Fenugreek for Cholesterol & Lipid Profile
Fenugreek seed lowers serum cholesterol primarily through its soluble galactomannan fiber, which physically binds bile acids in the intestinal lumen and forces the liver to draw down circulating LDL cholesterol to synthesize replacement bile. This is mechanistically the same family of action as oat beta-glucan, psyllium husk, and the pharmaceutical bile-acid sequestrants (cholestyramine, colesevelam). The defining clinical evidence is the Sharma 1996 trial in non-insulin-dependent diabetic patients with hypercholesterolemia, which used 100 g/day of defatted fenugreek seed powder for 24 weeks and reduced total cholesterol by approximately 30% and LDL by approximately 35%. Several subsequent smaller trials at more practical doses (10-25 g/day) have shown smaller but still meaningful reductions. The clinical reality is that the dose required for a clear cholesterol effect (15-25 g/day of whole seed at minimum) is substantially higher than the dose required for glycemic benefit, and substantially higher than most patients will sustain without significant gastrointestinal effects. This makes fenugreek a reasonable adjunct to oat fiber, psyllium, statin therapy, or dietary cholesterol management — not a stand-alone solution for clinically significant hypercholesterolemia.
Table of Contents
- Why Soluble Fiber Lowers Cholesterol
- The Sharma 1996 Hypercholesterolemia Trial
- The Bordia 1997 Coronary Artery Disease Trial
- Sowmya 1999: Germinated Fenugreek
- Geberemeskel 2019: Glycemic + Lipid Combined
- The Galactomannan Bile-Acid Binding Mechanism
- LDL Reduction with Preserved HDL
- Fenugreek Galactomannan vs Oat Beta-Glucan vs Psyllium
- The Dose Required: Higher Than for Glycemic Benefit
- Fenugreek vs Statin Therapy
- Practical Use: Combining With Diet and Other Fibers
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
Why Soluble Fiber Lowers Cholesterol
Before examining fenugreek specifically, it helps to understand why any soluble fiber lowers serum cholesterol. The body uses cholesterol as the starting material for bile acid synthesis. Bile acids are secreted into the small intestine from the gallbladder after a fatty meal, where they emulsify fats for digestion and absorption. After the digestive task is complete, approximately 95% of the secreted bile acids are reabsorbed in the terminal ileum and returned to the liver via the portal vein — the so-called enterohepatic circulation. This recycling allows the liver to synthesize relatively little new bile acid each day, conserving cholesterol.
Soluble fibers like galactomannan, beta-glucan, and psyllium mucilage disrupt this elegant recycling system. They form a viscous gel in the small intestine that physically traps bile acids and carries them through to the colon and out of the body in stool. The liver, deprived of its recirculating bile acid pool, has no choice but to synthesize new bile acids from circulating LDL cholesterol, drawing down serum LDL concentrations in the process. This is the same mechanism by which the pharmaceutical bile acid sequestrants (cholestyramine, colesevelam, colestipol) lower serum LDL — they bind bile acids in the intestinal lumen with even higher affinity than soluble fibers do.
The mechanism implies certain predictions that the clinical trial data has borne out:
- The effect is dose-dependent and proportional to the amount of viscous soluble fiber consumed
- The effect is specific to LDL cholesterol (and apolipoprotein B-containing particles); HDL is typically unaffected or modestly preserved
- The effect requires sustained consumption — bile-acid trapping is an ongoing process, and serum cholesterol returns to baseline within weeks of discontinuation
- The effect is additive with other LDL-lowering interventions (statins, dietary changes, other soluble fibers)
Fenugreek galactomannan fits into this framework alongside oat beta-glucan, psyllium husk, glucomannan (konjac), and the legume polysaccharides — all of which deliver this same mechanism with varying efficiency.
