Fenugreek for Blood Sugar & Type 2 Diabetes
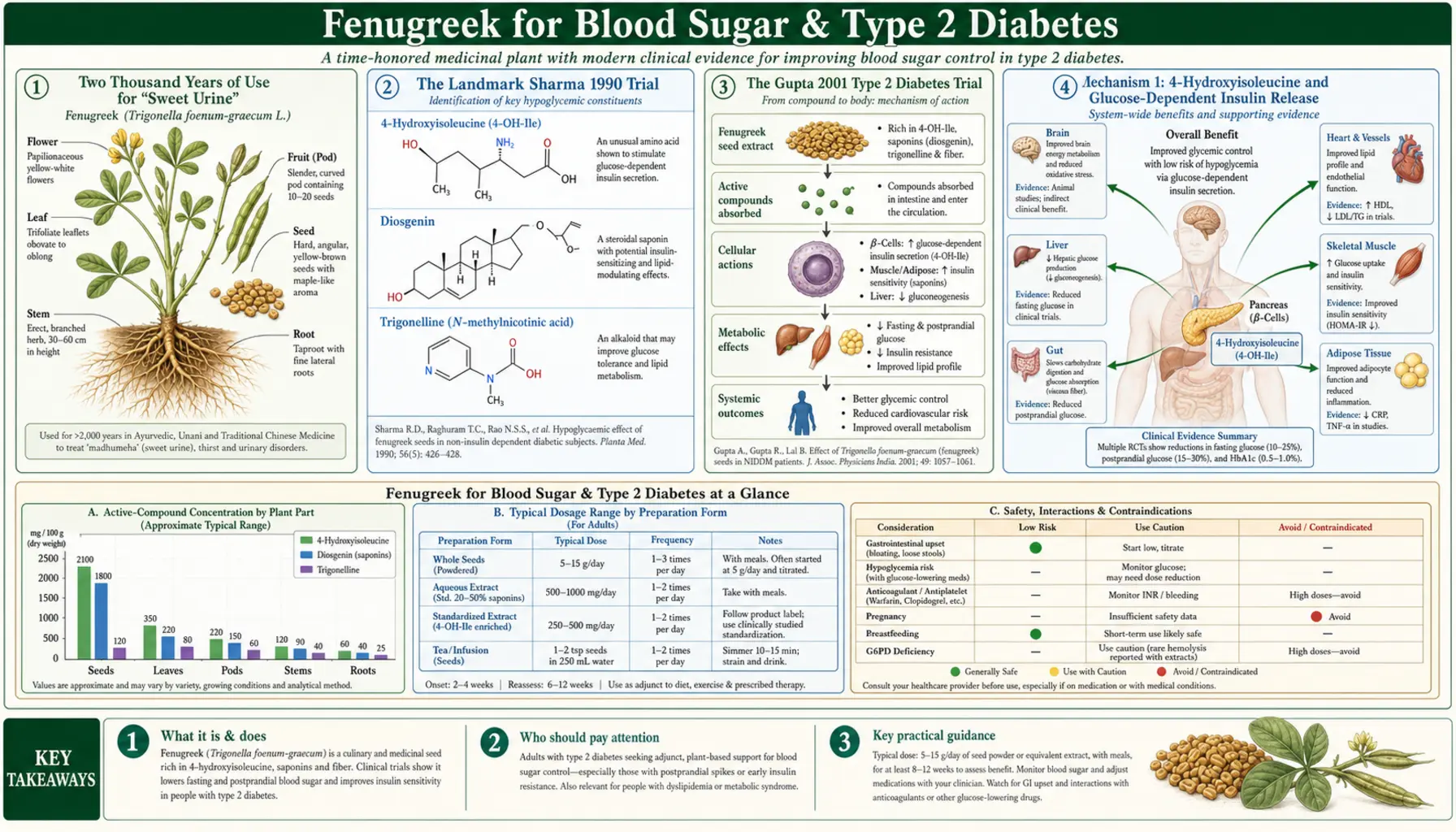
Fenugreek seed has been used continuously in traditional Indian, Egyptian, and Middle Eastern medicine for "sweet urine" (the ancient description of diabetes) for at least two thousand years, and the modern randomized-trial literature has confirmed a clinically meaningful glycemic effect. The defining study is still Sharma et al. 1990, which used 100 g of defatted fenugreek seed powder daily in newly-diagnosed type 2 diabetic patients and dropped fasting plasma glucose from a baseline near 151 mg/dL to roughly 112 mg/dL by week eight. The Gupta 2001 follow-up at a more practical 25 g/day dose confirmed the effect in a randomized double-blind setting. The mechanism is now well-characterized as a dual action: 4-hydroxyisoleucine, a non-protein amino acid unique to fenugreek, directly stimulates pancreatic beta-cell insulin release in a glucose-dependent manner, while the seed's viscous galactomannan fiber slows gastric emptying and carbohydrate absorption. This page walks through every clinical trial of note, contrasts fenugreek with metformin and sulfonylureas, and lays out the practical 5-25 g/day dose-response curve along with the specific situations where fenugreek is most and least likely to help.
Table of Contents
- Two Thousand Years of Use for "Sweet Urine"
- The Landmark Sharma 1990 Trial
- The Gupta 2001 Type 2 Diabetes Trial
- Mechanism 1: 4-Hydroxyisoleucine and Glucose-Dependent Insulin Release
- Mechanism 2: Galactomannan Fiber and Carbohydrate Absorption
- The 5-25 g/day Dose-Response Curve
- Meta-Analyses: What the Pooled Evidence Says
- Fenugreek vs Metformin: Head-to-Head and Adjunct
- Prediabetes: The Gaddam 2015 Prevention Trial
- Practical Use: Form, Timing, and Monitoring
