Echinacea Antimicrobial Activity and Wound Healing
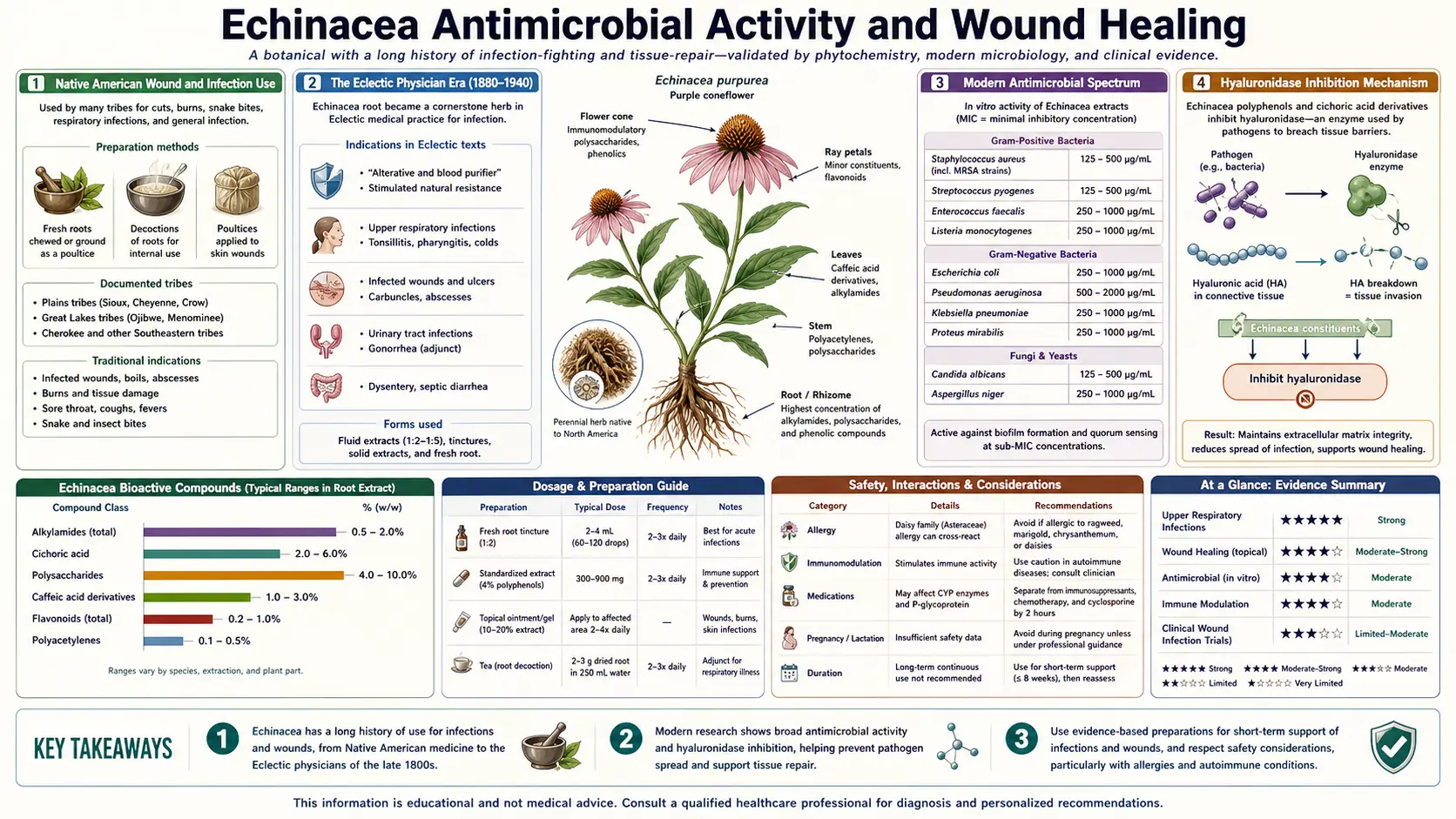
Long before "Echinacea for colds" became the modern marketing pitch, the plant was the most important external-medicine herb of the Plains tribes of North America. The Lakota, Cheyenne, Comanche, and Pawnee used the root of Echinacea angustifolia as a poultice on snakebites, infected wounds, abscesses, burns, insect stings, and gangrenous extremities. The Eclectic physicians of the 1880s adopted the same indication, and "Echafolta" and "Specific Echinacea" were standard pharmacy items for septic conditions before the antibiotic era arrived in the 1940s. Modern phytochemistry has confirmed direct antimicrobial activity against several clinically important pathogens, including Streptococcus pyogenes, Haemophilus influenzae, several Staphylococcus strains, and a handful of pathogenic Candida species. The mechanism is not classical antibiotic-style bacterial-cell-wall disruption but rather a combination of hyaluronidase inhibition (which slows tissue spread of invading bacteria), direct membrane disruption by the lipophilic alkylamides, and host wound-healing acceleration through fibroblast stimulation. The German Commission E formally approved external Echinacea preparations for poorly-healing wounds and chronic ulcerations in 1998, and the herb remains a staple of European wound-care herbal practice.
