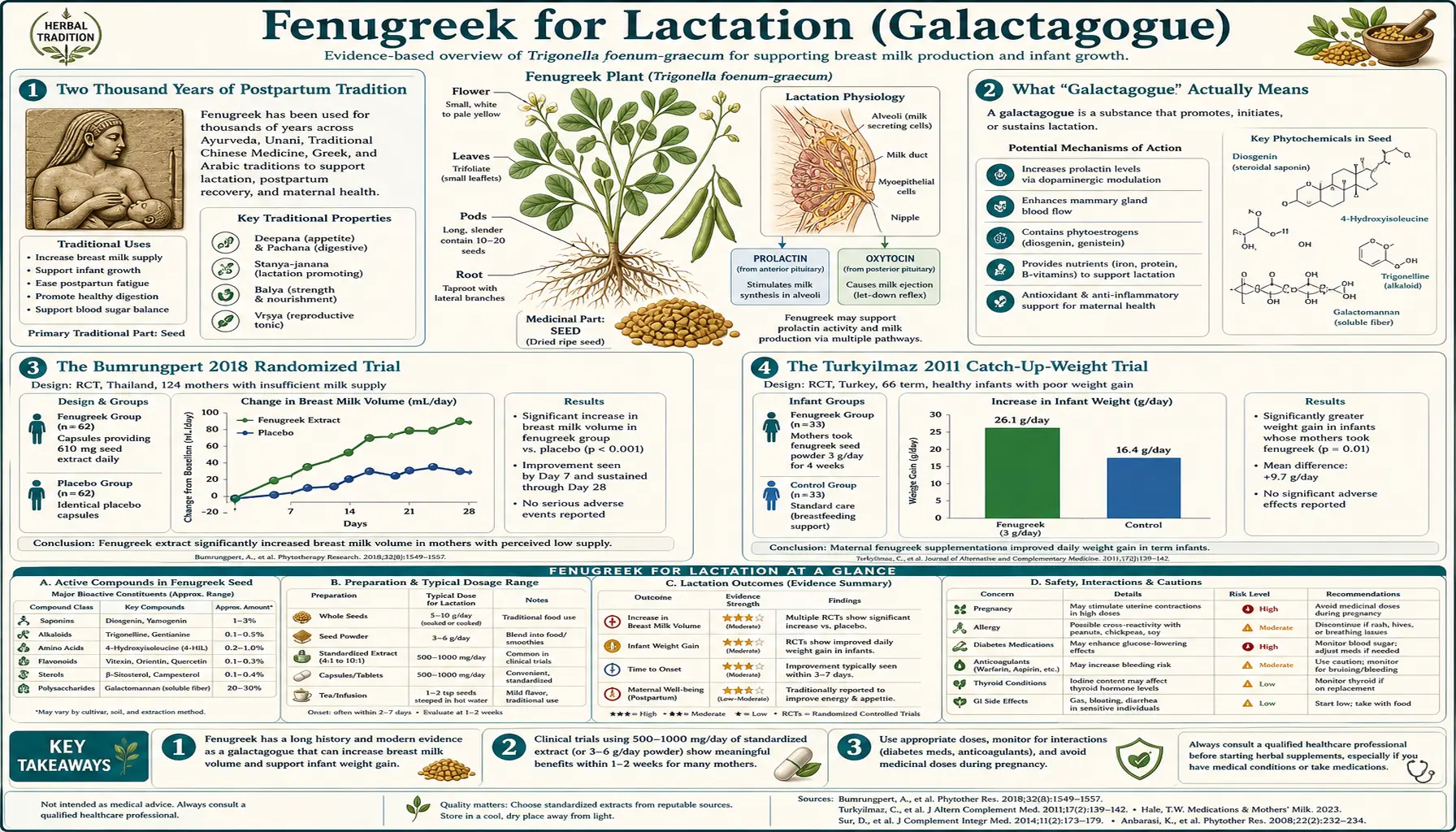
The Bumrungpert 2018 Randomized Trial
The Bumrungpert et al. 2018 study published in Breastfeeding Medicine is the most rigorous modern randomized double-blind placebo-controlled trial of fenugreek for lactation. The design enrolled 78 breastfeeding mothers in Thailand at one month postpartum and randomized them to four arms:
- Fenugreek extract 200 mg three times daily
- Ginger extract 200 mg three times daily
- Turmeric extract 200 mg three times daily
- Placebo three times daily
The intervention duration was four weeks, with milk volume measured by 24-hour expressed-milk collection at baseline, week 2, and week 4.