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
Two Thousand Years of Use for "Sweet Urine"
Fenugreek (Trigonella foenum-graecum) is one of the oldest cultivated plants in continuous medicinal use. Charred seeds have been recovered from Tutankhamun's tomb (circa 1320 BCE), and the Ebers Papyrus (circa 1550 BCE) describes a fenugreek preparation for what would today be recognized as a wasting/polyuric condition consistent with diabetes mellitus. In Indian Ayurveda, methi seeds appear in formulations for "madhumeha" (literally "sweet urine") in the Charaka Samhita and Sushruta Samhita, both compiled in the early centuries CE. In Greco-Arab Unani medicine, fenugreek (hulba) was a primary agent for "ziyabetis" — the same Greek root that gave us "diabetes."
Modern interest began in the 1930s and accelerated dramatically after the Sharma group at the National Institute of Nutrition in Hyderabad, India, published their first metabolic ward studies in the late 1980s. Today fenugreek is one of only a handful of botanical agents (alongside berberine, bitter melon, and gymnema) with multiple randomized controlled trials supporting a clinically meaningful glycemic effect.
The Landmark Sharma 1990 Trial
Sharma, Raghuram, and Rao's 1990 paper in the European Journal of Clinical Nutrition remains the single most-cited fenugreek diabetes trial and the one that put fenugreek on the modern medical map. The design was a metabolic-ward crossover study in newly-diagnosed type 2 diabetic patients who had not yet started any oral antidiabetic medication. The intervention period used 100 g of defatted fenugreek seed powder incorporated into unleavened bread (chapati), divided into two equal meals daily, for eight weeks. The control period used isocaloric matched bread without fenugreek.
