Echinacea Immune Modulation Mechanisms
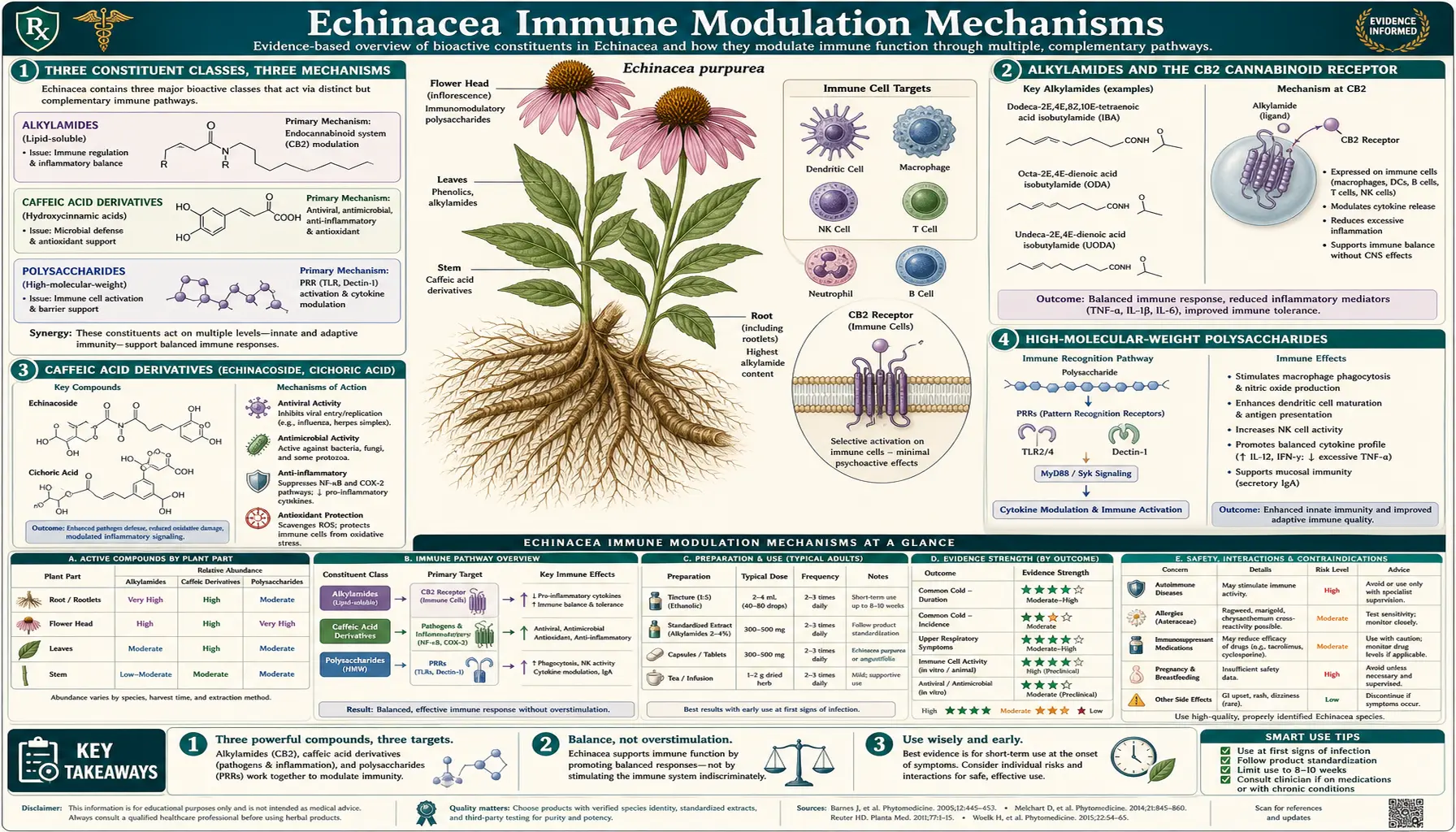
The popular phrase "Echinacea boosts the immune system" is at best a useful shorthand and at worst actively misleading. The molecular reality is more interesting: Echinacea contains at least three pharmacologically distinct classes of active constituent that interact with the immune system in fundamentally different ways. The alkylamides bind cannabinoid receptor 2 (CB2) on immune cells with affinity comparable to anandamide, the body's own endogenous cannabinoid. The caffeic acid derivatives (echinacoside, cichoric acid) act as antioxidants and direct antivirals while inhibiting bacterial hyaluronidase. The high-molecular-weight polysaccharides directly stimulate macrophages, dendritic cells, and natural killer cells through pattern-recognition receptors. These three mechanisms together produce modulation rather than simple stimulation — Echinacea appears to bring a dysregulated immune response back toward balance, calming excessive inflammation while supporting effective pathogen clearance. The species and the preparation determine which of the three mechanisms dominates, which is why no single "Echinacea" product captures the full range of effects.
