Echinacea for Cold and Flu Prevention
Echinacea is the most-studied herb in the world for the common cold, with more than two dozen randomized controlled trials and several large meta-analyses. The headline finding from the Shah 2007 Lancet Infectious Diseases meta-analysis is that Echinacea reduces cold incidence by approximately 58% and shortens cold duration by approximately 1.4 days compared with placebo, but those numbers conceal a large amount of preparation-by-preparation variability. The 2014 Karsch-Volk Cochrane review of 24 trials confirmed a modest but real benefit, particularly for the Echinaforce pressed-juice preparation of E. purpurea aerial parts taken prophylactically. This deep-dive walks through the major trials, the preparation-method variable that determines whether a given study shows benefit or null, the prophylaxis-versus-at-onset distinction, the species and plant-part differences that explain the inconsistency, and what to actually buy and how to dose it.
Table of Contents
- The Common Cold — Burden and Therapeutic Gap
- The Shah 2007 Meta-Analysis — The 58% Number
- The Karsch-Volk 2014 Cochrane Review
- The Echinaforce Trial — Prophylactic E. purpurea Pressed Juice
- Three Species, Different Chemistry, Different Trial Results
- Root vs Aerial Parts — Why It Matters
- Prophylaxis vs At-Onset Treatment
- The Negative Trials (Turner 2005, Barrett 2010)
- Influenza — What the Evidence Does and Doesn't Show
- Practical Patient Protocol
- Key Research Papers
- Connections
- Featured Videos
The Common Cold — Burden and Therapeutic Gap
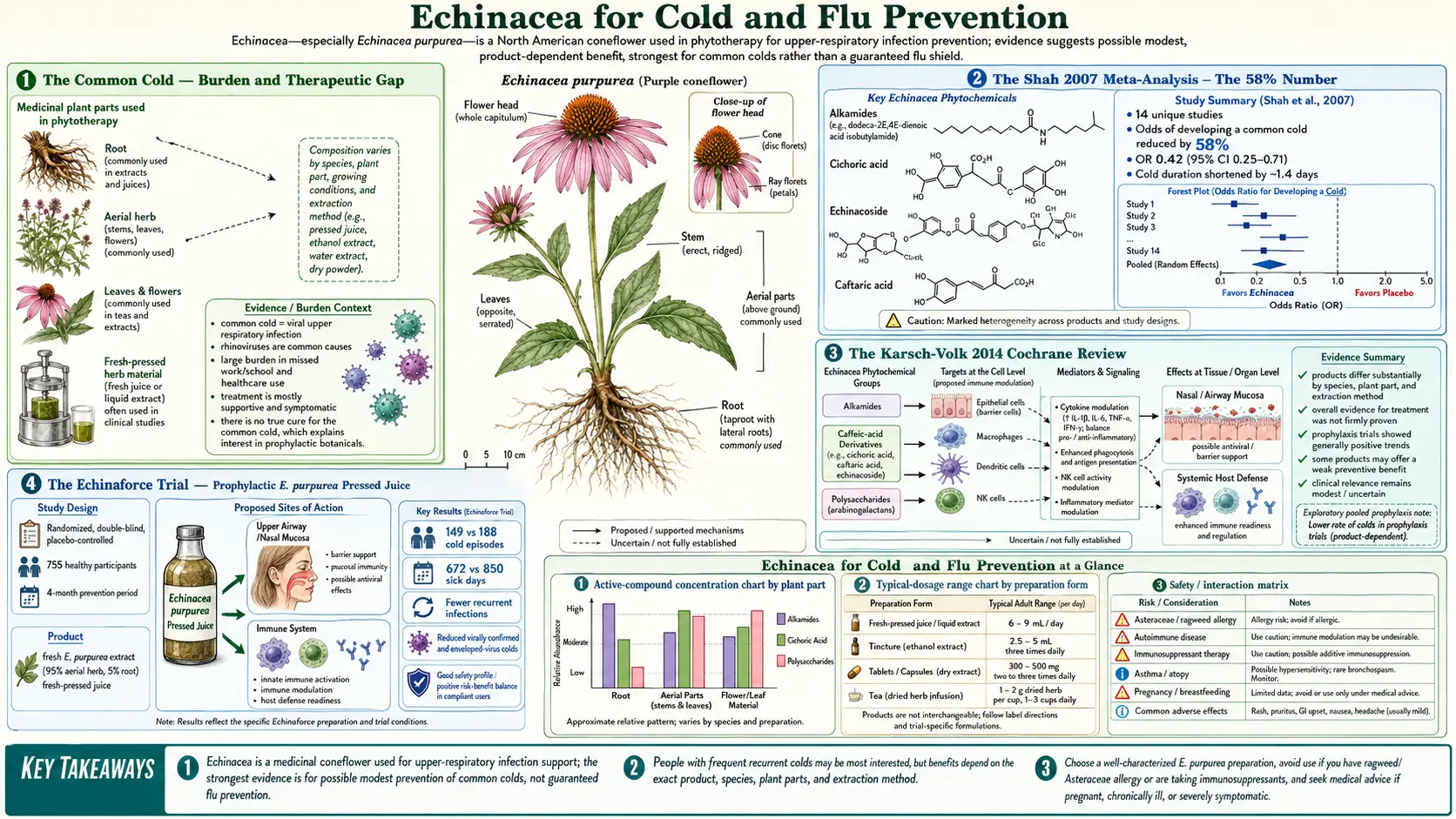
The common cold (acute viral rhinopharyngitis) is the most common acute illness in the developed world. The average adult experiences two to three episodes per year, the average school-age child six to ten. The economic burden in the United States alone is estimated at $40 billion annually in direct medical costs plus lost productivity. There is no curative therapy — the more than 200 rhinoviruses and dozens of coronavirus, parainfluenza, RSV, and adenovirus serotypes that cause colds make vaccine development effectively impossible.