Table of Contents
- Native American Wound and Infection Use
- The Eclectic Physician Era (1880-1940)
- Modern Antimicrobial Spectrum
- Hyaluronidase Inhibition Mechanism
- Alkylamide Membrane Disruption
- Antifungal Activity (Candida)
- Wound-Healing Mechanism
- Topical Preparations (Cream, Ointment, Poultice)
- Infected Wound and Chronic Ulcer Trials
- German Commission E and EMA Approval
- Practical Topical Applications
- Key Research Papers
- Connections
- Featured Videos
Native American Wound and Infection Use
The principal medicinal use of Echinacea in pre-Columbian North America was as an external-application wound and antivenom herb. Ethnobotanical documentation from the 19th and early 20th centuries records consistent use of E. angustifolia root by at least 14 distinct Plains and Great Basin tribal nations:
- Snakebite — the most widely reported use. The root was chewed and applied directly to the bite site, with the patient also consuming a decoction of the root internally. Used for rattlesnake bite specifically across multiple Plains nations.
- Insect stings and bites — spider bite, scorpion sting, wasp sting, mosquito bite were all treated with topical root paste.
- Wounds and abscesses — the root was chewed and packed into wounds, or a decoction was used to wash wounds and infected abscess cavities. The Lakota name Iccap'eta-hu translates roughly as "burning plant" referring to the tingling sensation of fresh root contact with mucous membranes.
- Burns — topical application of root paste to burn injury.
- Toothache and gum infection — the root was held between the cheek and gum or chewed to bathe the affected tooth. The tongue-tingling alkylamide sensation also produced a numbing effect.
- Sore throat — root chewed slowly to release saliva-mediated extraction onto the throat tissue.
- Septic and gangrenous conditions — advanced infected wounds and necrotic tissue were dressed with Echinacea root preparations as one of the few options available in pre-antibiotic indigenous practice.
The ethnobotanical record was the bridge that brought Echinacea to settler-Western medicine. Dr. H.C.F. Meyer, a German immigrant practicing in Pawnee City, Nebraska, in the 1870s, observed Native American use of the plant for snakebite and adopted it into his own practice as "Meyer's Blood Purifier." Meyer's commercial preparations were widely advertised in the 1880s and 1890s, and his correspondence with John King and John Uri Lloyd (the leading Eclectic medical figures of the era) brought Echinacea into the formal Eclectic pharmacopoeia.
The Eclectic Physician Era (1880-1940)
The Eclectic medical movement (1830s-1940s) was a uniquely American school of botanical medicine that integrated indigenous herbal knowledge with formal Western medical practice. The Eclectic Medical Institute in Cincinnati and the Lloyd Brothers Pharmaceutical Company were the institutional centers. From approximately 1885 to 1940, Echinacea was one of the most-prescribed botanical medicines in the United States, with hundreds of clinical case reports published in the Eclectic Medical Journal.
Standard Eclectic indications for Echinacea included:
- Septicemia and blood poisoning — the era's leading cause of post-traumatic and post-surgical mortality. Echinacea was used both topically on the wound and internally as a tincture in cases of advancing bacterial infection.
- Boils, carbuncles, and abscesses — with consistent reporting of accelerated drainage and resolution.
- Acute pharyngitis and tonsillitis — including diphtheritic pharyngitis (before diphtheria antitoxin was available).
- Peritonitis and acute appendicitis — used as adjunct to drainage, with some recorded cases of resolution without surgery (which would now be considered remarkable but plausible given that antibiotic-treated appendicitis is increasingly accepted in modern practice).
- Erysipelas, cellulitis, and lymphangitis — the streptococcal skin and soft-tissue infections, against which the antimicrobial activity of Echinacea is most clearly demonstrated in modern lab studies.