The headline results were striking:
- Fasting plasma glucose fell from a baseline mean of approximately 151 mg/dL to approximately 112 mg/dL by week 8 of the fenugreek period — a reduction of about 40 mg/dL, or roughly 27% from baseline
- The oral glucose tolerance test (OGTT) area under the curve fell substantially, with the 2-hour postprandial glucose dropping by roughly 30%
- 24-hour urinary glucose excretion dropped by approximately 54%, consistent with better overall glycemic control
- Serum total cholesterol fell by 22% and LDL by 33% — the first published evidence of fenugreek's lipid-lowering effect (covered in detail on the Cholesterol page)
- No adverse effects beyond mild gastrointestinal distress (flatulence, diarrhea in the first week) were reported
The major practical limitation of the Sharma 1990 trial is the dose — 100 g/day of fenugreek powder is approximately three heaping tablespoons, an essentially impractical daily intake for free-living patients outside a metabolic ward. The follow-up trials by Sharma and others worked downward from that dose to find the minimum effective intake.
The Gupta 2001 Type 2 Diabetes Trial
The Gupta, Gupta, and Lal trial published in the Journal of the Association of Physicians of India in 2001 brought the dose down to a clinically realistic 1 g/day of a hydroalcoholic fenugreek seed extract (equivalent to roughly 25 g of whole seed) and confirmed the effect in a properly randomized, double-blind, placebo-controlled design over two months in 25 newly-diagnosed type 2 diabetic patients. Results:
- Fasting blood glucose dropped from 148 to 119 mg/dL in the fenugreek arm versus essentially no change in placebo
- 2-hour postprandial glucose fell from 210 to 181 mg/dL in fenugreek versus no change in placebo
- HOMA-IR (insulin resistance index) improved by approximately 18% in fenugreek
- Serum insulin concentrations declined modestly — consistent with improved insulin sensitivity rather than insulin-secretagogue-like pancreatic stress
- Triglycerides and total cholesterol both fell significantly
- The placebo group showed no significant change on any endpoint
The Gupta 2001 paper is the more practically relevant of the two foundational trials because the dose — 1 g of extract or about 25 g of whole seed daily — is achievable for a motivated patient without converting their entire diet to fenugreek bread.
Mechanism 1: 4-Hydroxyisoleucine and Glucose-Dependent Insulin Release
The most distinctive feature of fenugreek's glycemic mechanism is the non-protein amino acid 4-hydroxyisoleucine (4-HI), which is present in fenugreek seeds at approximately 0.55% by dry weight and in essentially no other common food in pharmacologically meaningful quantity. Sauvaire and colleagues at the University of Montpellier published the definitive characterization of 4-HI's insulinotropic effect in Diabetes in 1998. Their isolated rat and human pancreatic islet studies demonstrated:
- 4-HI directly stimulates pancreatic beta-cell insulin secretion in vitro
- The stimulation is strictly glucose-dependent — 4-HI amplifies insulin release at elevated glucose concentrations (6.6 mmol/L and above) but does not increase insulin secretion at basal glucose (3.3 mmol/L)
- The effect is dose-dependent across a physiologically relevant concentration range
- The mechanism is mediated by a direct effect on the beta cell, independent of the autonomic nervous system or gastrointestinal hormones
This glucose-dependent mechanism is a major clinical advantage over sulfonylurea drugs (glipizide, glyburide, glimepiride), which stimulate insulin release through the K-ATP channel regardless of ambient glucose and therefore carry a real risk of hypoglycemia. 4-HI's glucose-dependent action means fenugreek tends to amplify the normal physiological insulin response to a meal rather than provoke insulin release between meals. This is the same fundamental property that makes the GLP-1 agonists (liraglutide, semaglutide) and DPP-4 inhibitors (sitagliptin) clinically attractive — effective glucose lowering without iatrogenic hypoglycemia.
The clinical caveat is that 4-HI's effect at typical dietary fenugreek doses is modest. Mechanistically the molecule is interesting; quantitatively, fenugreek delivers far less 4-HI than a therapeutic dose of a pharmaceutical insulin secretagogue, and the bulk of the seed's glycemic effect at typical doses likely comes from the second mechanism — galactomannan fiber.
