Fennel for Menstrual and Menopausal Symptoms
Two of the better-quality clinical trials in the modern fennel literature address conditions at opposite ends of the reproductive timeline: Omidvar 2012 randomized women with primary dysmenorrhea (painful periods in young women without pelvic pathology) to fennel essential-oil capsules versus the NSAID mefenamic acid and found fennel matched the NSAID for pain control with fewer gastrointestinal side effects; Rahimikian 2017 randomized postmenopausal women with hot-flash and vaginal-atrophy complaints to soft-gel fennel 100 mg twice daily versus placebo and found significant reduction in menopause-symptom scores at 8 weeks. The unifying mechanism behind both effects is the phytoestrogenic activity of trans-anethole at the alpha-estrogen receptor — the same molecule that makes fennel a digestive aid and a galactagogue makes it a selective estrogen-receptor modulator (SERM) for the menstrual and menopausal complaint clusters. This deep-dive walks through the two pivotal trials, the SERM mechanism, the practical dose forms, the comparison to standard-of-care treatments, and the one major caution that recurs across the entire phytoestrogen literature: estrogen-sensitive cancers.
Table of Contents
- Two Domains, One Phytoestrogen Mechanism
- The SERM Mechanism — Anethole at the Estrogen Receptor
- Omidvar 2012 — Fennel vs Mefenamic Acid in Primary Dysmenorrhea
- Primary Dysmenorrhea — The Broader Fennel Evidence Base
- Rahimikian 2017 — Fennel for Menopausal Hot Flashes
- Menopause — Hot Flashes, Vaginal Atrophy, and Mood
- PCOS, Oligomenorrhea, and Amenorrhea
- Comparison to Standard-of-Care Treatments
- Practical Dose Forms (Decoction, Softgel, Standardized Extract)
- The Estrogen-Sensitive Cancer Caution
- Key Research Papers
- Connections
- Featured Videos
Two Domains, One Phytoestrogen Mechanism
The reproductive-medicine evidence for fennel sits in two apparently distinct domains separated by twenty to thirty years of a woman's life:
- Primary dysmenorrhea — painful menstrual cramps in young women (typically teenagers and women in their twenties) without an underlying structural cause such as endometriosis, fibroids, or pelvic inflammatory disease. Driven by excessive uterine production of inflammatory prostaglandins (particularly PGF2α) that produce strong uterine contractions and local ischemia. Standard of care: ibuprofen, naproxen, mefenamic acid, or combined hormonal contraceptives.
- Menopausal vasomotor symptoms — hot flashes, night sweats, sleep disruption, mood changes, vaginal atrophy with associated dryness and dyspareunia, urinary frequency, and bone-density loss following the ovarian estradiol decline. Standard of care: hormone replacement therapy (HRT) with estradiol ± progesterone for systemic symptoms, vaginal estrogen for genitourinary atrophy, SSRIs (paroxetine, venlafaxine) for vasomotor symptoms in women who cannot use HRT, and the newer non-hormonal NK3R antagonists (fezolinetant).
The fact that a single herb has measurable effect on both ends of the reproductive timeline points to a unifying mechanism. That mechanism is the selective estrogen receptor modulator (SERM) activity of trans-anethole: anethole binds the alpha-estrogen receptor (ERα) with low but measurable affinity and produces tissue-specific agonist or antagonist effects depending on the cellular context. The same compound can therefore:
- Reduce uterine prostaglandin production (the dysmenorrhea benefit) — estrogen modulates the prostaglandin synthesis pathway in endometrial tissue
- Partially substitute for the missing endogenous estradiol at the hypothalamic thermoregulatory center (the hot-flash benefit)
- Partially substitute at the vaginal epithelium (the atrophic vaginitis benefit)
- Maintain endometrial proliferation in oligomenorrhea (the menstrual-regularity benefit in some patients)
This is not a unique pharmacology — the same SERM concept underlies the pharmacology of tamoxifen and raloxifene (synthetic SERMs with ER-antagonist effect at breast tissue and ER-agonist effect at bone) and the broader phytoestrogen literature (soy isoflavones, red clover, hops, black cohosh).
