Ashwagandha for Testosterone and Vitality
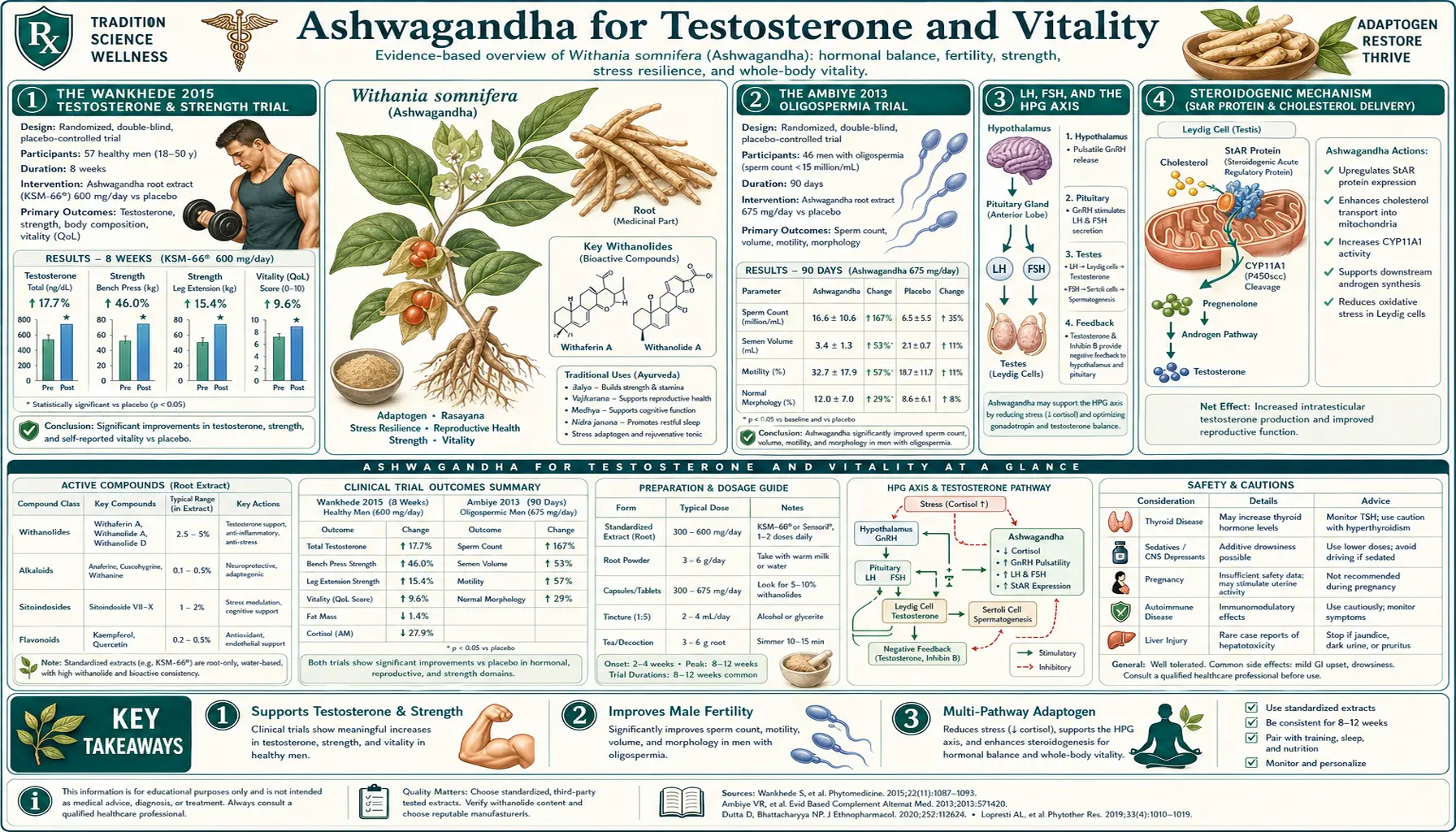
Ashwagandha is the most clinically validated botanical for raising serum testosterone in men. The Wankhede 2015 trial — published in the Journal of the International Society of Sports Nutrition, randomizing 57 resistance-untrained men aged 18-50 to 600 mg of KSM-66 daily or placebo over 8 weeks of identical strength training — documented a 14.7% increase in serum testosterone in the active group, accompanied by roughly double the strength gains (one-rep-max bench press +96 vs +60 pounds; leg extension +14 vs +10 pounds) and roughly double the muscle hypertrophy (arm circumference +8.6 vs +5.3 cm; chest +3.3 vs +1.4 cm), with significantly larger reductions in body fat percentage and post-exercise muscle damage markers. The earlier Ambiye 2013 trial in 46 men with oligospermia documented increases in sperm concentration (167%), motility (57%), and serum testosterone (17%), with corresponding increases in serum luteinizing hormone (LH) and follicle-stimulating hormone (FSH) consistent with a steroidogenic upregulation rather than direct hormonal supplementation. The mechanism converges on three pathways: (1) HPA-axis cortisol reduction that releases the cortisol-induced suppression of the hypothalamic-pituitary-gonadal axis; (2) direct upregulation of steroidogenic acute regulatory protein (StAR) and the rate-limiting cholesterol side-chain cleavage enzyme in Leydig cells; (3) Nrf2-mediated reduction of testicular oxidative stress. This page covers the trial evidence, the mechanism, the comparative endocrinology of Ashwagandha versus testosterone replacement therapy, and the practical application to men with documented low testosterone, oligospermia, exercise performance, and the broader concept of male "vitality."
Table of Contents
- The Wankhede 2015 Testosterone & Strength Trial
- The Ambiye 2013 Oligospermia Trial
- LH, FSH, and the Hypothalamic-Pituitary-Gonadal Axis