Mechanism 2: Galactomannan Fiber and Carbohydrate Absorption
Fenugreek seed is approximately 45-50% total dietary fiber, of which roughly half is soluble. The dominant soluble fiber is a viscous galactomannan polysaccharide structurally similar to guar gum, with a mannose:galactose ratio of roughly 1:1. When fenugreek seed is consumed, this galactomannan hydrates in the stomach and forms a viscous gel with two major glycemic consequences:
- Delayed gastric emptying — the viscous gel slows the release of carbohydrate-containing chyme into the small intestine, which flattens the postprandial glucose curve and reduces the magnitude of the peak
- Reduced rate of glucose absorption — even after gastric emptying, the viscous unstirred water layer in the small intestine slows the diffusion of glucose to the brush-border enterocyte transporters (SGLT1 and GLUT2), further attenuating the postprandial glucose excursion
This is fundamentally the same mechanism by which oat beta-glucan, psyllium husk, guar gum, and (in pharmaceutical form) acarbose work to attenuate postprandial glucose. The clinical implication is that fenugreek's glycemic effect is dose-dependent and time-dependent in a fiber-typical way — the seed needs to be consumed with or just before the carbohydrate-containing meal to deliver maximum benefit, and the dose required to see a meaningful effect on fasting glucose and HbA1c is in the 10-25 g/day range, which is substantially more than the dose required for the 4-HI insulinotropic effect.
For patients who cannot tolerate the gastrointestinal load of 25 g of whole fenugreek seed daily, the practical compromise is either a smaller dose of whole seed combined with other soluble fibers like psyllium or oat, or a standardized fenugreek extract enriched for 4-HI (typically labeled as "Furosap" or "Testofen" depending on the brand) at a much lower daily milligram dose. The latter provides less fiber-based glycemic benefit but is easier to take consistently.
The 5-25 g/day Dose-Response Curve
Pooling the published clinical trial data, a rough dose-response curve emerges:
- 1-5 g/day of whole seed — insufficient fiber load to meaningfully affect fasting glucose or HbA1c in established type 2 diabetes. May still provide modest postprandial glucose attenuation if consumed immediately before a high-carbohydrate meal
- 5-10 g/day of whole seed — consistent modest reduction in postprandial glucose; small but measurable reduction in fasting glucose and HbA1c in some trials; well-tolerated by most patients without major gastrointestinal distress
- 10-25 g/day of whole seed — the dose range that consistently produces clinically meaningful reductions in fasting glucose (typically 15-30 mg/dL), 2-hour postprandial glucose, and HbA1c (typically 0.3-0.7 percentage points) in type 2 diabetic patients across the published trials. This is the dose range that requires patient counseling about the expected maple-syrup body odor and gastrointestinal effects
- 25-100 g/day of whole seed — the dose range used in the original Sharma 1990 metabolic-ward studies. Produces larger effects but is essentially impractical outside a research setting, with substantial gastrointestinal distress reported by most patients
- 500-1,000 mg/day of standardized hydroalcoholic extract (Gupta 2001 dose) — equivalent to roughly 25 g of whole seed for the soluble components but with much less fiber load. Effective on fasting glucose and HbA1c, with much better tolerability
For most patients with type 2 diabetes or prediabetes, the practical starting point is 5 g of whole seed twice daily (one teaspoon, soaked overnight per the canonical 8-12 hour preparation on the main Fenugreek page), titrating up to 10 g twice daily if tolerated.
Meta-Analyses: What the Pooled Evidence Says
Three major meta-analyses have pooled the fenugreek glycemic trial literature: Neelakantan 2014 (10 trials, 386 patients), Suksomboon 2011 (a smaller earlier pooling), and Hassani 2019 (a systematic review without quantitative pooling). The Neelakantan analysis, published in Nutrition Journal, is the most rigorous of the three and the most commonly cited.
