Fennel for Lactation and as a Galactagogue
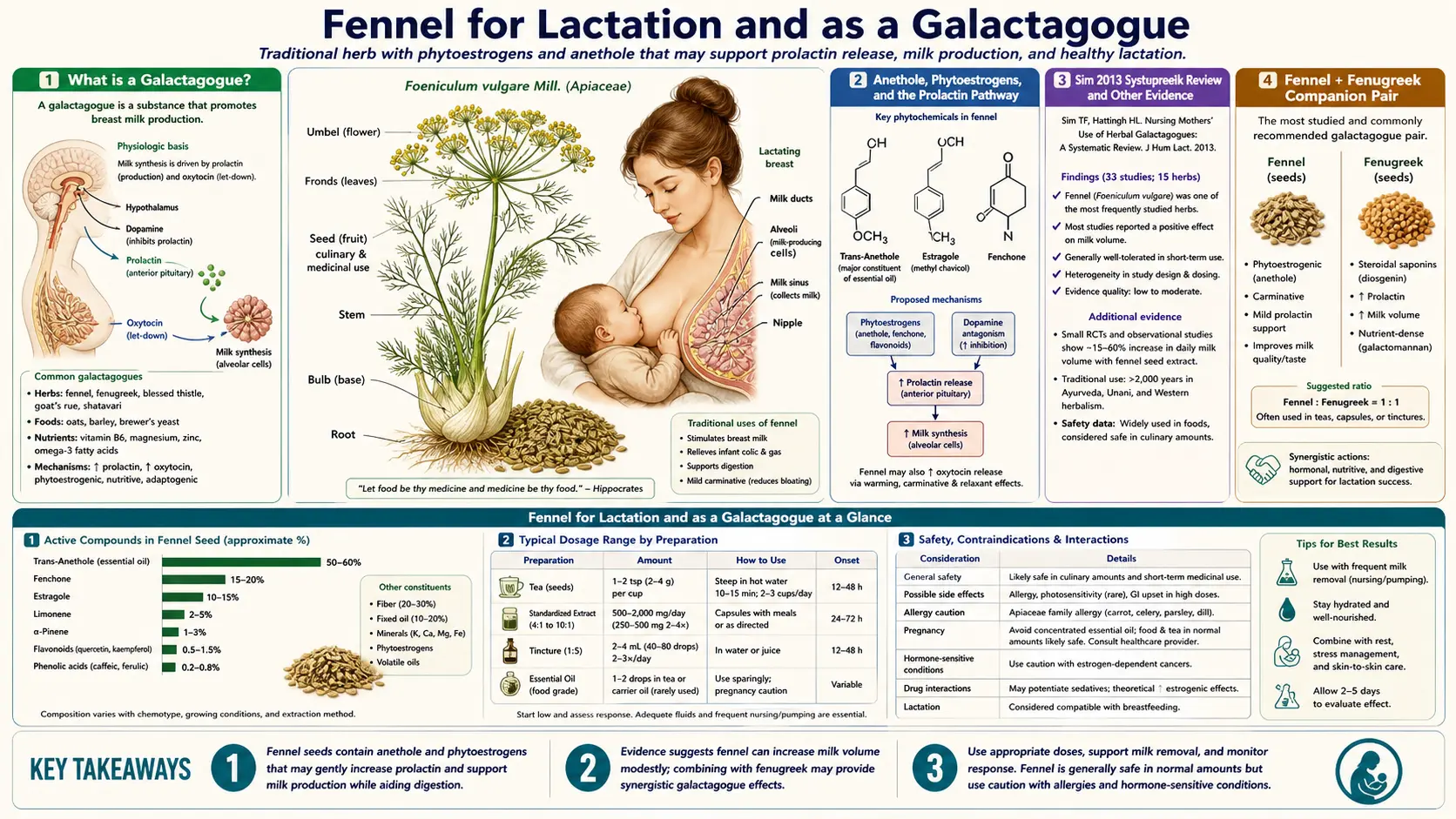
A galactagogue is any agent — food, herb, or drug — that increases breast-milk production. Fennel is one of the two most-used herbal galactagogues worldwide, alongside fenugreek, and the two are routinely used together in postpartum tea blends from the Mediterranean to South Asia. The Sim 2013 systematic review and the consistent ethnobotanical record across at least eight independent cultural traditions establish fennel as a credible galactagogue with a plausible mechanism (the phytoestrogenic anethole appears to enhance prolactin signalling at the lactotroph). For the breastfeeding mother facing low milk supply — particularly the mother of a premature infant in the NICU, the mother returning to work and pumping, or the mother with delayed lactogenesis after Caesarean delivery — fennel offers a low-cost, low-risk first-line intervention that is widely accepted by lactation consultants and is broadly compatible with breastfeeding per the LactMed and e-lactancia pharmacology databases. This deep-dive covers the mechanism, the trial evidence, the comparison to the prescription dopamine antagonist domperidone, traditional postpartum dose forms, and the one unresolved infant-exposure question.