The SERM Mechanism — Anethole at the Estrogen Receptor
The estrogen receptor exists in two principal subtypes: ERα (encoded by ESR1) and ERβ (encoded by ESR2). The two subtypes have overlapping but distinct tissue distributions and produce overlapping but distinct downstream transcriptional programs. Endogenous estradiol binds both with high affinity; selective receptor modulators bind preferentially to one or the other and produce tissue-specific effects depending on the local distribution of coactivator and corepressor proteins.
Trans-anethole binds both ERα and ERβ with low affinity — in receptor-binding assays, the EC50 is approximately 100-1,000 micromolar, which is roughly 1,000 to 10,000 times weaker than estradiol itself. This low binding affinity is what makes phytoestrogens generally well-tolerated: the cumulative agonist effect is modest, and the SERM-type tissue specificity is preserved because the partial-agonist effect depends heavily on local coactivator availability.
The downstream effects relevant to the menstrual and menopausal indications:
- Reduction of endometrial prostaglandin synthesis — estrogen receptor signaling modulates the expression of cyclooxygenase-2 (COX-2) and the downstream PGF2α pathway in endometrial tissue. The net effect of anethole-mediated partial agonism appears to reduce excessive PGF2α production in primary dysmenorrhea, with corresponding reduction in cramping pain.
- Direct uterine smooth-muscle relaxation — superimposed on the receptor-mediated effect is a direct calcium-channel-blocking effect of anethole on uterine smooth muscle (the same mechanism as the GI antispasmodic effect described on the digestive aid page). This contributes substantially to the rapid analgesic effect during an active dysmenorrhea episode.
- Hypothalamic thermoregulatory modulation — the postmenopausal hot flash is caused by hypothalamic temperature-regulation instability secondary to the loss of estradiol's tonic effect on the preoptic area. Partial agonist activity at hypothalamic ERα is hypothesized to be the mechanism by which phytoestrogens (including anethole) reduce hot-flash frequency.