Pooled results from Neelakantan 2014:
- Fasting plasma glucose reduction of approximately 0.96 mmol/L (~17 mg/dL) versus control in patients with type 2 diabetes
- 2-hour postprandial glucose reduction of approximately 2.19 mmol/L (~39 mg/dL)
- HbA1c reduction in the range of 0.85 percentage points where it was measured
- The effect was largest at higher doses (>5 g/day of whole seed) and in patients with worse baseline glycemic control
- The effect on patients with prediabetes or impaired fasting glucose was smaller but still statistically significant
For context, a 0.85 percentage point reduction in HbA1c is in the range of effect seen with low-dose metformin (500 mg/day) or with the addition of a DPP-4 inhibitor — clinically meaningful but not on the scale of full-dose metformin (1.5-2.0 g/day) or insulin therapy. Fenugreek is best understood as a useful adjunct to first-line therapy rather than a standalone replacement for pharmacological management of established type 2 diabetes.
Fenugreek vs Metformin: Head-to-Head and Adjunct
The direct head-to-head comparison with metformin is informative. Metformin at 1.5-2.0 g/day typically reduces HbA1c by 1.0-1.5 percentage points, fasting glucose by 50-80 mg/dL, and weight by 2-3 kg over 6-12 months. Fenugreek at 10-25 g/day reduces HbA1c by 0.3-0.85 points, fasting glucose by 15-30 mg/dL, and has neutral or slightly favorable effects on weight.
Mechanistically the two are partially complementary — metformin's primary action is hepatic gluconeogenesis suppression and modest peripheral insulin sensitization, while fenugreek's primary actions are pancreatic insulin amplification (4-HI) and carbohydrate absorption modulation (galactomannan). They target different points in the glucose-disposal pathway, so concurrent use is biologically reasonable. The Bordia 1997 trial and several smaller adjunct studies show additive effects when fenugreek is added to existing oral antidiabetic therapy.
Practical clinical positioning:
- Newly-diagnosed type 2 diabetes with HbA1c 6.5-7.5% — fenugreek alone (along with diet and exercise) is a reasonable first-line trial before initiating metformin, particularly for patients reluctant to start medication. Recheck HbA1c at 3 months; if still above target, initiate metformin and continue fenugreek as adjunct
- Established type 2 diabetes on metformin not at target — fenugreek as adjunct is biologically rational and well-supported. Expect HbA1c reduction of roughly 0.3-0.7 points
- Type 2 diabetes on insulin — fenugreek can be added but glucose monitoring needs to be more careful in the first weeks, as the combined glucose-lowering may require insulin dose reduction
- Type 2 diabetes on sulfonylurea — concurrent use is theoretically more concerning for hypoglycemia, though the 4-HI glucose-dependent mechanism mitigates this. Still, monitor closely and consider dose-reducing the sulfonylurea
- Prediabetes — fenugreek is reasonable preventive nutrition, with the Gaddam 2015 trial showing meaningful prevention of progression to diabetes over three years
Prediabetes: The Gaddam 2015 Prevention Trial
The Gaddam 2015 trial in the Journal of Diabetes and Metabolic Disorders is the most important prediabetes-specific fenugreek study and the one that bridges the gap between symptomatic diabetes treatment and primary prevention. The design enrolled 140 patients with prediabetes (impaired fasting glucose 100-125 mg/dL or impaired glucose tolerance) and randomized them to either 5 g of whole fenugreek seed powder twice daily plus lifestyle counseling, or lifestyle counseling alone, for three years.