The conventional pharmacy aisle for cold treatment is mostly symptomatic: decongestants (pseudoephedrine, oxymetazoline), antihistamines, expectorants (guaifenesin), antitussives (dextromethorphan), and analgesic-antipyretics (acetaminophen, ibuprofen). None of these shorten the underlying viral illness; they only blunt the symptoms while the immune system clears the infection over five to ten days. Antibiotics are inappropriate and harmful for viral colds — they don't help the virus, they kill the patient's commensal microbiome, and they drive antibiotic resistance.
The therapeutic gap is exactly the niche Echinacea occupies in the popular pharmacopoeia. Roughly 10 million U.S. adults take Echinacea annually, the great majority for cold or flu. It is the second-most-used botanical in the country after ginseng. The clinical question is whether the popular use is supported by evidence. The answer, properly stratified by preparation, is a qualified yes — for some products taken in some patterns, there is a real but modest benefit.
The Shah 2007 Meta-Analysis — The 58% Number
The most-cited single statistic on Echinacea comes from Shah and colleagues at the University of Connecticut, published in The Lancet Infectious Diseases in July 2007. The authors pooled 14 placebo-controlled randomized trials and reported two headline numbers:
- Incidence reduction: 58% — the odds ratio for developing a cold while taking Echinacea (any preparation, any species) compared with placebo was 0.42 (95% confidence interval 0.25-0.71)
- Duration reduction: 1.4 days — weighted mean difference in cold duration between Echinacea and placebo arms across the trials
Those numbers received enormous press coverage, including front-page treatment in The New York Times, and remain the most widely-quoted figures on Echinacea efficacy. They were also immediately controversial. Critics pointed out that the meta-analysis pooled wildly heterogeneous preparations (root vs aerial; tincture vs pressed juice vs encapsulated dry herb; E. purpurea vs E. angustifolia vs E. pallida vs combinations) and used statistical methods that the critics argued exaggerated the apparent benefit. The Shah authors defended their methods as appropriate given the underlying biology of the herb — the assumption being that the active mechanisms are common to all species and preparations even if the constituent ratios differ.
The 2014 Karsch-Volk Cochrane review (next section) revisited the same evidence base with more rigorous methods and reached a more measured conclusion: a small but statistically significant benefit, smaller than the 58% Shah number, and concentrated in specific preparations rather than uniform across Echinacea products.