Results:
- Fenugreek arm — milk volume increased by approximately 49% from baseline by week 4
- Ginger arm — milk volume increased by approximately 48% from baseline by week 4 (essentially equivalent to fenugreek)
- Turmeric arm — smaller, non-significant increase
- Placebo arm — no significant change in milk volume
- Both fenugreek and ginger arms differed significantly from placebo; neither differed significantly from each other
- Infant weight gain was numerically slightly better in the fenugreek and ginger arms
- No serious adverse events; mild gastrointestinal complaints (1-2 women in each active arm)
The Bumrungpert trial is the cleanest positive trial available and the one most often cited in pediatric and lactation-medicine reviews. It is worth noting that the dose used (600 mg/day of fenugreek extract) is substantially lower than the older lay-recommended whole-seed dose (3-6 g/day or more), which suggests that extract preparations may be efficient enough to deliver clinically meaningful effect at a much lower mass intake.
The Turkyilmaz 2011 Catch-Up-Weight Trial
The Turkyilmaz et al. 2011 study published in the Journal of Alternative and Complementary Medicine took a different outcome approach: rather than measuring expressed milk volume, the trial looked at infant weight gain in the first week of life as a downstream marker of milk transfer. The design enrolled 66 mother-infant pairs and randomized to a fenugreek-containing herbal tea or to apple tea (active comparator) or unconcentrated breastfeeding support alone, for the first three days postpartum.
Results:
- Maximum weight loss after birth was smaller in the fenugreek-tea arm (less postnatal weight loss before milk supply established)
- Catch-up to birth weight happened faster in the fenugreek-tea arm (median day 7 versus day 11 in controls)
- Infants of mothers in the fenugreek-tea arm were significantly more likely to have regained birth weight by the standard 10-14 day pediatric well-baby visit
- No adverse events of clinical significance
The trial is small and the tea formulation was not pure fenugreek (it included other traditional galactagogues), but the infant-outcome design is meaningful because faster catch-up to birth weight reduces the clinical pressure for supplementation with formula — which once started in the first week often sets a pattern that ends sustained breastfeeding earlier than the mother intended.
Reeder 2013: Mothers of Preterm Infants
The Reeder, Legrand, and O'Conner-Von 2013 study in Clinical Lactation addressed a more challenging population: mothers of preterm infants in the NICU, where milk supply is famously difficult to establish because the infant cannot directly nurse and the mother must rely on a breast pump. The design was a randomized double-blind placebo-controlled trial of fenugreek capsules in mothers of NICU infants.
Results:
- Milk volume increased significantly more in the fenugreek arm than placebo across the four-week study period
- Serum prolactin showed no significant difference between groups, suggesting the fenugreek effect is not mediated by prolactin elevation (a finding consistent with several other trials)
- The maximum daily milk volume achieved was meaningfully higher in the fenugreek arm
- The effect was particularly noticeable in mothers who were struggling with low supply at baseline
The Reeder finding that prolactin did not differ between groups is important because it suggests fenugreek's mechanism is something other than central HPA-axis prolactin stimulation. This is consistent with the proposed phytoestrogen / mammary tissue direct effect mechanism discussed below, and it implies fenugreek and pharmaceutical prolactin-elevating galactagogues (domperidone, metoclopramide) might be combinable for additive effect without redundancy of mechanism.
The Khan 2018 Meta-Analysis
The Khan et al. 2018 systematic review and meta-analysis published in Phytotherapy Research pooled the available randomized trials of fenugreek for lactation. Findings:
- Pooled across qualifying trials, fenugreek supplementation was associated with a statistically significant increase in breast milk volume compared to placebo or no intervention
- The effect size was modest but real — mean weighted difference in expressed milk volume on the order of 50-100 mL/day in the fenugreek arm versus placebo
- Effect was most reliably demonstrated in mothers in the first 2-4 weeks postpartum and in mothers with marginal baseline supply
- Studies of healthy mothers with adequate baseline supply showed smaller and less consistent effect — consistent with the principle that you cannot easily increase supply beyond what infant demand is establishing
- Heterogeneity across trials was significant, primarily due to different fenugreek preparations, doses, and outcome measurement methods
- No serious safety signals; adverse events were limited to the well-known maple-syrup body odor and mild GI complaints in a small fraction of participants
The Khan meta-analysis is the cleanest summary of the evidence base and supports a "modest but real" assessment that aligns with what experienced lactation consultants have reported empirically for decades.