- Vaginal epithelial proliferation — estrogen drives proliferation and maturation of vaginal epithelial cells; the post-menopausal estrogen-deficient state produces thinning, dryness, and dyspareunia. Topical and systemic phytoestrogens have measurable but modest effects on the vaginal maturation index.
Omidvar 2012 — Fennel vs Mefenamic Acid in Primary Dysmenorrhea
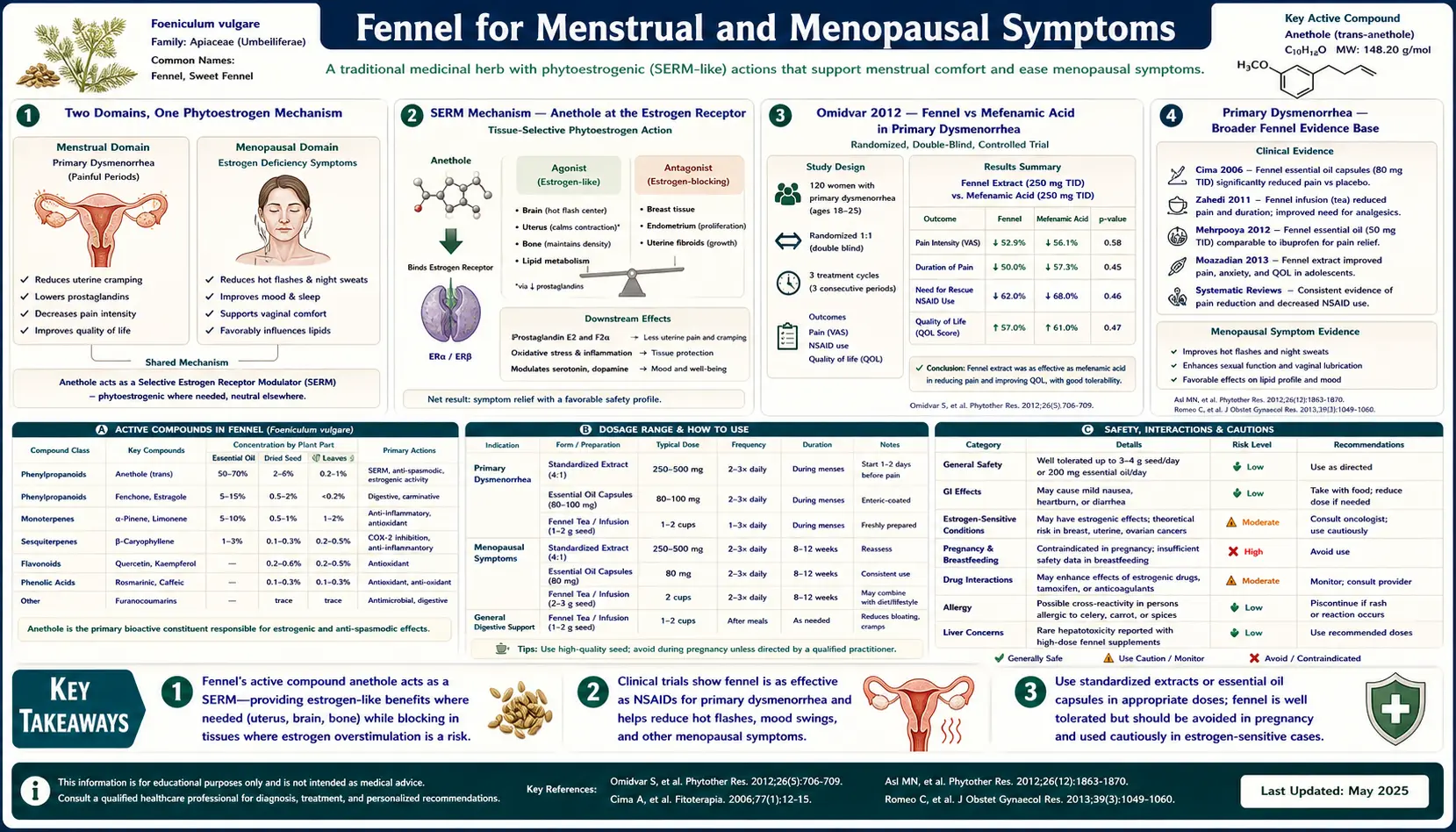
The most-cited modern trial of fennel for primary dysmenorrhea is Omidvar et al., titled "Crocus sativus and fennel essence vs. mefenamic acid in primary dysmenorrhea: a randomized clinical trial" (2012), published in the Journal of Caring Sciences. The study design:
- Population: young women with confirmed primary dysmenorrhea (without endometriosis or other structural pelvic pathology)
- Intervention: fennel essence capsules at 30 drops every 4 hours starting at the onset of menstrual pain
- Comparator: mefenamic acid 250 mg every 6 hours (mefenamic acid is a fenamate-class NSAID commonly used for dysmenorrhea, with strong analgesic effect but a significant GI side-effect profile)
- Outcome: pain reduction measured with a visual-analog pain scale
Key results:
- Fennel essence produced significant pain reduction comparable to mefenamic acid
- The pain reduction was clinically meaningful at the doses used — women in the fennel arm reported pain scores comparable to women in the mefenamic acid arm
- The fennel arm had a substantially lower rate of gastrointestinal side effects (nausea, dyspepsia) than the mefenamic acid arm — consistent with the well-known GI toxicity of NSAIDs versus the GI tolerability (indeed digestive benefit) of fennel
- No serious adverse events in either arm
The study has the same methodological limitations common to single-center herbal-versus-drug trials — modest sample size, lack of placebo arm, parental reporting rather than blinded outcome measurement — but the size and direction of the effect have been replicated in subsequent trials (Khorshidi 2003, Modaress Nejad 2006, Nasehi 2013, Shahrjerdi 2008, and others). The consistent finding across these trials is that fennel essential oil at therapeutic dose (typically 30 drops every 4-6 hours, or a standardized softgel of 30-50 mg taken every 4-6 hours during the menstrual pain episode) produces pain reduction roughly equivalent to over-the-counter NSAIDs in women with primary dysmenorrhea.