The Karsch-Volk 2014 Cochrane Review
The definitive evidence synthesis is the Cochrane systematic review by Karsch-Volk and colleagues, published in February 2014 as Cochrane Database of Systematic Reviews Issue 2: CD000530, an update of earlier 1999 and 2009 versions. The review included 24 randomized controlled trials with a combined enrollment of 4,631 participants. Key findings:
- Prevention trials — pooled across all preparations, the effect of Echinacea on cold incidence reached borderline statistical significance (risk ratio approximately 0.83), suggesting a roughly 10-20% relative risk reduction. The effect was somewhat larger and more clearly significant in trials of E. purpurea aerial-parts pressed-juice (Echinaforce) preparations taken prophylactically.
- Treatment trials — trials starting Echinacea at symptom onset rather than prophylactically showed less consistent benefit. A few trials demonstrated reduced duration; others showed no difference.
- Adverse events — no significant difference between Echinacea and placebo for any adverse event, including the immune-related events that the autoimmune-contraindication concern would predict. Rates of rash and gastrointestinal upset were marginally higher in Echinacea arms but the difference was not statistically significant.
The Cochrane authors emphasized a critical methodological point that is essential to understanding the Echinacea literature: "the trials included in this review were highly heterogeneous regarding the type of Echinacea preparation used, the species of plant, the part of plant used, the extraction method, the dose, and the duration of the intervention." The authors specifically singled out the Echinaforce E. purpurea pressed-juice preparation as having the most consistent benefit signal and recommended that future trials standardize preparation more carefully to test specific products rather than the genus broadly.
The bottom-line Cochrane conclusion: "Echinacea products may have a weak benefit on the duration and severity of colds but the size and clinical relevance of the effect are uncertain." This is a notably less enthusiastic conclusion than the Shah 58% meta-analysis, but the two findings are not actually in conflict — both confirm that the average effect across all Echinacea preparations is positive, while emphasizing that the magnitude depends critically on which product is being used.
The Echinaforce Trial — Prophylactic E. purpurea Pressed Juice
The largest and most methodologically rigorous Echinacea trial is the 2012 randomized double-blind placebo-controlled trial by Jawad and colleagues published in Evidence-Based Complementary and Alternative Medicine. The trial enrolled 755 healthy adults randomized to either Echinaforce (an alcoholic extract of freshly-pressed E. purpurea aerial parts, manufactured by A. Vogel Bioforce of Switzerland) or matching placebo, taken three times daily for four months during the cold season. The trial captured 282 cold episodes by symptom diary.
Results were notable:
- Total days of cold symptoms over four months: 149 days in the Echinaforce arm vs 188 days in placebo (P = 0.024)
- Incidence of cold episodes: relative risk reduction of approximately 26% in the Echinaforce arm
- Time off work due to cold symptoms: significantly reduced
- Adverse-event profile: identical between arms, no significant safety signals
- Notably, episodes of recurrent and complicated colds (needing antibiotic or analgesic intervention) were reduced by 65% in the Echinaforce arm
The Echinaforce trial is the strongest single piece of clinical evidence for Echinacea cold prevention and is the trial most directly supporting practical patient use. The preparation specifics matter — it is the alcoholic extract of freshly-pressed aerial parts of E. purpurea at a specific extraction ratio, not a generic Echinacea capsule. Generic "Echinacea" capsules in the supplement aisle vary enormously in species, plant part, and preparation method, and many are not equivalent to the trial preparation.
Three Species, Different Chemistry, Different Trial Results
The genus Echinacea contains nine species native to North America, but only three are in significant commercial cultivation:
- E. purpurea — the most widely cultivated species, recognizable by its purple petals with a prominent orange-spiked central cone. Highest in cichoric acid (a caffeic acid derivative), present in alkylamides at moderate concentration, contains substantial high-molecular-weight polysaccharides in aerial parts. Used in pressed-juice (Echinaforce) and tincture preparations, both aerial parts and root.
- E. angustifolia — the species used most extensively by the Plains tribes of North America, the species adopted by the Eclectic physicians of the late 1800s, and the species used in the original European clinical research. Highest in alkylamides (the tongue-tingling lipophilic CB2-binding compounds) and in echinacoside. Lower in cichoric acid. Typically used as a root tincture.