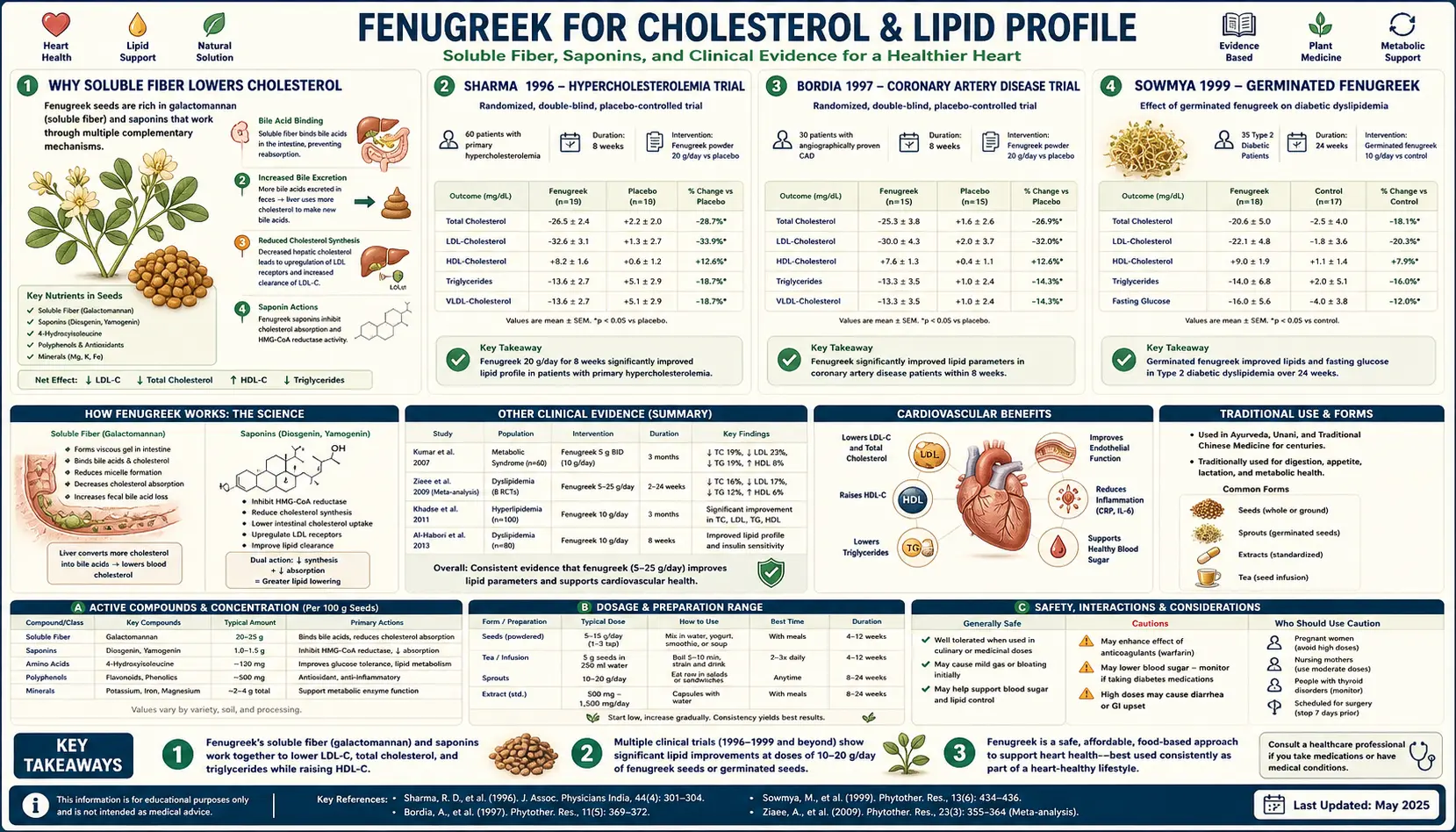
The Sharma 1996 Hypercholesterolemia Trial
The Sharma et al. 1996 study published in Phytotherapy Research is the foundational clinical evidence for fenugreek's cholesterol-lowering effect. The design followed the same metabolic-ward template Sharma's group had used for their landmark 1990 diabetes trial: 100 g/day of defatted fenugreek seed powder incorporated into chapati, given for 24 weeks to type 2 diabetic patients with concurrent hypercholesterolemia.