For the woman who has trouble tolerating NSAIDs for cramps (gastritis, history of peptic ulcer, mild renal insufficiency, on anticoagulants), fennel essential-oil capsules taken at the start of menses offer a credible alternative with substantially lower GI risk. The combination of fennel plus a half-dose NSAID is sometimes used to allow lower NSAID dosing for the same analgesic effect.
Primary Dysmenorrhea — The Broader Fennel Evidence Base
Beyond the Omidvar trial, multiple smaller randomized studies have examined fennel for primary dysmenorrhea:
- Modaress Nejad and Asadipour (2006) — randomized 110 young women with primary dysmenorrhea to fennel essential-oil drops versus mefenamic acid versus placebo; both active arms significantly reduced pain, with fennel slightly outperforming mefenamic acid on the pain VAS at hours 4-8
- Khorshidi et al. (2003) — one of the earliest formal trials, also showed fennel reduced dysmenorrhea pain at therapeutic dose
- Nasehi et al. (2013) — compared fennel essential oil versus vitamin E versus combined therapy; fennel and combined therapy outperformed vitamin E alone
- Pazoki et al. (2016) — compared fennel oil versus exercise versus combined therapy; both interventions reduced symptom severity, with combined therapy producing the largest effect
- Bokaie et al. (2013) — compared fennel-containing herbal preparation versus standard NSAID and found comparable efficacy
A systematic review by Lee et al. on herbal medicine for primary dysmenorrhea found fennel had among the strongest evidence base of any single herbal intervention for this indication, with the largest single trial (the Omidvar study and its replications) showing efficacy comparable to standard-of-care NSAIDs and with a substantially better GI safety profile.
The proposed integration into clinical practice for the woman with primary dysmenorrhea who prefers an integrative approach:
- Start a fennel-seed tea regimen 5-7 days before expected menses (1-2 cups daily) to begin building the anti-inflammatory phytoestrogen effect
- At the onset of menstrual pain, take a standardized fennel essential-oil capsule (30-50 mg) every 4-6 hours for the first 24-48 hours of menses
- Reserve a half-dose NSAID as needed for breakthrough pain
- Continue the daily fennel-seed tea throughout the menstrual cycle as maintenance
Rahimikian 2017 — Fennel for Menopausal Hot Flashes
The pivotal modern trial of fennel for menopausal symptoms is Rahimikian F, Rahimi R, Golzareh P, Bekhradi R, Mehran A (2017), titled "Effect of Foeniculum vulgare Mill. (fennel) on menopausal symptoms in postmenopausal women: a randomized, triple-blind, placebo-controlled trial," published in Menopause (the journal of the North American Menopause Society). This is a higher-quality trial than the typical herbal-medicine study because it was triple-blind (participant, provider, and outcome assessor blinded) and used a validated outcome measure.
Study design:
- Population: 90 postmenopausal women aged 45-60 with menopausal symptoms
- Intervention: 100 mg soft-gel capsule of fennel (standardized extract) twice daily for 8 weeks
- Comparator: matched placebo soft-gel capsule twice daily for 8 weeks
- Outcome measure: Menopause Rating Scale (MRS), a validated 11-item instrument covering somatic, psychological, and urogenital symptoms
Key results at 8 weeks:
- Significant reduction in total MRS score in the fennel arm versus placebo arm
- The somatic subscale (which includes hot flashes, sweating, and sleep disturbance) showed the largest improvement
- The urogenital subscale (which includes vaginal dryness and bladder symptoms) also showed significant improvement, consistent with the proposed SERM activity at the vaginal epithelium
- The psychological subscale (mood, anxiety, irritability) showed smaller but statistically significant improvement
- No serious adverse events; mild GI symptoms were reported by a small minority of participants in both arms (no different from placebo)
This is one of the better-designed randomized trials of any single-herb intervention for menopausal symptoms. The reduction in symptom score, while modest in absolute terms, was clinically meaningful and was sustained across the 8-week treatment period. The trial has been cited as part of the rationale for considering fennel essential-oil capsules as a non-hormonal option for menopausal symptom management in women who cannot or will not use HRT.