Table of Contents
- What is a Galactagogue? (And Why Mothers Reach for One)
- Anethole, Phytoestrogens, and the Prolactin Pathway
- The Sim 2013 Systematic Review and Other Evidence
- Fennel + Fenugreek — The Companion Pair
- Fennel vs Domperidone — The Safety Profile Comparison
- Traditional Postpartum Use Across Cultures
- Dosing for Nursing Mothers
- The Infant-Exposure Question — Anethole in Breast Milk
- When to Use Fennel (and When Not To)
- Cautions and Contraindications
- Key Research Papers
- Connections
- Featured Videos
What is a Galactagogue? (And Why Mothers Reach for One)
A galactagogue is any agent that increases milk production in a lactating mother. The category includes prescription drugs (the dopamine antagonists metoclopramide and domperidone), foods believed to support supply (oats, dark leafy greens, brewer's yeast), herbs (fennel, fenugreek, blessed thistle, goat's rue, milk thistle, shatavari), and the most-important non-pharmacological intervention — frequent, effective breast emptying, which is the primary physiological driver of supply regardless of any pharmaceutical or herbal adjunct.
The clinical scenarios in which a mother reaches for a galactagogue typically include:
- Delayed lactogenesis — the normal transition from colostrum to mature milk volume usually occurs by day 3-5 postpartum but can be delayed beyond day 5 in 25-40% of first-time mothers, especially after Caesarean delivery, retained placenta, postpartum hemorrhage, obesity, gestational diabetes, or PCOS
- Inadequate weight gain in the breastfed infant — the most common medical indication for galactagogue use, defined as less than 20-30 grams/day after the first week of life or failure to regain birth weight by day 14
- Pumping mothers — mothers exclusively pumping for a premature infant in NICU or mothers returning to work who need to maintain supply through pump expression alone, which tends to produce lower volumes than direct nursing
- Re-lactation or induced lactation — mothers attempting to restart milk production after an interruption, or adoptive mothers seeking to induce lactation
- Perceived insufficient milk — the most common reason a mother stops breastfeeding earlier than she intended, often when objective supply is actually adequate but the mother is reading normal infant cluster-feeding behavior as hunger
The galactagogue prescription should always sit downstream of an assessment of breastfeeding technique, latch quality, frequency of feeds, the rule-out of medical causes of low supply (retained placenta, Sheehan's syndrome, hypothyroidism, prior breast surgery), and a careful conversation about perceived versus measured supply. With those checks done, a galactagogue can provide a useful 10-30% bump in supply for many mothers — meaningful in the marginal case.
Anethole, Phytoestrogens, and the Prolactin Pathway
Lactation is governed by two hormones working through complementary mechanisms:
- Prolactin — secreted by anterior pituitary lactotrophs, drives the synthesis of milk constituents in the lactating alveolus. Prolactin secretion is held under tonic dopaminergic inhibition; dopamine binding to D2 receptors on the lactotroph reduces prolactin release. Pharmacological galactagogues (metoclopramide, domperidone) work by blocking the D2 receptor and lifting the inhibition. Endogenous prolactin release is stimulated by the suckling reflex.
- Oxytocin — secreted by the posterior pituitary, drives the milk-ejection (let-down) reflex by contracting the myoepithelial cells around the alveoli. Stress, anxiety, and pain inhibit oxytocin release; warmth, skin-to-skin contact, and a calm environment promote it.