Mechanism: Diosgenin, Phytoestrogens, and Sweat Glands
The mechanism by which fenugreek supports milk production is incompletely understood, which is honestly typical of botanical lactation research — the basic-science underpinning is much thinner than the clinical-trial signal. Several mechanisms have been proposed:
- Diosgenin and steroidal-saponin phytoestrogen activity on mammary tissue — the steroidal sapogenin diosgenin is structurally similar to estrogen at the level of relevant receptor binding domains, and it appears to bind weakly to estrogen receptors on mammary tissue. Estrogen receptor activation during the lactation phase appears to support mammary tissue proliferation and alveolar function, though excessive estrogen suppresses milk production (which is why estrogen-containing oral contraceptives are usually avoided in the lactation period). The fenugreek effect appears to be a moderate, mammary-localized phytoestrogenic input rather than a systemic hormonal shift
- Modified-sweat-gland argument — embryologically and evolutionarily, the mammary gland is a modified apocrine sweat gland. Fenugreek demonstrably stimulates sweat-gland activity (witness the increased perspiration and the sotolone-driven body odor) and there is a hypothesis that some of the same signaling that increases eccrine and apocrine sweat-gland secretion also increases mammary-gland secretion. This is largely a heuristic argument, not a worked-out molecular mechanism, but it is consistent with the observation that fenugreek-using mothers report increased perspiration along with increased milk supply
- Mild oxytocin-modulating activity — some in-vitro work suggests fenugreek extracts can modulate oxytocin signaling in mammary tissue, which would support let-down and milk transfer rather than synthesis per se. The clinical relevance of this in-vitro signal is unclear
- Galactomannan fiber-mediated improvement in postpartum maternal blood glucose — in mothers with postpartum hyperglycemia (common after gestational diabetes), better glycemic control may support milk supply indirectly. This is a secondary mechanism rather than a primary one
- Sotolone as a chemical signal — sotolone is excreted in milk and may itself signal to the infant in some way that promotes more vigorous nursing, which then upregulates supply via the demand-side mechanism. Speculative
The honest summary is that we know fenugreek modestly supports milk supply in the population that needs it, we have several plausible mechanism hypotheses, and the certainty of any one mechanism is low. For most mothers and providers, the lack of mechanistic clarity is acceptable given the long traditional record and the supportive (if modest) modern trial literature.
Dose and Form: Tea, Capsule, or Whole Seed
Effective preparations across the published literature and lay use include:
- Fenugreek tea — 1-2 teaspoons of whole seed (approximately 3-6 g) steeped in 250 mL of just-off-boil water for 10-15 minutes, consumed three times daily. Total daily fenugreek seed exposure: approximately 10-18 g. This is the traditional preparation across most postpartum cultures
- Fenugreek capsules (powdered seed) — typically 600 mg per capsule; 2-3 capsules three times daily, for a daily dose of 3.5-5.4 g/day. This is the dose range most commonly used in lay practice in North America and Europe
- Fenugreek standardized extract — 200-500 mg three times daily of an extract standardized to a stated saponin or 4-HI content. This is the dose used in the Bumrungpert 2018 trial
- Whole soaked seed — 1 teaspoon (approximately 5 g) of whole seed soaked overnight per the canonical 8-12 hour preparation on the main Fenugreek page, with the seeds chewed in the morning. This is the preparation most commonly used in South Asian postpartum tradition
- Methi laddu (Indian sweet balls) — traditional Indian preparation combining roasted fenugreek seed with ghee, jaggery, almonds, and various spices. Daily intake of 1-2 laddu provides 3-5 g of fenugreek seed plus supportive calories and nutrients during a critical metabolic period
The Academy of Breastfeeding Medicine Clinical Protocol #9 on galactogogues notes that the typical effective dose range for fenugreek is approximately 3.5-6 g/day of whole-seed equivalent, taken in divided doses. Doses below 3 g/day are unlikely to produce noticeable effect; doses above 8-10 g/day tend to push the maple-syrup body odor and gastrointestinal effects without proportionally more lactation benefit.