Table of Contents
- Three Constituent Classes, Three Mechanisms
- Alkylamides and the CB2 Cannabinoid Receptor
- Caffeic Acid Derivatives (Echinacoside, Cichoric Acid)
- High-Molecular-Weight Polysaccharides
- Macrophage Activation and Cytokine Modulation
- Natural Killer Cell Stimulation
- Th1/Th2 Balance and Dendritic Cell Function
- Why "Modulator" Not "Booster"
- Species and Preparation Distinction
- Clinical Translation
- Key Research Papers
- Connections
- Featured Videos
Three Constituent Classes, Three Mechanisms
Phytochemical analysis of Echinacea tissue identifies dozens of secondary metabolites, but three constituent classes account for the bulk of the immunological activity:
- Alkylamides (isobutylamides) — lipophilic, tongue-tingling fatty-acid amides. The dodeca-2E,4E,8Z,10E/Z-tetraenoic acid isobutylamides are the most-studied; more than 20 distinct alkylamides have been characterized in the genus. Concentrated in E. angustifolia root and E. purpurea root, present at lower levels in E. purpurea aerial parts, largely absent from E. pallida.
- Caffeic acid derivatives — polar phenolic compounds. Echinacoside is the dominant compound in E. angustifolia and E. pallida; cichoric acid (2,3-dicaffeoyl-L-tartaric acid) is the dominant compound in E. purpurea. Other related compounds include caftaric acid, chlorogenic acid, and chicoric acid stereoisomers.
- High-molecular-weight polysaccharides and glycoproteins — heteroxylans (4-O-methylglucuronyl-xylan), arabinogalactans, fructans, and protein-bound polysaccharides. These are extracted by pressed-juice and water-extraction methods but precipitate out of concentrated alcoholic tinctures — an important distinction for preparation choice.
The three classes are not redundant; they act through different receptors on different cell types and produce different effects. The combined-action picture is what makes Echinacea genuinely interesting pharmacologically — it is not a single drug but a multi-target intervention, which may explain why the in-vitro mechanisms translate to modest but real clinical effects despite the bioavailability challenges of any single constituent.
Alkylamides and the CB2 Cannabinoid Receptor
The single most important pharmacological discovery in Echinacea research in the past two decades was the 2004 publication by Gertsch and colleagues in FEBS Letters showing that Echinacea alkylamides bind cannabinoid receptor 2 (CB2) with sub-micromolar affinity. CB2 is the immune-cell cannabinoid receptor (CB1 is the predominantly-neural cannabinoid receptor that mediates the psychoactive effects of THC), expressed at high levels on macrophages, B cells, T cells, natural killer cells, and microglia.
The endogenous ligand for CB2 is anandamide (an arachidonic-acid-derived endocannabinoid) and 2-arachidonoylglycerol. Both are produced on demand by immune cells in response to inflammatory signals and act as a negative-feedback brake on excessive immune activation. When endocannabinoid tone is low (chronic inflammation, autoimmune disease, neuroinflammation), CB2 signaling is insufficient and inflammation runs unchecked. When endocannabinoid tone is appropriate, CB2 signaling restrains inflammatory cytokine release while permitting effective pathogen clearance.