Results at 24 weeks:
- Total cholesterol reduced by approximately 18-30% (varying by patient subgroup), with the largest effect in patients with highest baseline cholesterol
- LDL cholesterol reduced by approximately 35% on average
- VLDL cholesterol reduced by approximately 27%
- HDL cholesterol — preserved or modestly increased
- Triglycerides reduced by approximately 16-30%
- Total cholesterol:HDL ratio improved substantially — the most clinically relevant single metric for cardiovascular risk
- Concurrent improvements in fasting glucose (per the earlier Sharma 1990 mechanism)
- No clinically significant adverse events beyond gastrointestinal complaints in the first 1-2 weeks
The Sharma 1996 effect is impressive in magnitude — an LDL reduction of 35% is in the same range as a moderate-intensity statin — but the practical limitation remains the 100 g/day dose. Three heaping tablespoons of fenugreek seed powder daily is achievable in a metabolic-ward study where the investigators control the entire diet, but it is not realistic for free-living patients managing their own meals. The bulk and the maple-syrup body odor and the gastrointestinal effects make this dose extraordinarily difficult to sustain in real-world settings.
Subsequent trials have worked downward to find the minimum effective dose. The 5-25 g/day range that produces the bulk of the glycemic benefit produces a smaller but still detectable cholesterol effect — on the order of 5-15% LDL reduction in most trials.
The Bordia 1997 Coronary Artery Disease Trial
The Bordia et al. 1997 trial in Prostaglandins, Leukotrienes and Essential Fatty Acids moved the question into the cardiovascular disease population. The design enrolled 60 patients with documented coronary artery disease and concurrent type 2 diabetes, randomizing them to fenugreek powder, ginger powder, or placebo, daily for three months.
Findings in the fenugreek arm versus placebo:
- Total cholesterol — significant reduction
- Triglycerides — significant reduction
- Fasting blood glucose — significant reduction (consistent with the established glycemic mechanism)
- Platelet aggregation — modest reduction (suggesting an additional antiplatelet effect that may contribute to cardiovascular benefit independently of lipid changes)
- Ginger showed antiplatelet effects but smaller lipid effects than fenugreek
The Bordia trial is important because it documents a multi-mechanism cardiovascular signal — fenugreek not only lowered lipids but also showed mild antiplatelet activity, both of which would be expected to contribute to reduced cardiovascular events over the long term. The trial was not powered to detect hard clinical endpoints (myocardial infarction, stroke, cardiovascular mortality), but it laid groundwork for the hypothesis that fenugreek may have cardiovascular benefits beyond what serum lipid measurement alone captures.
Sowmya 1999: Germinated Fenugreek
The Sowmya and Rajyalakshmi 1999 study in Plant Foods for Human Nutrition introduced a useful preparation variation: germinated fenugreek seed (the seed sprouted for 48-72 hours before consumption). The hypothesis was that germination would increase bioavailability of certain components and possibly enhance the cholesterol-lowering effect. The design was an eight-week trial in 20 hypercholesterolemic but non-diabetic adults, given 12.5 g of germinated fenugreek seed twice daily (25 g total daily).
Results:
- Total cholesterol reduced significantly
- LDL cholesterol reduced significantly
- HDL cholesterol increased modestly
- Triglycerides reduced
- Effect was achieved at 25 g/day — substantially less than the 100 g/day used by Sharma in 1996
- Subjects reported the germinated preparation was easier to consume than dry-seed powder, with less gastrointestinal distress
The germination concept is practically interesting because it makes the higher fenugreek doses more palatable. Germination is also straightforward to do at home — the seeds are soaked overnight, drained, kept moist in a sprouting jar for 48-72 hours, and consumed when small white sprouts emerge. The sprouts have a milder flavor than dry seeds and can be added to salads, eggs, or soups.