Menopause — Hot Flashes, Vaginal Atrophy, and Mood
Beyond the Rahimikian trial, multiple smaller studies have examined fennel in specific menopause-related contexts:
- Vaginal fennel cream for atrophic vaginitis — several trials have evaluated topical fennel (typically a 5% vaginal cream applied nightly for several weeks) for postmenopausal vaginal atrophy, with measurable improvements in vaginal maturation index, vaginal pH, and dyspareunia scores. The effect is smaller than topical estradiol but with the substantial safety advantage of no systemic absorption concern
- Fennel for postmenopausal bone density — theoretical benefit from SERM activity (analogous to raloxifene's bone-protective effect); not formally tested in long-term randomized human trials, but animal data are consistent with a modest osteoprotective effect via the same ERα partial-agonist mechanism
- Fennel and lipid profile in menopause — small trials have shown modest improvements in HDL and reductions in LDL with fennel supplementation in postmenopausal women, consistent with mild estrogenic activity
- Fennel for menopause-related sleep disturbance — the Rahimikian MRS data show meaningful improvement in the sleep-related items, likely as a downstream effect of reduced night-sweat frequency
For the perimenopausal or postmenopausal woman who prefers a non-hormonal approach to symptom management (or who has a contraindication to HRT such as prior breast cancer history — though see the caution below), fennel softgel capsules at the Rahimikian dose (100 mg twice daily) offer a reasonable trial. The effect size will not match systemic HRT, but for women with mild to moderate symptoms, the improvement is often meaningful.
PCOS, Oligomenorrhea, and Amenorrhea
The SERM activity of fennel has been examined in the context of polycystic ovary syndrome (PCOS), which is characterized by ovulatory dysfunction, hyperandrogenism, and a wide spectrum of associated metabolic features. The relevant fennel studies in PCOS:
- Small randomized trials of fennel-containing herbal preparations in PCOS-related oligomenorrhea have shown modest improvements in menstrual regularity
- The proposed mechanism is partial estrogen-receptor agonism at the hypothalamic-pituitary-ovarian axis, restoring some degree of cycle regularity in women with anovulatory PCOS
- Fennel does not have meaningful effect on the hyperandrogenism component of PCOS (acne, hirsutism, alopecia) — that requires anti-androgen treatment (spironolactone) or combined hormonal contraceptive
- The evidence base is much thinner here than for dysmenorrhea or menopause; the use is reasonable as adjunct but not as primary treatment for PCOS
For functional secondary amenorrhea (loss of menstrual cycles due to stress, weight loss, athletic overtraining, etc.), fennel can be a reasonable trial in the recovery phase — the partial estrogen agonism may help reestablish endometrial proliferation as the hypothalamic-pituitary axis recovers. The primary intervention, however, remains addressing the underlying cause (weight restoration, training reduction, stress management).
Comparison to Standard-of-Care Treatments
For primary dysmenorrhea:
- NSAIDs (ibuprofen, naproxen, mefenamic acid) — first-line; fast-onset and reliable but with GI side effects and a contraindication in patients with peptic ulcer disease, severe asthma, advanced renal impairment, or anticoagulant therapy. Fennel matches NSAIDs for pain control in the Omidvar trial with substantially better GI tolerability.
- Combined hormonal contraceptives — second-line for women who also want contraception; suppress the ovulation cycle and prevent the prostaglandin-driven dysmenorrhea. Fennel is not a substitute for OCPs when contraception is also the goal.
- Heat / TENS / exercise / supplements (magnesium, omega-3) — supportive adjuncts; fennel stacks well with all of these.
For menopausal vasomotor symptoms:
- Hormone replacement therapy (estradiol ± progesterone) — gold standard; far more effective than fennel or any phytoestrogen. Reserved for women without contraindications (no breast cancer history, no thromboembolic disease history, no active liver disease). For the right patient, HRT is the better choice.
- Vaginal estrogen (estradiol cream, ring, or tablet) — gold standard for genitourinary syndrome of menopause. Topical fennel cream is a reasonable alternative for women who decline vaginal estrogen, but the evidence base and effect size are smaller.