Echinacea alkylamides functionally mimic the endogenous endocannabinoid signal:
- Binding affinity — the dodeca-2,4,8,10-tetraenoic acid isobutylamide binds CB2 with Ki approximately 60 nM, comparable to or better than anandamide
- CB1 vs CB2 selectivity — the alkylamides show modest CB2 selectivity, meaning they preferentially target immune-cell cannabinoid receptors over neural ones; they are not psychoactive at oral doses, in stark contrast to THC
- Downstream signaling — CB2 binding by alkylamides reduces TNF-alpha gene expression in stimulated monocytes, modulates IL-12 production by dendritic cells, and dampens NF-kB activation in macrophages
- Bioavailability — alkylamides are well-absorbed orally from tincture preparations, with detectable plasma concentrations within 30 minutes and persistence for several hours; the tongue-tingling sensation from a fresh tincture is direct evidence of alkylamide concentration
This CB2 mechanism explains why "Echinacea boosts the immune system" is a misleading characterization. Pure immune stimulation would worsen autoimmune disease, would worsen sepsis cytokine storms, and would worsen any inflammation-driven pathology. The CB2-mediated mechanism is the opposite — it dampens excessive inflammation while preserving the pathogen-clearance capacity of the immune system. This is what immunologists call immunomodulation rather than immunostimulation, and it has very different clinical implications.
Caffeic Acid Derivatives (Echinacoside, Cichoric Acid)
The caffeic acid derivatives are the polar phenolic constituents and act through several mechanisms distinct from the alkylamide-CB2 pathway:
- Antioxidant — the catechol moiety of caffeic acid is a potent free-radical scavenger. Echinacoside and cichoric acid both have high oxygen radical absorbance capacity (ORAC), reducing oxidative stress in inflamed tissue. This contributes to the symptomatic effect on cold severity (much of cold symptomatology comes from host inflammatory response and oxidative damage to upper airway epithelium, not from the virus itself)
- Hyaluronidase inhibition — many bacterial pathogens (Streptococcus, Staphylococcus, Clostridium) secrete hyaluronidase to break down the hyaluronic acid of host connective tissue and spread through tissue planes. Echinacoside and cichoric acid are competitive hyaluronidase inhibitors, slowing bacterial tissue spread. This is the proposed mechanism behind the traditional wound-healing applications.
- Direct antiviral activity — in vitro studies show caffeic acid derivatives interfere with viral attachment to host cells for rhinovirus, influenza A, and herpes simplex. The mechanism appears to be binding of phenolic OH groups to viral surface proteins, blocking the receptor-binding domain interaction with host cell receptors.
- Anti-inflammatory effects — caffeic acid derivatives inhibit cyclooxygenase and 5-lipoxygenase, reducing prostaglandin and leukotriene production. The effect is modest compared with NSAIDs but contributes to symptom relief.
The bioavailability challenge for the caffeic acid derivatives is significant. Echinacoside is poorly absorbed when given as the isolated compound (oral bioavailability under 1%) and is rapidly conjugated and excreted. The clinical effect appears to depend on the matrix — co-administration with the lipophilic alkylamides in a complete alcoholic tincture or pressed juice improves apparent bioavailability and tissue penetration relative to isolated compound. This is one of the reasons standardized whole-plant extracts have stronger trial signals than isolated-compound preparations.
High-Molecular-Weight Polysaccharides
The third major mechanism class is the high-molecular-weight polysaccharide fraction. The principal polysaccharides characterized from E. purpurea aerial parts are arabinogalactan-protein complexes and acidic heteroxylans with molecular weights in the 25-50 kDa range. These compounds act as immunostimulants in the traditional sense — they directly activate macrophages and dendritic cells through pattern-recognition receptors:
- Toll-like receptor 4 (TLR4) activation by acidic heteroxylans on macrophages, triggering NF-kB-mediated transcription of pro-inflammatory cytokines and antimicrobial peptides
- Dectin-1 and other C-type lectin receptor engagement by arabinogalactans, particularly on dendritic cells, enhancing antigen presentation and T-cell priming
- Complement activation — the alternative complement pathway is activated by some Echinacea polysaccharide fractions, contributing to the antimicrobial effect
The polysaccharide fraction is the constituent class that originally generated the autoimmune-contraindication concern (discussed in detail on the Safety page) — in-vitro studies of isolated arabinogalactan fractions did show Th1-type cytokine upregulation that, theoretically, could worsen autoimmune disease driven by Th1 dysregulation. The crucial caveat is that those in-vitro effects of isolated polysaccharides have not translated into clinical worsening of autoimmune disease in trials of whole-plant Echinacea preparations, because: (a) the alkylamide CB2 effect and the caffeic acid anti-inflammatory effect counterbalance the polysaccharide stimulation; (b) the polysaccharide fraction is partially or fully removed in concentrated alcoholic tinctures, the most common form patients take; (c) gut absorption of intact high-molecular-weight polysaccharides is limited, so much of the in-vitro signal does not translate to systemic effect after oral administration.