- E. pallida — the pale purple coneflower. High in echinacoside but lower in alkylamides than E. angustifolia. Historically used as a substitute for E. angustifolia when the latter was scarce, and frequently adulterates E. angustifolia products in the marketplace.
The three species are not interchangeable in trials. A meta-analysis that pools, for example, a E. purpurea aerial-parts pressed juice with an E. angustifolia root alcoholic tincture is essentially averaging two different drugs. The Karsch-Volk Cochrane review explicitly stratified by preparation type when possible, and noted that the pressed-juice Echinaforce preparation drove much of the positive signal. Trials of E. angustifolia alcoholic root tinctures have shown more variable results, partly because the alcoholic extraction loses the polysaccharide fraction and partly because the bioavailability of the lipophilic alkylamides is preparation-sensitive.
Root vs Aerial Parts — Why It Matters
Different plant parts within the same Echinacea species contain different constituent ratios:
- Root — higher in alkylamides (especially for E. angustifolia), higher in echinacoside, lower in cichoric acid, lower in high-MW polysaccharides
- Aerial parts (leaves, stems, flowers) — higher in cichoric acid (especially for E. purpurea), higher in high-MW polysaccharides, lower in alkylamides
The traditional Eclectic-physician use was E. angustifolia root tincture, on the principle that the root contained the most concentrated medicinal activity. Modern German and European herbal medicine has largely shifted to E. purpurea aerial-parts pressed juice, driven by the Echinaforce trial evidence and by cultivation practicality (the aerial parts can be harvested annually without destroying the plant; the root harvest kills the plant and requires 3-4 years of growth).
For a patient buying Echinacea today, the practical implication is to read the label carefully. A product labeled simply "Echinacea" without species or plant-part specification is essentially uncharacterized. The trial-supported preparations are: (1) Echinaforce E. purpurea aerial-parts pressed juice (the strongest single piece of evidence), and (2) E. angustifolia root alcoholic tincture used in the traditional Eclectic style. Products falling outside those two categories may still be effective but lack direct trial validation.
Prophylaxis vs At-Onset Treatment
Echinacea trials fall into two categories that differ substantially in design and outcome:
- Prophylaxis trials — participants take Echinacea continuously through cold season (typically 2-4 months) and the primary outcome is the incidence or total days of cold symptoms. The Echinaforce Jawad 2012 trial is the prototypical example. These trials generally show modest reductions in cold incidence and total cold-symptom days.
- At-onset treatment trials — participants start Echinacea at first cold symptoms (sneezing, sore throat) and continue for 7-10 days, with the primary outcome being symptom severity score or duration of illness. Results have been more mixed — some trials show modest reductions in severity and duration, others show no significant difference from placebo.
The mechanistic explanation for the prophylaxis-vs-onset difference is that the alkylamide-mediated CB2 modulation, the caffeic-acid-mediated antioxidant and antiviral effects, and the polysaccharide-mediated immune priming all need time to reach steady state in tissues. Starting Echinacea at symptom onset of a cold — when viral replication is already underway — gives less time for the modulatory effects to develop than continuous prophylactic dosing.
The implication for patients is that the most evidence-supported use is continuous prophylaxis through cold season at the Echinaforce dose, rather than starting at first sniffle. The at-onset approach is not without evidence but the effect size is more modest and less consistent across trials.
The Negative Trials (Turner 2005, Barrett 2010)
Two widely-publicized trials reported negative results and deserve direct discussion because they are frequently cited as evidence that Echinacea "doesn't work":
- Turner 2005 (NEJM) — Ronald Turner and colleagues at the University of Virginia inoculated 437 healthy adults intranasally with rhinovirus 39 after pretreatment with one of three Echinacea preparations or placebo. None of the three Echinacea preparations significantly reduced cold rates or severity. The trial used three different E. angustifolia root extracts at relatively low daily doses (1.5 g/day of dried herb equivalent). Critics noted that the dose was low and the preparation was root-only rather than the Echinaforce aerial-parts pressed juice that has the strongest trial evidence, and that experimental rhinovirus inoculation in a lab is a different clinical scenario from natural cold acquisition in community settings.