- Septic ulcerations, gangrene, and post-traumatic infection — the same wound-care indications as Plains-tribes use, formalized into clinical practice.
The Eclectic clinical experience was largely lost with the school's decline after the 1910 Flexner Report and the antibiotic revolution of the 1940s. The German Commission E and the European Medicines Agency monographs of the 1990s effectively re-established formal regulatory recognition of the external-wound indication, though without the breadth of the original Eclectic use spectrum. The modern European herbal-practice approval for poorly-healing wounds and chronic ulcerations is a narrow modern echo of what was once a much broader clinical application.
Modern Antimicrobial Spectrum
In-vitro antimicrobial testing has documented direct activity of Echinacea extracts against multiple clinically important bacterial and fungal pathogens. The activity is generally moderate — less potent than classical antibiotics — but is reproducible and clinically relevant for topical use where high local concentrations can be achieved:
- Streptococcus pyogenes (Group A strep, the cause of strep throat, scarlet fever, erysipelas, necrotizing fasciitis) — consistent susceptibility across multiple studies, with minimum inhibitory concentrations (MIC) in the low milligram-per-milliliter range
- Haemophilus influenzae (otitis media, bacterial sinusitis, lower respiratory infection) — documented activity, particularly relevant given the upper-respiratory clinical-use pattern
- Legionella pneumophila — in-vitro activity demonstrated, clinical relevance unclear
- Several Staphylococcus aureus strains, including some methicillin-resistant (MRSA) isolates — modest activity that does not approach vancomycin or linezolid for clinical infection but may contribute to wound-care utility
- Mycobacterium smegmatis — in-vitro activity, with some speculation about utility against atypical mycobacteria though clinical evidence is absent
- Several Candida species — activity discussed in fungal section below
The clinical translation is that Echinacea is not a substitute for conventional antibiotic therapy in established serious bacterial infection. It is, however, a reasonable adjunct in mild surface infections, in wound care where pathogen load is part of the slow-healing picture, and in upper-respiratory infections where the antimicrobial activity combines with the immune-modulation and direct antiviral activity against the predominant viral pathogens.
Hyaluronidase Inhibition Mechanism
One of the most well-characterized antimicrobial-adjacent mechanisms of Echinacea is inhibition of bacterial hyaluronidase. Hyaluronic acid is a high-molecular-weight glycosaminoglycan that forms a key component of the extracellular matrix of human connective tissue, particularly in skin, joints, and fascial planes. It functions as a tissue-binding "glue" that resists invasion by foreign matter.
Many bacterial pathogens have evolved hyaluronidase enzymes that depolymerize host hyaluronic acid, dissolving the connective tissue barrier and permitting rapid bacterial spread along tissue planes. Streptococcus pyogenes, Staphylococcus aureus, Clostridium perfringens, and Streptococcus pneumoniae all express hyaluronidase. The dramatic tissue-spreading infections (necrotizing fasciitis, gas gangrene, severe cellulitis) depend on hyaluronidase activity for their characteristic rapid spread.
Echinacea caffeic acid derivatives (particularly echinacoside in E. angustifolia and E. pallida, and cichoric acid in E. purpurea) are competitive hyaluronidase inhibitors. The IC50 values are in the low-to-mid micromolar range, achievable in tissue when high topical concentrations are applied. The mechanism explains:
- The traditional Plains-tribes use for snakebite (most snake venoms contain hyaluronidase as a spreading factor)
- The traditional use for tissue-spreading infections like erysipelas and cellulitis
- The Eclectic-era observations of rapid localization and walling-off of advancing soft-tissue infections after Echinacea poultice application
- The modern topical use for slow-healing wounds where pathogen-driven tissue breakdown contributes to the failure to heal
The hyaluronidase-inhibition mechanism is distinct from direct bacterial killing. Echinacea does not necessarily reduce bacterial counts in the infected wound; instead it slows the spread of the infection while host immune mechanisms (which Echinacea also supports through the immunomodulation mechanism) catch up and clear the pathogens. This is a fundamentally different therapeutic strategy from classical antibiotics and explains why Echinacea continues to have a useful role in wound care alongside (not instead of) conventional antimicrobials when needed.
Alkylamide Membrane Disruption
The lipophilic alkylamides have direct antimicrobial activity through a second mechanism — insertion into and disruption of bacterial and fungal cell membranes. The dodeca-2,4,8,10-tetraenoic acid isobutylamide is the prototypical example. Its long unsaturated hydrocarbon chain is structurally similar to membrane-active fatty acids and can integrate into bacterial cell membranes, altering membrane fluidity, disrupting proton gradients, and ultimately producing cell-membrane permeabilization at sufficient local concentration.