The practical implication is that the polysaccharide-mediated immunostimulation is most relevant for pressed-juice and water-extract preparations and for short-term high-dose at-onset use, and less relevant for the alcoholic tincture preparations used for prophylaxis.
Macrophage Activation and Cytokine Modulation
The macrophage is the prototypical effector cell of the innate immune system — it phagocytoses pathogens, presents antigen, secretes cytokines, and coordinates tissue inflammation. Echinacea preparations consistently demonstrate macrophage activation in vitro across multiple assay systems:
- Phagocytic activity — macrophages exposed to Echinacea extract show 30-60% increased phagocytosis of opsonized particles in standard assays
- Reactive oxygen species production — the macrophage respiratory burst (NADPH-oxidase-mediated superoxide production used for intracellular killing of phagocytosed pathogens) is enhanced
- Nitric oxide synthesis — inducible nitric oxide synthase (iNOS) is upregulated, increasing NO-mediated killing of intracellular pathogens
- Cytokine secretion modulation — the cytokine effect is the most nuanced. Crude Echinacea extracts produce a complex pattern: polysaccharide-driven increase in TNF-alpha, IL-1, and IL-6 (pro-inflammatory); alkylamide-driven decrease in TNF-alpha through CB2 binding (anti-inflammatory); net effect depending on preparation and dose
The cytokine-modulation pattern explains the term immunomodulator. In an underactivated immune system, Echinacea preparations tend to increase cytokine output and enhance pathogen clearance. In an overactivated immune system (excessive inflammation, autoimmune cytokine storms), the alkylamide-CB2 mechanism tends to dampen cytokine output. The net effect is restoration toward homeostasis rather than uniform stimulation.
Natural Killer Cell Stimulation
Natural killer (NK) cells are large granular lymphocytes of the innate immune system that recognize and kill virally-infected cells and tumor cells without requiring prior antigen sensitization. NK cell function is one of the more sensitive measures of innate immunocompetence and is significantly affected by Echinacea preparations:
- In healthy volunteers given oral Echinacea preparations, NK cell cytotoxic activity (measured by chromium-release assay against K562 target cells) typically increases 30-50% over baseline within 5-10 days of dosing
- NK cell number does not increase significantly — the enhancement is at the per-cell cytotoxic activity level
- The mechanism appears to be primarily polysaccharide-driven, with secondary contributions from interferon-gamma upregulation by macrophages
- NK enhancement persists for days after discontinuation, suggesting some durable receptor or gene-expression change rather than a purely acute pharmacological effect
The NK cell effect has been explored most extensively in the cancer-supportive-care literature, particularly in elderly populations where age-related NK decline contributes to increased infection susceptibility and possibly to increased tumor incidence. Trials of long-term Echinacea supplementation in geriatric populations have shown maintained NK cell function and reduced infection rates, though without specific cancer-prevention claims being supportable from current evidence.
Th1/Th2 Balance and Dendritic Cell Function
The adaptive immune system effects of Echinacea are subtler than the innate effects but are mechanistically interesting. Dendritic cells exposed to Echinacea preparations show altered cytokine secretion patterns that influence downstream T-cell differentiation:
- IL-12 modulation — dendritic cells exposed to Echinacea polysaccharide fractions secrete more IL-12, which pushes naive CD4+ T cells toward Th1 differentiation (cellular immunity, intracellular pathogen defense). This is the in-vitro observation that originally generated autoimmune-contraindication concerns.
- IL-10 modulation — alkylamide exposure increases IL-10 secretion, which is anti-inflammatory and pushes T cells toward the regulatory (Treg) phenotype. This counterbalances the IL-12 effect.
- Th17 effects — in chronic-inflammation models, Echinacea preparations tend to reduce Th17-mediated tissue damage, possibly through the CB2 mechanism and the IL-10 upregulation.
- Treg induction — alkylamide-driven CB2 activation modestly enhances Treg cell generation in vitro, contributing to the anti-inflammatory net effect.
The bottom line is that the in-vitro effects of Echinacea on T-cell differentiation are mixed, with both Th1-pushing and Treg-pushing signals depending on which constituent class dominates. In clinical trials of whole-plant preparations — which contain all three constituent classes — the net effect appears to be modulation toward balance rather than unidirectional Th1 push, which is consistent with the absence of observed autoimmune-disease flares in the Echinacea trial literature.