- Barrett 2010 (Annals of Internal Medicine) — Bruce Barrett and colleagues at the University of Wisconsin enrolled 719 adults with new-onset cold symptoms and randomized them to 10.2 g of unrefined E. purpurea root and aerial parts on the first day, then 5.1 g/day for four more days, vs placebo, vs no-pill control. Cold severity score was 33% lower in the Echinacea arm than placebo, but the difference did not reach the prespecified statistical significance threshold. Cold duration was nominally shorter in the Echinacea arm (7.0 days vs 7.6 days) but again not significantly so. The trial is sometimes labeled "negative," but the point estimates favor Echinacea; the trial simply did not reach the high bar of statistical significance.
Neither trial fundamentally contradicts the positive evidence from Echinaforce-style trials. The Turner trial used a preparation (low-dose E. angustifolia root) that differs from the trial-validated preparations. The Barrett trial used an at-onset treatment design where, as discussed above, the effect is smaller and less consistent than in prophylactic designs. The overall body of evidence, properly stratified by preparation and design, supports a modest benefit for trial-validated preparations used prophylactically — a conclusion consistent with the Karsch-Volk Cochrane review's measured language.
Influenza — What the Evidence Does and Doesn't Show
The clinical evidence for Echinacea specifically for influenza (as distinct from the more general "common cold") is sparser but generally favorable. The trials and observational data suggest:
- In-vitro antiviral activity against multiple influenza A strains, including H1N1 and H5N1, has been demonstrated for Echinaforce extract. The mechanism appears to be inhibition of viral binding to host cells via interference with hemagglutinin, plus antioxidant effects that reduce host-tissue damage from the inflammatory response.
- The Pleschka 2009 study in Virology Journal showed Echinaforce extract had antiviral activity comparable to oseltamivir (Tamiflu) in cell culture against several influenza strains.
- A 2015 trial by Raus and colleagues in Current Therapeutic Research compared Echinaforce with oseltamivir for early-stage acute influenza in 473 adults. Recovery times were not significantly different between the two arms, suggesting Echinaforce may be a reasonable adjunctive therapy for early influenza.
The caveat is that none of these data are nearly as strong as the conventional antiviral evidence for neuraminidase inhibitors (oseltamivir, zanamivir, baloxavir) in early influenza, and Echinacea should not be considered a replacement for those drugs in patients with severe influenza or high-risk groups (elderly, immunocompromised, pregnant). For mild influenza in otherwise healthy adults, Echinacea is a reasonable supportive option with a benign safety profile. See our Influenza page for more on conventional and integrative approaches.
Practical Patient Protocol
For an adult patient considering Echinacea for cold and flu prevention during cold season:
- Choose a trial-validated preparation — Echinaforce (A. Vogel) E. purpurea aerial-parts pressed-juice tincture is the most evidence-based choice. Acceptable alternatives include high-quality E. angustifolia root alcoholic tincture from a reputable herbalist (Herb Pharm, Gaia Herbs, Mountain Rose Herbs) or a combination E. purpurea aerial + root tincture from the same manufacturers.
- Dose for prophylaxis — for Echinaforce, the trial dose is 0.9 mL three times daily continuously through cold season (approximately 2.4 mL/day total). For a 1:5 alcoholic root tincture, the traditional Eclectic dose is approximately 2-4 mL three times daily. Most trials run continuously for 2-4 months during peak cold season.
- Dose for at-onset treatment — double the prophylactic dose at first cold symptoms, continued for 7-10 days or until symptoms resolve. Slightly less evidence-supported than prophylaxis but still reasonable.
- Avoid generic encapsulated dried herb — the alkylamides degrade in dried herb stored at room temperature, and the polysaccharide fraction is poorly bioavailable in dry capsules without the alcoholic-extract matrix. Liquid tinctures and pressed juices outperform dried encapsulated products in trials.
- Cycle if desired — some traditional herbalists recommend cycling Echinacea (3 weeks on, 1 week off) to prevent receptor desensitization, though there is no specific trial evidence for this practice. Continuous 4-month dosing in the Echinaforce trial did not show any safety signal or efficacy attenuation.
- Stack with proven adjuncts — Vitamin D3 repletion (most U.S. adults are deficient in winter), zinc lozenges at symptom onset, and adequate sleep are all separately evidence-supported and synergistic.