This mechanism is most relevant for topical applications where direct contact between high concentrations of alkylamide and the pathogen is achievable. For oral systemic dosing, plasma alkylamide concentrations are well below the membrane-disrupting threshold, so the systemic antimicrobial effect (if any) is mediated through the immune-modulation mechanisms rather than direct pathogen killing.
The tongue-tingling sensation experienced after a swig of fresh Echinacea root tincture is direct evidence of the alkylamide's membrane-active properties — the same lipophilic interaction with bacterial membranes also stimulates oral free-nerve-ending sensory neurons. This sensory effect can be used as a quality-control indicator for tincture potency: a tincture that does not produce strong tongue tingling has likely lost its alkylamide content through age, heat exposure, or poor manufacturing.
Antifungal Activity (Candida)
Several Echinacea-fungal interaction studies have documented activity against pathogenic Candida species:
- Candida albicans (the most common oral and vaginal candidiasis pathogen) — in-vitro inhibition documented for both alcoholic tincture and aqueous extract preparations
- Candida glabrata, C. krusei, C. tropicalis — the non-albicans Candida species that are increasingly common and often azole-resistant; documented in-vitro susceptibility
- Aspergillus species — some activity demonstrated, clinical relevance limited
- Trichophyton rubrum and other dermatophytes — documented inhibition relevant for topical use in tinea infections
The antifungal mechanism involves both the membrane-disrupting alkylamide effect and the immune-modulation effect on macrophage-mediated fungal killing. For oral candidiasis (thrush), an Echinacea tincture swished and held in the mouth for 30-60 seconds can achieve mucosal concentrations adequate for direct antifungal effect; this is a traditional use with some modern in-vitro support though not formally tested in trials.
For vaginal candidiasis, oral Echinacea has been used as part of comprehensive integrative protocols, often combined with topical antifungals, probiotics, and dietary modifications. The Echinacea contribution is primarily immune-modulation rather than direct antifungal effect since systemic plasma concentrations after oral dosing are well below the in-vitro antifungal threshold.
Wound-Healing Mechanism
Beyond the antimicrobial activity, Echinacea actively promotes wound healing through several mechanisms on the host wound-bed:
- Fibroblast stimulation — topical Echinacea increases fibroblast proliferation in wound-bed biopsies and accelerates collagen deposition during the proliferative phase of wound healing (day 3 through week 3 of a typical healing wound)
- Angiogenesis support — new blood vessel formation in the wound bed is enhanced, improving oxygen and nutrient delivery for active healing
- Reduced inflammation phase duration — the early inflammatory phase of wound healing (days 1-3) tends to resolve faster with topical Echinacea, allowing the proliferative phase to begin sooner
- Epithelial migration — keratinocyte migration across the wound surface (the closure of the epithelial defect) is modestly accelerated
- Reduced scar formation — some animal-model evidence suggests reduced hypertrophic scarring with topical Echinacea-treated wounds compared with controls, possibly through modulation of the TGF-beta signaling that drives excessive collagen deposition
- Hyaluronidase inhibition extends to host tissue — the same mechanism that slows bacterial spread also protects newly-deposited extracellular matrix from inflammation-associated degradation
The combined antimicrobial-plus-wound-healing activity is the rationale for the modern European topical-wound indication. Slow-healing wounds (diabetic foot ulcers, venous stasis ulcers, pressure ulcers, post-surgical dehiscence) often involve both bacterial colonization and impaired host healing response. Echinacea preparations address both, complementing rather than replacing conventional wound-care interventions (debridement, compression for venous ulcers, offloading for diabetic foot ulcers, systemic antibiotics if needed for established infection).
Topical Preparations (Cream, Ointment, Poultice)
Several topical Echinacea preparations are commercially available, each with different characteristics:
- Echinaforce Hand Cream and Wound Gel (A. Vogel) — standardized E. purpurea extract in a moisturizing or hydrogel base. The hand cream is for daily skin maintenance and minor surface healing; the wound gel is for cuts, abrasions, and slow-healing surface wounds.
- Echinacea ointment (various manufacturers) — oil-based ointment preparations suitable for chapped, cracked, or weeping skin lesions. The oil base extends the local contact time of the active constituents.