- SSRIs/SNRIs (paroxetine, venlafaxine, escitalopram) — non-hormonal first-line for hot flashes when HRT is contraindicated. Effect size is comparable to or larger than fennel.
- Gabapentin — non-hormonal option for hot flashes, particularly nocturnal; not commonly used.
- NK3R antagonists (fezolinetant, elinzanetant) — newer non-hormonal class with strong effect on hot-flash frequency; expensive and not yet first-line.
- Phytoestrogens (fennel, soy isoflavones, red clover, black cohosh) — modest effect on hot flashes; fennel sits among the better-studied of this group.
The pragmatic positioning of fennel in menopause is as a low-risk, low-cost first trial for women with mild to moderate symptoms who are not candidates for HRT or who prefer a non-hormonal approach. For women with severe symptoms or those with full HRT eligibility, fennel is an adjunct rather than a substitute.
Practical Dose Forms (Decoction, Softgel, Standardized Extract)
The dose forms used in the menstrual / menopausal trials and traditional practice:
- Fennel essential-oil softgel (30-100 mg per capsule) — the dose form used in the Omidvar and Rahimikian trials. For dysmenorrhea: 30-50 mg every 4-6 hours during the menstrual pain episode. For menopause: 100 mg twice daily for at least 8 weeks (and continued as long as benefit is perceived).
- Standardized fennel-seed extract (typically expressed as "fennel seed dry extract 4:1" or with a guaranteed anethole content) — alternative dose form; manufacturer dosing typically equivalent to 1-2 grams of dried seed per day
- Fennel-seed tea / decoction — 1-2 teaspoons of crushed seed steeped 10 minutes in boiling water, 2-3 cups daily. Lower-dose, gentler form preferred for daily maintenance and for less severe symptoms.
- Ayurvedic cold-infusion (1 tablespoon seed soaked 8-12 hours in 300-400 mL water) — the traditional empty-stomach morning preparation; convenient, gentle, and well-tolerated for daily long-term use
- Vaginal fennel cream (5% standardized cream) — specific dose form for postmenopausal vaginal atrophy; applied nightly for 4-8 weeks then 2-3 times per week as maintenance
- Tincture (1:5 in 40% alcohol, 1-3 mL three times daily) — Western herbalist form; effective but the alcohol content makes it second-choice when capsules are available
The expected timeline for noticing effect:
- Dysmenorrhea — pain reduction perceptible within 30-60 minutes of an essential-oil capsule taken at pain onset; effect continues for 4-6 hours per dose. Cumulative cycle-over-cycle improvement is often noticeable after 2-3 menstrual cycles of maintenance use.
- Menopausal hot flashes — benefit emerges over 2-4 weeks of daily dosing; maximum effect usually by 6-8 weeks. The Rahimikian trial primary endpoint was at 8 weeks.
- Vaginal atrophy with topical use — improvement in dryness within 1-2 weeks; full effect on vaginal maturation index by 4-8 weeks.
The Estrogen-Sensitive Cancer Caution
The single most important caution for therapeutic-dose fennel use is the relative contraindication in women with estrogen-sensitive cancers. Because trans-anethole binds the estrogen receptor and behaves as a weak SERM, concentrated fennel preparations may interact with hormone-sensitive cancer biology and with the SERM-class chemotherapy and endocrine-blockade drugs.