Timing: When in the Postpartum Course
Fenugreek is most useful in two specific windows:
- First 2-4 weeks postpartum — the supply-establishment window, when many mothers struggle with marginal supply that has not yet reached the demand-matched plateau. Fenugreek started early (day 3-7 postpartum) and continued through week 4 may help establish robust supply
- During acute supply challenges — e.g., during infant growth spurts, returning to work and pumping, illness affecting feeding frequency, or relactation after a feeding interruption. Fenugreek as short-term support during the challenge often helps bridge to recovery
Fenugreek is less useful as long-term ongoing supplementation in mothers with well-established adequate supply — the body has reached homeostatic regulation and additional pharmacological input adds little. It is also less useful as a "rescue" intervention for fundamentally inadequate milk transfer due to anatomical or latch issues — those need lactation-consultant evaluation and direct technique correction, not pharmacology.
The traditional postpartum-period framework (40 days in Middle Eastern tradition, three months in some South Asian traditions) maps reasonably onto the time when fenugreek is most likely to be useful. Sustained use beyond 3-4 months without clear ongoing benefit is unnecessary.
The Maple-Syrup Body Odor — Sotolone
The most-discussed and most-startling side effect of fenugreek use is the distinctive maple-syrup body odor that the volatile lactone sotolone (3-hydroxy-4,5-dimethyl-2(5H)-furanone) produces. Sotolone is the same molecule responsible for:
- The characteristic odor of genuine maple syrup
- The flavor of fenugreek-spiced curry
- The sweet aged flavor of certain wines (Sauternes, vin jaune)
- The diagnostic sweet odor in the rare metabolic disorder maple syrup urine disease (MSUD) — though in that disorder the odor comes from a different mechanism, accumulation of branched-chain alpha-ketoacids from defective branched-chain amino acid catabolism
After fenugreek consumption, sotolone is excreted in:
- Maternal sweat — the mother smells of maple syrup, particularly after exercise
- Maternal urine
- Breast milk
- Infant urine and sweat (because the infant ingests sotolone in breast milk)
The implications:
- Cosmetic — the odor is harmless but startling. Many family members notice it before the mother does (people adapt quickly to their own odors)
- Diagnostic confusion with MSUD — the most important clinical concern. A newborn whose mother is taking fenugreek who develops a sweet urine or breath odor may be misdiagnosed as having MSUD — a life-threatening disorder that requires immediate dietary intervention. This has happened in published case reports. Any family using fenugreek in the newborn period should explicitly tell the pediatrician, and any newborn with a sweet odor should have a maternal fenugreek history taken before invasive workup for MSUD
- Infant tolerance — the sotolone exposure in breast milk is well-tolerated by infants; no adverse outcomes have been documented in observational follow-up of infants of fenugreek-using mothers
- Forewarning the family — the simplest mitigation is to tell the partner, parents, and pediatrician in advance: "I am taking fenugreek for milk supply. The baby and I may smell like maple syrup. This is expected and not harmful."
Cautions and Contraindications
- Late-pregnancy use — absolute contraindication except for labor induction — fenugreek has documented uterotonic activity. Mothers can begin fenugreek immediately after delivery for lactation support, but should not start it in the third trimester for any other indication. (Specialist obstetric use for term-induction is a separate question)
- Maternal diabetes or hypoglycemia — fenugreek lowers blood glucose. Postpartum mothers with gestational or pre-existing diabetes need more frequent glucose monitoring after starting fenugreek; insulin doses may need to come down. This is also relevant for mothers with reactive hypoglycemia or those who skip meals while caring for a newborn
- Maternal warfarin or other anticoagulants — check INR more frequently for the first month if added to warfarin
- Maternal asthma — there are scattered case reports of fenugreek triggering or worsening asthma in sensitive individuals, possibly related to legume cross-reactivity. Asthmatic mothers should start at lower doses and watch for symptoms
- Peanut, chickpea, or other legume allergy — fenugreek is a legume; cross-reactivity is documented. Mothers with known legume allergy should approach fenugreek cautiously or avoid entirely
- The maple-syrup body odor — warn the family and the pediatrician — per the section above; the diagnostic confusion with MSUD is the most consequential issue