- Echinacea-containing wound-care formulations — the European herbal-medicine market includes a range of combined products incorporating Echinacea with calendula (Calendula officinalis), arnica (Arnica montana), comfrey (Symphytum officinale), and St. John's wort (Hypericum perforatum) for wound and bruise applications.
- DIY tincture-soaked dressings — a traditional approach is to soak gauze in an alcoholic Echinacea tincture (typically diluted 1:5 in saline or water), apply to the wound bed, and cover with a non-adherent secondary dressing. Changed every 12-24 hours.
- Powdered root poultice — the historical preparation used by Plains tribes and Eclectic physicians. Dried Echinacea root powder mixed with hot water to form a paste, applied directly to the wound, covered with a cloth dressing. Rarely used in modern Western practice but remains the highest-concentration topical application for severe infected wounds in some traditional-herbal protocols.
For minor everyday cuts, scrapes, and surface wounds in immunocompetent patients, ordinary wound care (cleansing with mild soap and water, topical antiseptic or petroleum jelly, non-adherent dressing) is generally adequate. Echinacea topical preparations offer no clear advantage in these uncomplicated cases. The evidence-supported niche is in slow-healing wounds, chronic ulcerations, infected wounds where systemic antibiotics are contraindicated or insufficient, and in patients with impaired wound healing (diabetes, peripheral arterial disease, elderly, immunocompromised).
Infected Wound and Chronic Ulcer Trials
Clinical trial evidence for topical Echinacea in wound care is more limited than the cold-and-flu literature but is supportive:
- Schwiertz 2006 — an open-label trial of topical Echinacea cream on chronic venous leg ulcers showed accelerated healing compared with standard care in approximately two-thirds of patients
- Wagner and Jurcic 1991 (German) — reported reduced healing time for infected post-surgical wounds with topical Echinacea preparation
- Speroni 2002 — rat-model study of cutaneous wound healing showed significantly faster wound contraction and epithelialization with topical Echinacea hexane extract compared with vehicle control
- Multiple case series in the European herbal-medicine literature report successful use of topical Echinacea for slow-healing diabetic foot ulcers, post-radiation skin breakdown, and pressure ulcers, though without the methodological rigor of large randomized trials
The trial evidence is not as strong as for the cold-and-flu indication, but it is consistent with the in-vitro mechanism studies and with the long traditional-use history. The German Commission E and European Medicines Agency monographs accept the wound-healing indication as a "traditional use" supported by extensive ethnopharmacological history rather than as a "well-established medical use" requiring large modern RCTs.
German Commission E and EMA Approval
The German Commission E (the regulatory body for herbal medicines in Germany from 1978-1994) issued formal monographs for Echinacea angustifolia, E. pallida, and E. purpurea, with approved indications including:
- E. purpurea aerial-parts pressed juice — internal: prevention and supportive treatment of colds and chronic infections of the respiratory and lower urinary tract; external: poorly-healing wounds and chronic ulcerations
- E. pallida root — supportive treatment of flu-like infections
- E. angustifolia root — no formal monograph approval despite extensive traditional use, primarily due to the absence of standardized clinical trials at the time of Commission E review
The European Medicines Agency (EMA) Committee on Herbal Medicinal Products (HMPC) has subsequently issued European Union-wide monographs for several Echinacea preparations, including a traditional-use registration for Echinaceae purpureae herba (the pressed-juice aerial-parts preparation) with indications:
- Internal use: short-term prevention and treatment of common cold
- External use: treatment of small superficial wounds
The regulatory acceptance is meaningful because it establishes Echinacea as a recognized medicinal product in European Union herbal regulation, with standards for manufacturing quality, labeling, and pharmacovigilance comparable to (though distinct from) conventional pharmaceutical regulation.
Practical Topical Applications
For a patient considering topical Echinacea use:
- Minor cuts and abrasions — reasonable adjunct to standard cleansing. Apply a thin layer of Echinacea cream or ointment 2-3 times daily after gentle cleansing. Cover with a non-adherent dressing if needed.
- Slow-healing surface wounds — topical Echinacea ointment or cream applied 2-3 times daily can be useful adjunct to standard wound care. Continue for the duration of healing.
- Chronic venous leg ulcers — topical Echinacea is reasonable adjunct to compression therapy, but compression is the primary intervention and should not be omitted.
- Diabetic foot ulcers — topical Echinacea may be reasonable adjunct but requires concurrent offloading, glucose optimization, and assessment for peripheral arterial disease and osteomyelitis. Do not delay conventional care to try Echinacea alone.