The progression-to-diabetes endpoint was striking:
- Progression to diabetes at three years — approximately 4.2% in the fenugreek arm versus 25.7% in the control arm
- This translates to a relative risk reduction of approximately 84% for the fenugreek arm, and an absolute risk reduction of approximately 21 percentage points
- Number needed to treat (NNT) to prevent one case of diabetes over 3 years was approximately 5
- Fasting glucose, postprandial glucose, and HbA1c all improved more in the fenugreek arm
- Lipid profile (LDL, total cholesterol, triglycerides) also improved more in the fenugreek arm
For context, the major lifestyle-intervention prediabetes trials (DPP, Finnish DPS) showed risk reductions of approximately 58% with intensive diet-and-exercise counseling, and metformin in DPP showed risk reduction of approximately 31%. The Gaddam fenugreek effect is in the same range as the DPP lifestyle intervention, which is a very strong showing for a single-botanical intervention. The trial is limited by being a single-center study without independent replication at this scale, but it remains a hopeful signal for fenugreek as a prediabetes preventive.
Practical Use: Form, Timing, and Monitoring
For patients pursuing fenugreek for glycemic benefit:
- Form — whole soaked seed is the canonical form and the form used in most positive clinical trials. Powdered fenugreek (sold as the spice in any grocery store) is the next most-studied form. Capsulated standardized extracts (Furosap, Testofen) are easier to take but provide less fiber-based glycemic benefit. Defatted fenugreek seed powder used in the Sharma 1990 trial is rarely sold commercially but can be produced at home by extracting whole seed powder briefly with a food-grade solvent and drying
- Soaking — the canonical 8-12 hour overnight cold-water soak described on the main Fenugreek page maximizes extraction of the soluble components without destroying the heat-sensitive 4-HI. Boiling water destroys 60-70% of the soluble actives
- Timing — the soaked-seed water and chewed seeds should be consumed first thing in the morning on an empty stomach for maximum 4-HI absorption. For fiber-based postprandial glucose attenuation, a second dose immediately before the largest carbohydrate meal of the day adds additional benefit
- Monitoring — check fasting glucose weekly for the first month, then monthly. Check HbA1c at 3 months. For patients on insulin or sulfonylureas, more frequent home glucose monitoring is warranted in the first two weeks to detect any combined hypoglycemic effect
- Realistic expectations — for a typical type 2 diabetic patient with HbA1c 7.5-8.5% on metformin alone, adding fenugreek at 10-15 g/day should reduce HbA1c by approximately 0.3-0.7 percentage points over 3 months. This is meaningful but not transformative
Cautions and Drug Interactions
- Pregnancy — absolute contraindication — fenugreek has documented uterotonic activity (it stimulates uterine smooth muscle contraction) and is traditionally used in late pregnancy in some cultures to induce labor. High-dose fenugreek in early or mid pregnancy carries a theoretical risk of miscarriage. Pregnant women should avoid medicinal fenugreek doses entirely, though small culinary amounts (as a spice in curry) are not concerning
- Warfarin — INR elevation — case reports document increased INR (excessive anticoagulation) in patients stably anticoagulated on warfarin who add fenugreek to their regimen. The mechanism is likely coumarin-related. Patients on warfarin should not start fenugreek without checking INR more frequently for the first 2-4 weeks and adjusting warfarin dose if needed
- Diabetes medications — additive hypoglycemic effect — combining fenugreek with insulin, sulfonylureas, or meglitinides can produce additive glucose-lowering. The risk of frank hypoglycemia is mitigated by 4-HI's glucose-dependent action but is not zero, particularly with sulfonylureas and insulin. More frequent home glucose monitoring is warranted in the first 2-4 weeks