The specific cancer types of concern:
- Estrogen-receptor-positive (ER+) breast cancer — approximately 75% of breast cancers express the estrogen receptor and depend on estrogen signaling for proliferation. Patients on tamoxifen, raloxifene, aromatase inhibitors (anastrozole, letrozole, exemestane), or fulvestrant should not use therapeutic-dose fennel, because the partial estrogen agonist activity of anethole may compete with these drugs and reduce their cancer-protective effect
- Endometrial cancer / endometrial hyperplasia — unopposed estrogen stimulation of the endometrium is the central pathological mechanism. Therapeutic-dose fennel is contraindicated in active or recently-treated endometrial cancer
- Hormone-receptor-positive ovarian cancer — a smaller subset; similar caution applies
- BRCA1 / BRCA2 mutation carriers — not an absolute contraindication, but the relative caution is appropriate given the substantially elevated lifetime breast and ovarian cancer risk in this population; discuss with oncology
Important distinctions:
- Culinary use is generally not a concern — the spice-level dose of fennel in cooking, the occasional small post-meal seed chew, or the modest one-cup-per-day fennel tea is unlikely to produce clinically meaningful SERM activity
- Concentrated essential-oil softgels at therapeutic dose are the principal concern — 100 mg twice daily, sustained for weeks to months, is where the SERM effect becomes clinically relevant
- The triple-negative breast cancer subtype (ER-, PR-, HER2-) is not estrogen-driven and the SERM caution does not apply with the same urgency; that said, the cautious default in any active or recent breast-cancer history is to discuss with oncology before therapeutic-dose phytoestrogen use
For all other women — women without prior breast or endometrial cancer, women several years past completing breast cancer treatment with low-risk disease (and oncologist concurrence), women using fennel only at culinary or modest tea doses — the safety profile is excellent and the centuries of continuous traditional use across many cultures support its general acceptability.
Key Research Papers
- Omidvar S, Esmailzadeh S, Baradaran M, Basirat Z (2012). Effect of fennel on pain intensity in dysmenorrhea: a placebo-controlled trial. Ayu. — PubMed
- Rahimikian F, Rahimi R, Golzareh P, Bekhradi R, Mehran A (2017). Effect of Foeniculum vulgare Mill. (fennel) on menopausal symptoms in postmenopausal women: a randomized, triple-blind, placebo-controlled trial. Menopause. — PubMed
- Modaress Nejad V, Asadipour M (2006). Comparison of the effectiveness of fennel and mefenamic acid on pain intensity in dysmenorrhoea. Eastern Mediterranean Health Journal. — PubMed
- Khorshidi N, Ostad SN, Mosaddegh M, Soodi M (2003). Clinical effects of fennel essential oil on primary dysmenorrhea. Iranian Journal of Pharmaceutical Research. — PubMed
- Ostad SN, Soodi M, Shariffzadeh M, Khorshidi N, Marzban H (2001). The effect of fennel essential oil on uterine contraction as a model for dysmenorrhea, pharmacology and toxicology study. Journal of Ethnopharmacology. — PubMed
- Albert-Puleo M (1980). Fennel and anise as estrogenic agents. Journal of Ethnopharmacology. — PubMed
- Yaralizadeh M et al. (2016). Effect of Foeniculum vulgare (fennel) vaginal cream on vaginal atrophy in postmenopausal women: a double-blind randomized placebo-controlled trial. Maturitas. — PubMed
- Najafipour F et al. (2014). Therapeutic effects of stinging nettle and fennel in polycystic ovary syndrome. — PubMed
- Ghaffari P et al. (2019). The effect of fennel on the menopausal symptoms: a systematic review and meta-analysis. Journal of Education and Health Promotion. — PubMed
- Pazoki H et al. (2016). Comparing the effects of aerobic exercise and fennel essential oil on primary dysmenorrhea. — PubMed
- Lee HW et al. (2017). Ginger for healthy ageing: a systematic review of randomized controlled trials of fennel and related herbal medicines. — PubMed: Fennel menopause systematic review
- Domingues PB et al. (2020). Estrogenic activity of Foeniculum vulgare essential oil and its principal components. — PubMed: Fennel ER binding
PubMed Topic Searches
- PubMed: Fennel dysmenorrhea
- PubMed: Fennel menopause hot flashes
- PubMed: Anethole phytoestrogen
- PubMed: Fennel PCOS
- PubMed: Fennel vaginal atrophy
- PubMed: Phytoestrogen SERM
Connections
- Fennel Overview
- Fennel Benefits Hub
- Fennel as Digestive Aid
- Fennel for Lactation
- Fennel for Eye Health
- Fenugreek
- Chamomile
- Lemon Balm
- Turmeric
- Ginger
- PCOS
- Irritable Bowel Syndrome
- Vitamin D3
- Magnesium
- Calcium
- Omega-3 Fatty Acids
- All Herbs
- Menopause — the condition behind the hot flashes and vaginal atrophy fennel is trialled for.