The mechanism by which fennel and other phytoestrogenic herbs enhance lactation appears to operate through the prolactin pathway. Estrogen has a known prolactin-stimulating effect at the pituitary — high circulating estrogen in late pregnancy is what primes the mammary tissue for lactation, and the abrupt fall in placental estrogen after delivery is what permits prolactin to surge. The phytoestrogenic anethole in fennel appears to maintain modest estrogen-receptor stimulation at the pituitary into the postpartum period, supporting continued prolactin output. The effect is dose-dependent and modest — nothing close to the magnitude of pharmacologic dopamine antagonists — but consistent across multiple in vivo studies in lactating animals and the limited human data.
A second proposed mechanism is via the cholinergic enhancement of oxytocin release. Anethole has been shown in animal preparations to enhance acetylcholine-mediated nerve transmission, and oxytocin release is partly cholinergic. The contribution of this mechanism to the clinical galactagogue effect is unclear but may explain the long-standing folkloric report that fennel-containing teas seem to improve the "let-down" experience more than they raise pump volume per se.
The Sim 2013 Systematic Review and Other Evidence
The most-cited evidence summary on herbal galactagogues is the qualitative work by Sim, Sherriff, Hattingh, Parsons, and Tee (2013), titled "The use, perceived effectiveness and safety of herbal galactagogues during breastfeeding," published in the International Breastfeeding Journal. The Sim work surveyed Australian women who had used herbal galactagogues postpartum and reviewed the published literature on the most-commonly used agents.
Key findings from Sim 2013 and the surrounding literature:
- Fennel and fenugreek are by far the two most-commonly-used herbal galactagogues globally; the combination is the dominant pattern across multiple cultural traditions
- Self-reported perceived effectiveness was high (60-90% of users in various surveys reported they believed the herb increased their supply)
- Objective trial-quality evidence is limited but supportive — small randomized trials of fennel-containing teas in lactating women have shown statistically significant increases in milk volume on the order of 30-65% over baseline, with corresponding improvements in infant weight gain
- The Turkmen 2009 trial randomized 66 mothers of preterm infants to either a fennel-containing herbal tea or placebo; the fennel arm showed significant improvements in milk volume, infant weight gain, and reduced time to reach full enteral feeding
- Safety in both mother and infant was good across all studies; no serious adverse events were attributable to fennel
- The Reeder 2013 case report of a maternal-grand-multipara who used fennel for re-lactation provides a representative single-patient demonstration of effect
The honest framing is that the evidence base for fennel as a galactagogue is built from many small studies, traditional use, and biologically plausible mechanism — not from a single large definitive randomized trial. This is the case for nearly all herbal galactagogues; even the prescription dopamine antagonist domperidone has surprisingly modest randomized evidence given how widely it is used (and is unapproved for this indication in the United States due to the FDA cardiotoxicity warning).
Fennel + Fenugreek — The Companion Pair
Across nearly every cultural tradition that uses herbal galactagogues, fenugreek (Trigonella foenum-graecum) and fennel appear together. The two are biochemically and mechanistically complementary:
- Fenugreek — the more potent of the pair; the active mechanism is via the steroidal-saponin diosgenin (a structural cousin of estrogen) plus a direct effect on milk volume that is independent of prolactin (the precise pathway remains debated). Side effects: a distinctive maple-syrup body odor (also in the infant's urine via metabolic transfer), occasional hypoglycemia (relevant for mothers with insulin-treated diabetes), and a small but real cross-allergy risk with peanut and chickpea
- Fennel — the gentler, sweeter-tasting companion; the active mechanism is via anethole's phytoestrogenic effect; tends to be better-tolerated than fenugreek with fewer side effects but a smaller effect size individually
Most commercial nursing teas contain both herbs along with several adjuncts — common combinations include blessed thistle, anise seed, caraway, and goat's rue. The classic European nursing tea (Mother's Milk Tea by Traditional Medicinals is a representative US-market example) is essentially fennel and fenugreek with adjuncts.