The expected benefit on average is modest — roughly a 20-30% reduction in cold incidence and roughly a 1-2 day reduction in cold duration. This is not a miracle drug, but it is a meaningful improvement on placebo with an excellent safety profile, and the cost (under $30 for a season's supply of Echinaforce or a comparable tincture) is low.
Key Research Papers
- Karsch-Volk M, Barrett B, Kiefer D, Bauer R, Ardjomand-Woelkart K, Linde K (2014). Echinacea for preventing and treating the common cold. Cochrane Database of Systematic Reviews, Issue 2: CD000530. — PubMed
- Shah SA, Sander S, White CM, Rinaldi M, Coleman CI (2007). Evaluation of echinacea for the prevention and treatment of the common cold: a meta-analysis. The Lancet Infectious Diseases 7(7):473-480. — PubMed
- Jawad M, Schoop R, Suter A, Klein P, Eccles R (2012). Safety and efficacy profile of Echinacea purpurea to prevent common cold episodes: a randomized, double-blind, placebo-controlled trial. Evidence-Based Complementary and Alternative Medicine 2012:841315. — PubMed
- Turner RB, Bauer R, Woelkart K, Hulsey TC, Gangemi JD (2005). An evaluation of Echinacea angustifolia in experimental rhinovirus infections. New England Journal of Medicine 353(4):341-348. — PubMed
- Barrett B, Brown R, Rakel D, Mundt M, Bone K, Barlow S, Ewers T (2010). Echinacea for treating the common cold: a randomized trial. Annals of Internal Medicine 153(12):769-777. — PubMed
- Pleschka S, Stein M, Schoop R, Hudson JB (2009). Anti-viral properties and mode of action of standardized Echinacea purpurea extract against highly pathogenic avian influenza virus (H5N1, H7N7) and swine-origin H1N1 (S-OIV). Virology Journal 6:197. — PubMed
- Raus K, Pleschka S, Klein P, Schoop R, Fisher P (2015). Effect of an Echinacea-based hot drink versus oseltamivir in influenza treatment: a randomized, double-blind, double-dummy, multicenter, noninferiority clinical trial. Current Therapeutic Research 77:66-72. — PubMed
- Schoop R, Klein P, Suter A, Johnston SL (2006). Echinacea in the prevention of induced rhinovirus colds: a meta-analysis. Clinical Therapeutics 28(2):174-183. — PubMed
- Goel V, Lovlin R, Barton R, Lyon MR, Bauer R, Lee TD, Basu TK (2004). Efficacy of a standardized echinacea preparation (Echinilin) for the treatment of the common cold: a randomized, double-blind, placebo-controlled trial. Journal of Clinical Pharmacy and Therapeutics 29(1):75-83. — PubMed
- Lindenmuth GF, Lindenmuth EB (2000). The efficacy of echinacea compound herbal tea preparation on the severity and duration of upper respiratory and flu symptoms: a randomized, double-blind placebo-controlled study. Journal of Alternative and Complementary Medicine 6(4):327-334. — PubMed
- Sperber SJ, Shah LP, Gilbert RD, Ritchey TW, Monto AS (2004). Echinacea purpurea for prevention of experimental rhinovirus colds. Clinical Infectious Diseases 38(10):1367-1371. — PubMed
- Ross SM (2016). Echinacea purpurea: a proprietary extract of Echinacea purpurea is shown to be safe and effective in the prevention of the common cold. Holistic Nursing Practice 30(1):54-57. — PubMed
PubMed Topic Searches
- PubMed: Echinacea common cold prevention
- PubMed: Echinaforce pressed juice trials
- PubMed: Echinacea influenza antiviral
- PubMed: Echinacea angustifolia root tincture
- PubMed: Echinacea URI meta-analyses
Connections
- Echinacea Overview
- Echinacea Benefits Hub
- Echinacea Immune Modulation
- Echinacea Antimicrobial & Wound Healing
- Echinacea Safety & Autoimmune Cautions
- Elderberry
- Andrographis
- Goldenseal
- Vitamin C
- Vitamin D3
- Zinc
- Immune Boosting
- Influenza
- Sinusitis
- All Herbs