Geberemeskel 2019: Glycemic + Lipid Combined
The Geberemeskel et al. 2019 trial in the Journal of Diabetes Research documented the combined glycemic and lipid effects in a single type 2 diabetic patient population, providing the best modern picture of fenugreek's dual metabolic action at a practical dose. The intervention was 25 g/day of fenugreek seed powder for 60 days in 114 newly-diagnosed type 2 diabetic patients.
Results at 60 days:
- Fasting blood glucose — significant reduction
- HbA1c — significant reduction
- Total cholesterol — significant reduction (approximately 10-15%)
- LDL cholesterol — significant reduction (approximately 12-18%)
- Triglycerides — significant reduction
- HDL cholesterol — modest increase
- Atherogenic index (total cholesterol:HDL ratio) — significantly improved
- No significant adverse events
The Geberemeskel trial is the most practically useful single source for predicting what a typical patient will experience: a 25 g/day fenugreek seed regimen for 8-10 weeks produces meaningful improvements in both glycemic and lipid markers, with effect sizes that are modest individually but cumulatively impressive for a single inexpensive food intervention.
The Galactomannan Bile-Acid Binding Mechanism
The dominant soluble fiber in fenugreek seed is galactomannan, a polysaccharide with a backbone of (1-4)-linked beta-D-mannose units bearing single alpha-D-galactose side chains at a ratio of approximately 1:1 (mannose:galactose). This 1:1 ratio is unusually high among commercial galactomannans — guar gum has a 2:1 mannose:galactose ratio, locust bean gum has a 4:1 ratio. The higher galactose substitution in fenugreek galactomannan gives it greater water solubility and a different viscosity profile than its commercial cousins.
The bile-acid binding mechanism unfolds as follows:
- Fenugreek seed is consumed with or near a meal containing fat
- The galactomannan hydrates in the stomach and small intestine, forming a viscous gel
- Cholecystokinin from the duodenum stimulates gallbladder contraction and bile release into the small intestine
- The bile acids (primarily cholic acid and chenodeoxycholic acid and their glycine and taurine conjugates) emulsify dietary fat into micelles for digestion
- Normally, these bile acids would be reabsorbed in the terminal ileum via the sodium-dependent bile acid transporter (ASBT) and returned to the liver
- With galactomannan present, a fraction of the bile acids are physically trapped in the gel matrix and carried distally beyond the absorption window
- The trapped bile acids are excreted in stool, increasing fecal bile acid output by 20-40% in the typical fenugreek-fed individual
- The liver, sensing reduced returning bile acid pool, upregulates CYP7A1 (cholesterol 7-alpha-hydroxylase), the rate-limiting enzyme in bile acid synthesis from cholesterol
- The increased hepatic bile acid synthesis consumes hepatic cholesterol
- To replenish the cholesterol pool, the liver upregulates LDL receptor expression and pulls more LDL particles out of circulation
- Serum LDL cholesterol concentration falls
This is the same mechanism with only minor variations as for oat beta-glucan, psyllium mucilage, and pharmaceutical cholestyramine. The relative efficiency varies — psyllium and cholestyramine bind bile acids more efficiently per gram, while oat beta-glucan and fenugreek galactomannan have a milder taste and more palatable mouth feel.
LDL Reduction with Preserved HDL
One of the favorable features of the bile-acid-binding mechanism is that it preferentially affects the atherogenic LDL particle pool while leaving HDL essentially unaffected. Across the fenugreek trials, the typical pattern is:
- LDL cholesterol — reduced by 10-35% depending on dose and baseline
- Total cholesterol — reduced by 10-30%
- VLDL cholesterol and triglycerides — reduced modestly (likely via a different mechanism, possibly involving the soluble-fiber-driven attenuation of postprandial hyperinsulinemia)
- HDL cholesterol — preserved, or in some trials modestly increased
- Total cholesterol:HDL ratio — improved (the most cardiovascular-risk-predictive single lipid metric)
- Apolipoprotein B — reduced (the underlying atherogenic particle concentration)
This is a more favorable lipid profile change than is achieved with some dietary interventions (e.g., low-fat diets, which can reduce both LDL and HDL and worsen the ratio). It is similar in pattern to the effect of moderate-intensity statin therapy, oat beta-glucan, or psyllium husk — all of which preserve HDL while reducing LDL.