- Maple-syrup body odor (sotolone) — the volatile lactone sotolone is excreted in sweat, urine, and (in lactating mothers) breast milk after fenugreek consumption. It produces a distinct sweet maple-syrup odor that is harmless but surprises patients who were not warned. The effect is dose-dependent and noticeable in most patients at doses above 10 g/day. Some patients consider this a deal-breaker; others find it inoffensive or even pleasant
- Legume allergy — chickpea and peanut cross-reactivity — fenugreek is a legume (family Fabaceae) and shares cross-reactive proteins with chickpea, peanut, soy, and lentil. Patients with documented peanut or chickpea allergy should approach fenugreek cautiously, ideally with allergist guidance
- Gastrointestinal distress — flatulence, abdominal distension, and loose stools are common in the first 1-2 weeks of fenugreek use and typically resolve. Starting at 2-3 g/day and titrating up over 2-3 weeks reduces this
- Subclinical hypoglycemia in non-diabetic users — healthy individuals taking fenugreek for non-glycemic purposes (testosterone, lactation) can experience mild hypoglycemic symptoms (lightheadedness, hunger, irritability) particularly if doses are taken on an empty stomach. Taking with food usually resolves this
Key Research Papers
- Sharma RD, Raghuram TC, Rao NS (1990). Effect of fenugreek seeds on blood glucose and serum lipids in type I diabetes. European Journal of Clinical Nutrition 44:301-306. — PubMed
- Gupta A, Gupta R, Lal B (2001). Effect of Trigonella foenum-graecum (fenugreek) seeds on glycaemic control and insulin resistance in type 2 diabetes mellitus: a double-blind placebo-controlled study. Journal of the Association of Physicians of India 49:1057-1061. — PubMed
- Sauvaire Y et al. (1998). 4-hydroxyisoleucine: a novel amino acid potentiator of insulin secretion. Diabetes 47:206-210. — PubMed
- Neelakantan N et al. (2014). Effect of fenugreek (Trigonella foenum-graecum) intake on glycemia: a meta-analysis of clinical trials. Nutrition Journal 13:7. — PubMed
- Madar Z et al. (1988). Glucose-lowering effect of fenugreek in non-insulin-dependent diabetics. European Journal of Clinical Nutrition 42:51-54. — PubMed
- Ranade M, Mudgalkar N (2017). A simple dietary addition of fenugreek seed leads to the reduction in blood glucose levels: a parallel group, randomized single-blind trial. Ayu 38:24-27. — PubMed
- Gaddam A et al. (2015). Role of fenugreek in the prevention of type 2 diabetes mellitus in prediabetes. Journal of Diabetes and Metabolic Disorders 14:74. — PubMed
- Bordia A, Verma SK, Srivastava KC (1997). Effect of ginger and fenugreek on blood lipids, blood sugar and platelet aggregation in patients with coronary artery disease. Prostaglandins, Leukotrienes and Essential Fatty Acids 56:379-384. — PubMed
- Geberemeskel GA et al. (2019). Effect of fenugreek seed powder intake on glycemic control and lipid profile of type 2 diabetic patients. Journal of Diabetes Research 2019:8507453. — PubMed
- Hassani SS et al. (2019). Hypoglycemic and antidiabetic effects of Trigonella foenum-graecum in diabetes: a systematic review. Journal of Diabetes Research. — PubMed
- Suksomboon N et al. (2011). Meta-analysis of the effect of herbal supplement on glycemic control in type 2 diabetes. Journal of Ethnopharmacology 137:1328-1333. — PubMed
- Basch E et al. (2003). Therapeutic applications of fenugreek. Alternative Medicine Review 8:20-27. — PubMed
PubMed Topic Searches
- PubMed: Fenugreek type 2 diabetes randomized trials
- PubMed: 4-Hydroxyisoleucine insulin secretion
- PubMed: Galactomannan postprandial glucose
- PubMed: Fenugreek HbA1c meta-analysis
- PubMed: Fenugreek prediabetes prevention
Connections
- Fenugreek Overview
- Fenugreek Benefits Hub
- Fenugreek for Testosterone
- Fenugreek for Lactation
- Fenugreek for Cholesterol
- Berberine
- Bitter Melon
- Gymnema
- Cinnamon
- Chromium
- Magnesium
- Type 2 Diabetes
- Hemoglobin A1C
- Fasting Insulin
- Continuous Glucose Monitor
- Blood Sugar Control
- Fasting
- All Herbs
- Metformin — the first-line drug fenugreek is sized against and most often added to.