Why "Modulator" Not "Booster"
The phrase "immune booster" is one of the most overused and misleading terms in popular health writing. It implies that "more immune activity" is uniformly better, which is biologically false. An overactive immune system causes:
- Autoimmune disease (the immune system attacks self-tissue)
- Allergic disease (the immune system overreacts to harmless environmental antigens)
- Cytokine storms (sepsis, severe viral infections like influenza or SARS-CoV-2 historically, hemophagocytic lymphohistiocytosis)
- Chronic inflammation (the driver of cardiovascular disease, neurodegeneration, and many cancers)
The therapeutic ideal is not maximum immune activation but appropriate immune balance — vigorous response to genuine pathogen threats, tolerance of self-tissue and harmless environmental antigens, and prompt resolution of inflammation when the pathogen is cleared. This is the meaning of immunomodulator: an agent that pushes a dysregulated immune system back toward this balance, in either direction depending on which way the system is unbalanced.
Echinacea fits the modulator profile because:
- The alkylamide-CB2 mechanism dampens excessive inflammation
- The caffeic acid antioxidant effects reduce inflammation-driven tissue damage
- The polysaccharide-driven macrophage and NK activation enhances pathogen clearance when needed
- The dendritic-cell cytokine modulation pushes T-cell differentiation toward balanced Th1/Th2/Th17/Treg patterns rather than uniform expansion
The clinical translation is that Echinacea is most evidence-supported for situations where immune modulation is needed (cold and flu defense, post-illness recovery, low-grade chronic inflammation) and is not contraindicated — in current best evidence — in autoimmune disease where the older theoretical concern was based on isolated-constituent in-vitro studies rather than clinical observation.
Species and Preparation Distinction
The species and preparation determine which mechanism dominates in any given Echinacea product:
- E. angustifolia root alcoholic tincture — alkylamide-dominated. Strong CB2 mechanism, traditional Eclectic-physician preparation, good for at-onset cold use, intense tongue-tingling sensation indicating high alkylamide content. The polysaccharide fraction is largely removed by alcoholic extraction.
- E. purpurea aerial-parts pressed juice (Echinaforce) — balanced across all three mechanisms. Contains the cichoric acid (caffeic-acid derivative), alkylamides at moderate concentration, and the high-MW polysaccharides preserved by pressed-juice preparation. The strongest single-product trial evidence for prophylactic use.
- E. purpurea root tincture — alkylamide and cichoric acid present, polysaccharide fraction partially preserved depending on extraction method.
- E. pallida root preparation — echinacoside-dominated, lower alkylamides, primarily used in European market as substitute for E. angustifolia.
- Dried encapsulated Echinacea (any species) — alkylamides degrade in dried herb at room temperature, caffeic acid derivatives are reasonably stable, polysaccharide bioavailability is poor without alcoholic-extract matrix. Generally the weakest evidence-supported form.
For a patient looking to maximize the immune-modulation effect, the trial-supported choices are Echinaforce (most balanced across mechanisms, most evidence for cold prevention) or a high-quality E. angustifolia root tincture (most CB2 activation, best for at-onset use). Generic dried-herb capsules from low-cost mass-market brands are the least likely to deliver the intended pharmacological effect.
Clinical Translation
The three immune-modulation mechanisms translate into a specific clinical-use profile:
- Cold and flu prevention — the best-supported use; see the Cold and Flu Prevention deep-dive page for full trial review.
- Recovery from acute infection — the macrophage-activation and NK-stimulation mechanisms support the traditional use of Echinacea during convalescence from any acute viral or bacterial illness. The Cochrane review notes reduced cold severity and shorter recovery time as well as reduced incidence.
- Adjunctive use in chronic upper-respiratory inflammation — chronic sinusitis, recurrent otitis media, recurrent tonsillitis in patients with frequent post-infectious flares may benefit from prophylactic Echinacea. See the Sinusitis page.
- Wound healing — the hyaluronidase-inhibition mechanism (caffeic acid derivatives) and the local anti-inflammatory effect support traditional topical use on slow-healing wounds; see the Antimicrobial and Wound Healing page.
- Immune support in elderly populations — the documented effect on NK cell function in age-related immunosenescence is the rationale for long-term low-dose Echinacea in elderly patients; evidence is suggestive rather than definitive.