The dose for the combination is typically two to three cups of tea per day, started in the first week postpartum (or earlier, in the case of antenatal supply preparation in a mother with prior low-supply experience), continued until adequate supply is established. Most mothers notice a perceived effect within 24-72 hours of starting the tea; the objective volume change in the breast pump is typically measurable within a week.
Fennel vs Domperidone — The Safety Profile Comparison
For mothers with serious low-supply problems, the most commonly prescribed pharmacological galactagogue globally is domperidone, a peripheral dopamine D2 antagonist with strong prolactin-elevating effect. Domperidone is widely available in Canada, Europe, Australia, and most of Asia, but is not approved by the FDA in the United States due to a 2004 warning about cardiac arrhythmia (QT-prolongation and sudden cardiac death risk) at high doses. US lactation consultants sometimes recommend importation from Canadian pharmacies, but the practice sits in a regulatory gray zone.
The comparative profile of the two galactagogues:
- Effect size — domperidone produces a larger milk-volume increase (typically 30-80% over baseline at 20-30 mg three or four times per day) than fennel (typically 15-40% at therapeutic doses). For mothers with severe supply problems — particularly mothers of premature infants in the NICU — the larger effect of domperidone often justifies its use.
- Cardiac safety — domperidone carries a real (small but documented) risk of QT prolongation and sudden cardiac death, particularly in older patients, those on QT-prolonging co-medications, those with electrolyte abnormalities, and at high doses. Fennel has no documented cardiac signal at any dose used in lactation.
- Other side effects — domperidone causes dry mouth, headache, mild GI upset; rebound supply drop on discontinuation. Fennel has minimal side effects at typical lactation doses.
- Cost and access — fennel is essentially free worldwide and requires no prescription. Domperidone requires a prescription where it is approved and an importation workaround in the US.
- Mechanism transparency — both have plausible mechanisms (dopamine antagonism for domperidone, phytoestrogen + prolactin for fennel) but fennel's effect is more dose-variable and less predictable.
The pragmatic approach in clinical practice is to use fennel as first-line for mild to moderate low supply (a 10-30% bump matters here), reserve domperidone for severe low supply or for mothers of preterm infants where the higher effect-size justifies the cardiac risk-benefit tradeoff, and always pair either intervention with optimization of nursing technique, frequency, and rest. The two are not mutually exclusive — many mothers use fennel tea alongside prescribed domperidone.
Traditional Postpartum Use Across Cultures
The use of fennel in postpartum care is documented across at least eight independent cultural traditions:
- Mediterranean (Italian, Greek, Spanish) — fennel-anise-fenugreek tea (finocchio e anice in Italian; maramoyo in Greek) given to nursing mothers; the bulb is also eaten freely
- Indian Ayurveda — the postpartum tradition of jeerakarishta (a cumin / fennel / fenugreek fermented decoction) and shatavari-and-fennel ghee for the nursing mother
- Pakistani / North Indian — the daily seed mixture (panjiri, traditionally given postpartum) contains fennel, fenugreek, gum arabic, and ghee
- Middle Eastern (Lebanese, Syrian, Egyptian) — the daily nursing-mother decoction (moghli in Levantine tradition) includes fennel, anise, caraway, and cinnamon
- North African (Moroccan, Tunisian) — the postpartum tea (shiba-based blends) contains fennel as a primary component
- Chinese postpartum (zuo yuezi, "sitting the month") — fennel is one of the warming carminative herbs in postpartum cooking, especially in southern Chinese tradition
- Mexican / Latin American — hinojo tea is the traditional galactagogue, often combined with anise and chamomile
- Northern European folk medicine — Scandinavian and German nursing-mother teas have used fennel for centuries
The cross-cultural convergence on a single herb for a single indication is one of the better arguments for the herb's actual effect — this is not a culturally idiosyncratic remedy but a global pattern that emerged independently across geography and language.
Dosing for Nursing Mothers
The dosing schedule that emerges from the clinical-trial literature, traditional use, and the EMA HMPC monograph:
- Fennel-seed tea (the standard form) — 1 to 2 teaspoons of crushed seed per cup of boiling water, steeped 10 minutes, 2 to 3 cups per day. Total daily seed dose: 5-7 grams.
- Fennel-seed decoction (stronger) — 1 tablespoon of crushed seed simmered in 500 mL water for 10 minutes, divided into two doses across the day.