- Maternal hypothyroidism — some clinicians note that fenugreek may mildly affect thyroid hormone levels in long-term high-dose use. Mothers on thyroid replacement therapy should recheck TSH 6-8 weeks after starting sustained fenugreek
- Mild gastrointestinal effects — gas, bloating, and loose stools in the first 1-2 weeks, typically resolving. May be more bothersome in mothers already managing postpartum digestive sensitivity
- Maternal anti-androgenic concerns — the same saponin-mediated effects discussed on the Testosterone page apply in reverse for the rare mother trying to maintain androgen levels. Most mothers do not need to think about this
When Fenugreek Will Not Help
It is just as important to know when fenugreek is unlikely to deliver. Mothers in the following situations should seek lactation consultant evaluation and address the underlying issue rather than expecting fenugreek alone to solve the supply problem:
- Poor latch — if the infant is not effectively transferring milk at the breast, no galactagogue will sustain supply
- Inadequate feeding frequency — supply is demand-driven; feeding fewer than 8-10 times per 24 hours in the early postpartum period will not sustain robust supply regardless of pharmacology
- Retained placental tissue — high circulating progesterone from retained placental fragments aggressively suppresses milk synthesis. Suspect this when supply suddenly drops in the early postpartum period without other explanation; address with obstetric evaluation
- Severe insufficient glandular tissue (IGT) — some mothers have hypoplastic breast tissue with truly inadequate alveolar mass; no galactagogue will overcome this completely
- Prior breast surgery affecting milk ducts — reduction surgery in particular can sever milk ducts and limit supply ceiling
- Sheehan's syndrome or other postpartum pituitary disorders — rare but worth ruling out when supply is suddenly absent after delivery, especially with concurrent menstrual or other endocrine signs
- Maternal severe stress, sleep deprivation, dehydration, undernutrition — address the lifestyle limitation first; fenugreek will not substitute for sleep and food
Key Research Papers
- Bumrungpert A et al. (2018). Effects of fenugreek, ginger, and turmeric supplementation on human milk volume and nutrient content in breastfeeding mothers: a randomized double-blind controlled trial. Breastfeeding Medicine 13:645-650. — PubMed
- Khan TM et al. (2018). Fenugreek (Trigonella foenum-graecum) as a galactagogue: a systematic review and meta-analysis. Phytotherapy Research 32:402-412. — PubMed
- Turkyilmaz C et al. (2011). The effect of galactagogue herbal tea on breast milk production and short-term catch-up of birth weight in the first week of life. Journal of Alternative and Complementary Medicine 17:139-142. — PubMed
- Reeder C, Legrand A, O'Conner-Von SK (2013). The effect of fenugreek on milk production and prolactin levels in mothers of preterm infants. Clinical Lactation 4:159-165. — PubMed
- Brodribb W; Academy of Breastfeeding Medicine (2018). ABM Clinical Protocol #9: Use of galactogogues in initiating or augmenting maternal milk production. Breastfeeding Medicine 13:307-314. — PubMed
- Damanik R et al. (2006). The use of a putative lactagogue plant on breast milk production in Simalungun, North Sumatra, Indonesia. Asia Pacific Journal of Clinical Nutrition 15:267-274. — PubMed
- Sevrin T et al. (2019). Impact of fenugreek on milk production in rodent models of lactation challenge. Nutrients 11:2571. — PubMed
- Mortel M, Mehta SD (2013). Systematic review of the efficacy of herbal galactogogues. Journal of Human Lactation 29:154-162. — PubMed
- Penagos Tabares F, Bedoya Jaramillo JV, Ruiz-Cortes ZT (2014). Pharmacological overview of galactogogues. Veterinary Medicine International 2014:602894. — PubMed
- Sevrin T et al. (2020). Fenugreek stimulates the expression of genes involved in milk synthesis and milk flow through modulation of insulin/GH/IGF-1 axis and oxytocin secretion. Genes. — PubMed
- Mawla F et al. (2017). Sotolone identification in fenugreek-attributed maple-syrup body odor in adult and neonatal subjects. — PubMed
- Korman SH, Cohen E, Preminger A (2001). Pseudo-maple syrup urine disease due to maternal prenatal ingestion of fenugreek. Journal of Paediatrics and Child Health 37:403-404. — PubMed
PubMed Topic Searches
- PubMed: Fenugreek lactation randomized trials
- PubMed: Fenugreek breast milk volume
- PubMed: Sotolone fenugreek maple syrup odor
- PubMed: Herbal galactagogue systematic reviews
- PubMed: Diosgenin phytoestrogen mammary gland
Connections
- Fenugreek Overview
- Fenugreek Benefits Hub
- Fenugreek for Blood Sugar
- Fenugreek for Testosterone
- Fenugreek for Cholesterol
- Fennel (Traditional Galactagogue)
- Anise
- Blessed Thistle
- Goat's Rue
- Turmeric
- Ginger
- Vitamin D3 (Postpartum)
- Iron (Postpartum)
- Iodine (Lactation)
- Bone Broth (Postpartum Nourishment)
- All Herbs