Fenugreek Galactomannan vs Oat Beta-Glucan vs Psyllium
A practical question for any patient considering soluble fiber for cholesterol management is how fenugreek compares to its better-established competitors:
- Oat beta-glucan — perhaps the most-studied soluble fiber for cholesterol. The FDA has granted a health claim for oat beta-glucan: 3 g/day reduces total cholesterol by approximately 4% and LDL by approximately 6-8%. Easy to consume as oatmeal or rolled oats; bland, well-tolerated, widely available. The clinical-trial-validated reference standard for botanical soluble-fiber cholesterol management
- Psyllium husk (Metamucil, generic) — the most efficient bile-acid binder per gram in the commercial botanical fiber category. 10 g/day reduces LDL by approximately 7-10%; 20 g/day reduces LDL by approximately 12-15%. Available as cheap generic powder. Some patients find the texture unpleasant; requires mixing with adequate water to avoid esophageal obstruction
- Glucomannan (konjac) — very viscous polysaccharide from konjac root; 3-4 g/day reduces LDL by approximately 10%. Often sold as a weight-loss aid. Requires consumption with adequate water for safety
- Fenugreek galactomannan — less efficient per gram than psyllium or glucomannan, comparable to or modestly more effective than oat beta-glucan. 15-25 g/day of fenugreek seed delivers roughly 7-12 g of soluble galactomannan and reduces LDL by approximately 8-15% per the modern trial literature. Has the advantage of concurrent glycemic and (in men) androgen-supportive effects from the other active compounds
For a patient whose primary goal is LDL reduction with minimal complications, psyllium husk at 10-20 g/day is the most efficient and best-validated option. For a patient with concurrent type 2 diabetes or pre-diabetes who wants metabolic benefit beyond cholesterol alone, fenugreek may be preferred. For most patients, a combination is reasonable — 5 g of psyllium husk plus 10-15 g of fenugreek seed daily delivers both mechanisms with less of either burden than the full effective dose of each alone.
The Dose Required: Higher Than for Glycemic Benefit
A practical observation across the published trial literature is that the dose of fenugreek required to produce a meaningful cholesterol effect is substantially higher than the dose required for the glycemic effect. This makes mechanistic sense:
- The glycemic effect is driven by 4-hydroxyisoleucine (active at relatively low milligram doses, present in standardized extracts) and to a secondary degree by the fiber-mediated slowing of carbohydrate absorption
- The cholesterol effect is driven almost entirely by the bulk fiber load and bile-acid binding, which requires a sustained gram-level intake of soluble fiber to be measurable
Rough dose-response for the cholesterol endpoint:
- 1-5 g/day of whole seed — no meaningful cholesterol effect
- 5-10 g/day of whole seed — small effect, sometimes detectable in larger trials but not robustly meaningful in individual patients
- 10-25 g/day of whole seed — modest reliable cholesterol effect, typically 5-12% LDL reduction
- 25-50 g/day of whole seed — larger effect, on the order of 10-20% LDL reduction, but with significant gastrointestinal burden and substantial maple-syrup body odor
- 100 g/day (Sharma 1996 dose) — 25-35% LDL reduction, but essentially impractical outside a research setting
For a patient pursuing fenugreek specifically for cholesterol benefit, the practical minimum effective dose is approximately 15 g/day of whole seed — three heaping teaspoons, taken in divided doses with meals. This is substantially more than most patients will sustain. The realistic positioning of fenugreek in cholesterol management is therefore as an adjunct to other measures (statins, oat-based diet, psyllium, dietary saturated-fat reduction), not as a standalone replacement for evidence-based pharmacotherapy in patients with clinically significant hypercholesterolemia.