- Combined nursing tea (Mother's Milk, Weleda Stillungstee, or homemade) — 1 to 2 teaspoons of the blend per cup, 2 to 4 cups per day. Most commercial blends are dose-calibrated to deliver roughly 1-2 grams each of fennel and fenugreek per cup.
- Standardized fennel essential-oil capsule (e.g. 100 mg per softgel) — 1 capsule two to three times per day. This is the most-concentrated form and not the traditional preference for lactation, but used in some clinical-trial settings.
- Tincture (1:5 in 40% alcohol) — 2-3 mL three times per day. Caution: the alcohol content is a concern in nursing, so the tincture is generally not the preferred form — tea or capsule is better.
Timing: many mothers find best results from drinking a warm cup of tea 30 minutes before a nursing or pumping session — the warmth itself triggers a stronger let-down, independent of the herb's pharmacological effect. The total daily dose is more important than the timing of individual cups.
Duration: continue for as long as galactagogue support is needed (typically the first 1-3 months postpartum for delayed lactogenesis, or as long as pumping continues for an NICU baby or working mother). There is no documented harm from prolonged use at lactation doses, but there is also no documented benefit beyond achieving the supply goal.
The Infant-Exposure Question — Anethole in Breast Milk
The one unresolved scientific question about fennel in lactation is the magnitude and clinical significance of the infant's exposure to anethole and other fennel essential-oil components via breast milk. Anethole is a small, lipid-soluble molecule that transfers freely into milk — nursing infants of mothers consuming fennel tea show detectable anethole in plasma and exhibit a measurable change in milk flavor (some infants nurse more eagerly when the mother has been drinking fennel tea, presumably because of the sweet anise flavor).
The infant-exposure data:
- LactMed (NIH National Library of Medicine drugs-and-lactation database) — lists fennel as "limited published information; appears compatible with breastfeeding at usual culinary and tea doses"
- e-lactancia (the European pediatric pharmacology breastfeeding compatibility database) — gives fennel its second-tier rating ("possible risk") due to estragole content in essential-oil concentrate, with the recommendation to use the seed/tea form (lower estragole exposure) and avoid concentrated essential-oil capsules during nursing if culinary or tea forms are an option
- Several case reports describe infants who became drowsy or had GI symptoms after the mother consumed very large doses of fennel tea (greater than 10 cups per day) or high-dose essential-oil capsules — symptoms resolved with dose reduction
- No serious adverse event has been documented at typical 2-3 cup-per-day lactation tea doses
The pragmatic clinical guidance, which the major lactation-consultant organizations have converged on, is:
- Tea and decoction forms at standard 2-3 cup-per-day doses are well-tolerated by both mother and infant
- Standardized essential-oil softgels are best avoided during lactation if the tea form is an option; if essential-oil capsules are used, stay at the low end of the dose range (100-200 mg per day)
- Watch the infant for any drowsiness, diarrhea, vomiting, or rash; discontinue if any of those appear
- Avoid in mothers of infants with documented allergy to umbelliferous family (celery, carrot, anise)
- The estragole concern, while real, is not a contraindication at standard doses — the cumulative exposure is far below any documented threshold of harm
When to Use Fennel (and When Not To)
Good candidate scenarios for fennel galactagogue:
- First-week postpartum with delayed lactogenesis, mother nursing or pumping frequently but supply not yet meeting infant demand
- Mother of a healthy term infant with mild low-supply concerns once technique and frequency are confirmed adequate
- Pumping mother (return to work, NICU baby) where supply is gradually declining
- Re-lactation attempt after weaning interruption
- Mother wishing a low-cost, low-risk first-line intervention before pharmaceutical options
Scenarios where fennel is not the right tool:
- Severe low supply in a NICU mother where domperidone's larger effect-size matters — consider domperidone first (or both)
- Low supply caused by a treatable medical problem (retained placenta, undiagnosed hypothyroidism, severe anemia) — treat the underlying cause first
- Mother with history of estrogen-sensitive breast cancer or active breast cancer — the SERM activity is a relative contraindication; consult oncology
- Infant with documented sensitivity to umbelliferous spices — rare but reported
- Perceived low supply in a mother whose objective measurement is normal — the right intervention is education, not a galactagogue
Cautions and Contraindications
- Estrogen-sensitive cancer — the principal contraindication. The SERM activity of anethole is a real concern for mothers with prior estrogen-receptor-positive breast cancer who are nursing after treatment completion. Consult oncology before starting therapeutic-dose fennel.