- Adjunctive use in cancer therapy — some small trials of Echinacea during chemotherapy have shown maintained leukocyte counts and reduced infection rates; this is an investigational use rather than a recommendation.
Echinacea is not appropriate for replacement of conventional immune therapy in severe disease — it is not a substitute for antibiotics in bacterial sepsis, for antivirals in severe influenza, or for immunosuppressants in autoimmune disease that requires them. The clinical niche is mild-to-moderate immune support in immunocompetent patients facing common-cold-level pathogen challenges and in convalescence from acute illness.
Key Research Papers
- Gertsch J, Schoop R, Kuenzle U, Suter A (2004). Echinacea alkylamides modulate TNF-alpha gene expression via cannabinoid receptor CB2 and multiple signal transduction pathways. FEBS Letters 577(3):563-569. — PubMed
- Woelkart K, Bauer R (2007). The role of alkamides as an active principle of echinacea. Planta Medica 73(7):615-623. — PubMed
- Raduner S, Majewska A, Chen JZ, Xie XQ, Hamon J, Faller B, Altmann KH, Gertsch J (2006). Alkylamides from Echinacea are a new class of cannabinomimetics. Cannabinoid type 2 receptor-dependent and -independent immunomodulatory effects. Journal of Biological Chemistry 281(20):14192-14206. — PubMed
- Spelman K, Burns J, Nichols D, Winters N, Ottersberg S, Tenborg M (2006). Modulation of cytokine expression by traditional medicines: a review of herbal immunomodulators. Alternative Medicine Review 11(2):128-150. — PubMed
- Goel V, Lovlin R, Chang C, Slama JV, Barton R, Gahler R, Bauer R, Goonewardene L, Basu TK (2005). A proprietary extract from the echinacea plant (Echinacea purpurea) enhances systemic immune response during a common cold. Phytotherapy Research 19(8):689-694. — PubMed
- Sullivan AM, Laba JG, Moore JA, Lee TD (2008). Echinacea-induced macrophage activation. Immunopharmacology and Immunotoxicology 30(3):553-574. — PubMed
- Burger RA, Torres AR, Warren RP, Caldwell VD, Hughes BG (1997). Echinacea-induced cytokine production by human macrophages. International Journal of Immunopharmacology 19(7):371-379. — PubMed
- See DM, Broumand N, Sahl L, Tilles JG (1997). In vitro effects of echinacea and ginseng on natural killer and antibody-dependent cell cytotoxicity in healthy subjects and chronic fatigue syndrome or acquired immunodeficiency syndrome patients. Immunopharmacology 35(3):229-235. — PubMed
- Currier NL, Miller SC (2000). Natural killer cells from aging mice treated with extracts from Echinacea purpurea are quantitatively and functionally rejuvenated. Experimental Gerontology 35(5):627-639. — PubMed
- Brovelli EA, Rua D, Roh-Schmidt H, Chandra A, Lamont E, Noratto GD (2005). Human gene expression as a tool to determine horticultural maturity in a bioactive plant (Echinacea purpurea). Journal of Agricultural and Food Chemistry 53(21):8156-8161. — PubMed
- Senchina DS, McCann DA, Asp JM, Johnson JA, Cunnick JE, Kaiser MS, Kohut ML (2005). Changes in immunomodulatory properties of Echinacea spp. root infusions and tinctures stored at 4 degrees C for four days. Clinica Chimica Acta 355(1-2):67-82. — PubMed
- Stevenson LM, Matthias A, Banbury L, Penman KG, Bone KM, Leach DL, Lehmann RP (2005). Modulation of macrophage immune responses by Echinacea. Molecules 10(10):1279-1285. — PubMed
PubMed Topic Searches
- PubMed: Echinacea alkylamide CB2 cannabinoid
- PubMed: Echinacea macrophage activation
- PubMed: Echinacea NK cell function
- PubMed: Echinacea polysaccharide immunostimulant
- PubMed: Echinacea caffeic acid derivatives
Connections
- Echinacea Overview
- Echinacea Benefits Hub
- Echinacea Cold & Flu Prevention
- Echinacea Antimicrobial & Wound Healing
- Echinacea Safety & Autoimmune Cautions
- Immune Boosting
- Astragalus
- Elderberry
- Reishi
- Andrographis
- Goldenseal
- Quercetin
- Vitamin C
- Vitamin D3
- Zinc