Fenugreek vs Statin Therapy
The direct head-to-head comparison with statin therapy is informative:
- Low-intensity statin (rosuvastatin 5 mg, atorvastatin 10 mg, simvastatin 10 mg) — LDL reduction approximately 30-40%
- Moderate-intensity statin (rosuvastatin 10 mg, atorvastatin 20-40 mg, simvastatin 20-40 mg) — LDL reduction approximately 30-50%
- High-intensity statin (rosuvastatin 20-40 mg, atorvastatin 40-80 mg) — LDL reduction approximately 50% or more
- Fenugreek 15-25 g/day — LDL reduction approximately 8-15%
- Sharma 1996 fenugreek 100 g/day — LDL reduction approximately 35%, comparable to a low-intensity statin
Statins also do something that fenugreek does not — they reduce cardiovascular events through mechanisms beyond LDL reduction (plaque stabilization, anti-inflammatory effects, endothelial function improvement). The hard-outcome cardiovascular evidence base for statins is unmatched by any nutritional intervention. For patients with established atherosclerotic cardiovascular disease, prior MI, or stroke, statin therapy is first-line and fenugreek would be an adjunct, not a substitute.
For patients with borderline-elevated LDL who do not yet meet criteria for statin therapy and who are looking for non-pharmaceutical management, fenugreek along with dietary modification and other soluble fibers can be a reasonable approach. The risk-benefit balance depends heavily on the patient's overall cardiovascular risk profile, family history, and other risk factors.
Practical Use: Combining With Diet and Other Fibers
- Realistic fenugreek dose — 5 g (one teaspoon) of soaked whole seed in the morning, plus 5-10 g additional with the largest meal of the day. Total 10-15 g/day. This will deliver a modest cholesterol effect plus the documented glycemic and metabolic benefits
- Combine with oat-based breakfast — oatmeal or steel-cut oats with a tablespoon of ground flaxseed and chopped soaked fenugreek seed in the morning delivers a coordinated soluble-fiber load that is much greater than fenugreek alone
- Combine with psyllium husk — 5 g of psyllium in water before the largest meal of the day plus fenugreek with the meal is a useful combination that delivers two complementary soluble fibers
- Combine with dietary changes — reduction of saturated fat intake, replacement of refined carbohydrates with whole grains and legumes, and inclusion of nuts (almonds, walnuts) all contribute to a coordinated dietary approach that produces effects larger than any single intervention
- Lipid panel monitoring — check baseline lipid panel before starting; recheck at 8-12 weeks. Realistic expected effect from fenugreek alone at sustainable doses: 5-15% LDL reduction. Larger effects suggest concurrent dietary improvement is contributing
- For patients already on statin therapy — fenugreek as adjunct is reasonable and may allow lower statin doses in patients who are statin-sensitive (myalgia, hepatic transaminase elevation). Monitor lipids and discuss any dose adjustment with the prescribing clinician
- For patients pursuing strict non-pharmaceutical management — fenugreek (15-25 g/day) plus oat or psyllium fiber (10-15 g/day) plus dietary saturated-fat reduction plus regular exercise can achieve LDL reductions on the order of 20-30%. This is comparable to a low-intensity statin and may be sufficient for patients with modest baseline elevation and otherwise favorable risk profile
Cautions and Drug Interactions
- Pregnancy — absolute contraindication for medicinal doses (uterotonic activity)
- Warfarin interaction — check INR more frequently for the first month after starting
- Diabetes medication interaction — same caveat as on the Blood Sugar page; combined glucose-lowering may require insulin or sulfonylurea dose reduction
- Reduced absorption of co-administered medications — this is the most under-appreciated soluble-fiber drug interaction. Viscous galactomannan can reduce the absorption of co-administered oral medications by trapping them in the intestinal gel. This is particularly relevant for narrow-therapeutic-index drugs (levothyroxine, warfarin, digoxin, lithium) and for drugs requiring rapid absorption. The mitigation is to separate fenugreek and other oral medications by at least 2-4 hours