- Infant tolerance — rare reports of drowsiness, GI upset, or rash in nursing infants of mothers consuming very large fennel doses. Always start at the low end of the dose range and watch the infant.
- Allergy — cross-reactive allergy to umbelliferous plants (celery, carrot, parsley, anise, dill, mugwort) is occasionally reported.
- Hormonal contraceptive interaction — theoretical concern about additive estrogen effect; clinical significance unclear for typical doses.
- Anticoagulant interaction — trans-anethole has shown mild antiplatelet activity in some in vitro studies; theoretical additive effect with warfarin or DOACs. Not a contraindication but worth noting for surgical patients.
- Estragole / safrole concern — at the very high end of essential-oil dosing, the genotoxic potential of estragole is a theoretical concern; not relevant at culinary or tea-level doses.
- Pregnancy — concentrated fennel essential-oil capsules are contraindicated in pregnancy. Culinary use is fine. The galactagogue indication starts after delivery, not before.
Key Research Papers
- Sim TF, Sherriff J, Hattingh HL, Parsons R, Tee LB (2013). The use, perceived effectiveness and safety of herbal galactagogues during breastfeeding: a qualitative study. International Breastfeeding Journal. — PubMed
- Turkmen N et al. (2009). The effect of an herbal tea preparation on breast-milk volume and content in mothers of preterm infants. — PubMed
- Mortel M, Mehta SD (2013). Systematic review of the efficacy of herbal galactagogues. Journal of Human Lactation. — PubMed
- Bazzano AN et al. (2016). A review of herbal and pharmaceutical galactagogues for breastfeeding. Ochsner Journal. — PubMed
- Albert-Puleo M (1980). Fennel and anise as estrogenic agents. Journal of Ethnopharmacology. — PubMed
- Foong SC et al. (2020). Oral galactagogues (natural therapies or drugs) for increasing breast milk production in mothers of non-hospitalised term infants. Cochrane Database of Systematic Reviews. — PubMed: Cochrane galactagogues
- Penagos Tabares F, Bedoya Jaramillo JV, Ruiz-Cortés ZT (2014). Pharmacological overview of galactogogues. Veterinary Medicine International. — PubMed: Galactogogue pharmacology
- The Academy of Breastfeeding Medicine Protocol Committee (2018). ABM Clinical Protocol #9: Use of Galactogogues in Initiating or Augmenting Maternal Milk Production, Second Revision. — PubMed: ABM Protocol 9
- Khan TM et al. (2018). A systematic review of effective therapeutic strategies for management of insufficient milk supply. European Journal of Hospital Pharmacy. — PubMed
- Ozalkaya E et al. (2018). Effect of a galactagogue herbal tea on breast milk volume and prolactin secretion by mothers of preterm babies. — PubMed
- Javan R et al. (2017). A review of medicinal plants effective in lactation insufficiency. Iranian Red Crescent Medical Journal. — PubMed
- Zuppa AA et al. (2010). Safety and efficacy of galactogogues: substances that induce, maintain and increase breast milk production. Journal of Pharmacy & Pharmaceutical Sciences. — PubMed
PubMed Topic Searches
- PubMed: Fennel galactagogue lactation
- PubMed: Fenugreek-fennel breast milk
- PubMed: Anethole prolactin
- PubMed: Domperidone galactagogue
- PubMed: Galactagogue systematic review
- PubMed: Postpartum herbal tea
Connections
- Fennel Overview
- Fennel Benefits Hub
- Fennel as Digestive Aid
- Fennel for Menstrual & Menopausal
- Fennel for Eye Health
- Fenugreek (Companion Galactagogue)
- Chamomile
- Lemon Balm
- Ginger
- Coriander Seeds
- Cumin
- PCOS
- Vitamin D3 (Postpartum)
- Iron (Postpartum)
- Vitamin C
- All Herbs