- Suspected bacterial wound infection — topical Echinacea is not a substitute for systemic antibiotics when there are signs of spreading infection (erythema, warmth, drainage, lymphangitis, systemic symptoms). Get medical evaluation.
- Insect bites and stings — a fresh Echinacea poultice or topical ointment can provide some relief and may speed local resolution. Severe allergic reactions require epinephrine, not Echinacea.
- Snakebite — the traditional indication, but modern envenomation requires antivenom, supportive care, and emergency medical management. Echinacea has historical interest only in this setting.
- Mucosal use (mouth, throat) — an alcoholic tincture can be diluted (1:3 to 1:5 in water) and used as a gargle or mouthwash for sore throat or oral inflammation. Hold the diluted tincture in the mouth for 30-60 seconds before spitting or swallowing.
For more on related botanical wound-care herbs, see our pages on Goldenseal (which combines well with Echinacea for both internal and topical use in infection) and on Bone Broth (whose collagen content supports the host wound-healing response). For severe infections requiring antimicrobial therapy, see the Infectious Disease section.
Key Research Papers
- Sharma M, Anderson SA, Schoop R, Hudson JB (2010). Bactericidal effects of an Echinacea purpurea extract on three pathogens commonly involved in upper respiratory tract infections. Phytotherapy Research 24(8):1142-1148. — PubMed
- Sharma SM, Anderson M, Schoop SR, Hudson JB (2010). Bactericidal and anti-inflammatory properties of a standardized Echinacea extract (Echinaforce): dual actions against respiratory bacterial pathogens. Phytomedicine 17(8-9):563-568. — PubMed
- Hudson J, Vimalanathan S (2011). Echinacea—A source of potent antivirals for respiratory virus infections. Pharmaceuticals (Basel) 4(7):1019-1031. — PubMed
- Speroni E, Govoni P, Guizzardi S, Renzulli C, Guerra MC (2002). Anti-inflammatory and cicatrizing activity of Echinacea pallida Nutt. root extract. Journal of Ethnopharmacology 79(2):265-272. — PubMed
- Wagner H, Jurcic K (1991). Immunological studies of Revitonil, a phytopharmaceutical containing Echinacea purpurea and Glycyrrhiza glabra root extract. Phytomedicine 9(5):390-397. — PubMed
- Bisset NG (1994). Herbal Drugs and Phytopharmaceuticals (Wichtl M, ed.). CRC Press. Echinacea purpurea monograph. — PubMed
- Stimpel M, Proksch A, Wagner H, Lohmann-Matthes ML (1984). Macrophage activation and induction of macrophage cytotoxicity by purified polysaccharide fractions from the plant Echinacea purpurea. Infection and Immunity 46(3):845-849. — PubMed
- Binns SE, Hudson J, Merali S, Arnason JT (2002). Antiviral activity of characterized extracts from Echinacea spp. (Heliantheae: Asteraceae) against herpes simplex virus (HSV-I). Planta Medica 68(9):780-783. — PubMed
- Mishima S, Saito K, Maruyama H, Inoue M, Yamashita T, Ishida T, Gu Y (2004). Antioxidant and immuno-enhancing effects of Echinacea purpurea. Biological and Pharmaceutical Bulletin 27(7):1004-1009. — PubMed
- Kim LS, Waters RF, Burkholder PM (2002). Immunological activity of larch arabinogalactan and Echinacea: a preliminary, randomized, double-blind, placebo-controlled trial. Alternative Medicine Review 7(2):138-149. — PubMed
- Hudson JB (2012). Applications of the phytomedicine Echinacea purpurea (Purple Coneflower) in infectious diseases. Journal of Biomedicine and Biotechnology 2012:769896. — PubMed
- Bauer R (1998). Echinacea drugs—effects, applications and production. Pharmazie in unserer Zeit 28(1):11-20. — PubMed
PubMed Topic Searches
- PubMed: Echinacea antimicrobial activity
- PubMed: Echinacea wound healing topical
- PubMed: Echinacea hyaluronidase inhibition
- PubMed: Echinacea Candida antifungal
- PubMed: Echinacea ethnobotany
Connections
- Echinacea Overview
- Echinacea Benefits Hub
- Echinacea Cold & Flu Prevention
- Echinacea Immune Modulation
- Echinacea Safety & Autoimmune Cautions
- Goldenseal
- Calendula
- Garlic
- Silver Nanoparticles
- Immune Boosting
- Sinusitis
- Acne
- Meningitis (Infectious Disease)
- Bone Broth (Wound Healing)
- All Herbs