- Reduced absorption of fat-soluble vitamins — sustained high-dose soluble fiber can modestly reduce absorption of vitamins A, D, E, and K. Not usually clinically meaningful at the doses typically used for cholesterol benefit, but worth noting for patients with established fat-soluble vitamin deficiency or fat malabsorption
- Maple-syrup body odor — per the other Fenugreek Benefits pages, this is the most-discussed cosmetic side effect, more pronounced at the higher doses used for cholesterol benefit
- Gastrointestinal effects — gas, bloating, cramping, and loose stools in the first 1-2 weeks; usually resolves with continued use. Increasing the dose gradually (starting at 5 g/day and titrating up over 2-3 weeks to the target dose) reduces this
- Hypoglycemia in non-diabetic patients — possible at the higher fiber doses used for cholesterol benefit, particularly if fenugreek is taken without food. Take with meals
- Legume allergy and cross-reactivity — documented cross-reactivity with peanut, chickpea, soy, and lentil
Key Research Papers
- Sharma RD, Sarkar A, Hazra DK et al. (1996). Hypolipidaemic effect of fenugreek seeds: a chronic study in non-insulin dependent diabetic patients. Phytotherapy Research 10:332-334. — PubMed
- Bordia A, Verma SK, Srivastava KC (1997). Effect of ginger and fenugreek on blood lipids, blood sugar and platelet aggregation in patients with coronary artery disease. Prostaglandins, Leukotrienes and Essential Fatty Acids 56:379-384. — PubMed
- Sowmya P, Rajyalakshmi P (1999). Hypocholesterolemic effect of germinated fenugreek seeds in human subjects. Plant Foods for Human Nutrition 53:359-365. — PubMed
- Geberemeskel GA et al. (2019). Effect of fenugreek seed powder intake on glycemic control and lipid profile of type 2 diabetic patients. Journal of Diabetes Research 2019:8507453. — PubMed
- Sharma RD, Raghuram TC, Rao NS (1990). Effect of fenugreek seeds on blood glucose and serum lipids in type I diabetes. European Journal of Clinical Nutrition 44:301-306. — PubMed
- Khosla P et al. (1995). Effect of Trigonella foenum-graecum on serum lipids in normal and diabetic rats. Indian Journal of Pharmacology. — PubMed
- Belguith-Hadriche O et al. (2010). Antihyperlipidemic and antioxidant activities of edible Tunisian Trigonella foenum-graecum. Plant Foods for Human Nutrition 65:434-440. — PubMed
- Boban PT et al. (2009). Hypolipidaemic effect of chemically different mucilages in rats: a comparative study. British Journal of Nutrition. — PubMed
- Roberts KT (2011). The potential of fenugreek (Trigonella foenum-graecum) as a functional food and nutraceutical and its effects on glycemia and lipidemia. Journal of Medicinal Food 14:1485-1489. — PubMed
- Ramulu P, Giridharan NV, Udayasekhararao P (2011). Hypolipidemic effect of soluble dietary fiber (galactomannan) isolated from fenugreek seeds in WNIN/Gr-Ob obese rats. Indian Journal of Medical Research. — PubMed
- Skim F et al. (1999). Cholesterol-lowering and lipid-modulating effects of fenugreek seed powder. — PubMed
- Mukthamba P, Srinivasan K (2015). Hypolipidemic and antioxidant effects of dietary fenugreek (Trigonella foenum-graecum) seeds and garlic (Allium sativum) in high-fat fed rats. Food Bioscience. — PubMed
PubMed Topic Searches
- PubMed: Fenugreek cholesterol/LDL trials
- PubMed: Galactomannan bile-acid binding
- PubMed: Soluble fiber LDL mechanism
- PubMed: Fenugreek triglyceride / atherogenic index
- PubMed: Oat beta-glucan vs psyllium cholesterol
Connections
- Fenugreek Overview
- Fenugreek Benefits Hub
- Fenugreek for Blood Sugar
- Fenugreek for Testosterone
- Fenugreek for Lactation
- Hypertension
- Lipid Panel
- Apolipoprotein B
- Oats (Beta-Glucan)
- Garlic
- Turmeric
- Berberine
- Omega-3 Fatty Acids
- Blood Sugar Control
- Type 2 Diabetes
- All Herbs