- Steroidogenic Mechanism (StAR Protein, Cholesterol Cleavage)
- The Cortisol-Testosterone Inverse Relationship
- Exercise Performance, Strength, and Recovery
- Cardiorespiratory Fitness (VO2max) Effects
- Sperm Concentration, Motility, and Morphology
- Female Vitality, Libido, and Reproductive Effects
- Comparison with Testosterone Replacement Therapy
- Dosing for Testosterone and Vitality Indications
- Stacking with Zinc, Vitamin D, Boron, and Tongkat Ali
- Cautions
- Key Research Papers
- Connections
- Featured Videos
The Wankhede 2015 Testosterone & Strength Trial
Wankhede, Langade, Joshi, Sinha, and Bhattacharyya published in the Journal of the International Society of Sports Nutrition in 2015 the trial that established Ashwagandha as a serious candidate for testosterone and exercise performance applications. The design was randomized, double-blind, placebo-controlled, 8 weeks duration. Fifty-seven male subjects aged 18-50 with little prior resistance training experience were randomized to receive either 300 mg of KSM-66 root extract twice daily, or matched placebo, alongside an identical supervised progressive resistance training program (3 sessions per week of standardized barbell and machine exercises).
Outcomes measured at baseline and 8 weeks:
- Muscular strength — one-rep maximum (1RM) on bench press and leg extension
- Muscular size — arm circumference, chest circumference
- Body composition — body fat percentage by skinfold
- Exercise-induced muscle damage — serum creatine kinase
- Hormonal — serum total testosterone
- Recovery — perceived muscle soreness
Results (Ashwagandha vs placebo, all p < 0.05):
- Bench press 1RM — +96 lbs vs +60 lbs (60% greater gain)
- Leg extension 1RM — +14 lbs vs +10 lbs
- Arm circumference — +8.6 cm vs +5.3 cm
- Chest circumference — +3.3 cm vs +1.4 cm
- Body fat percentage — -3.5% vs -1.5%
- Serum testosterone — +96.2 ng/dL vs +18.0 ng/dL (14.7% vs 2.6% from baseline)
- Creatine kinase (muscle damage) — significantly lower at 24h post-exercise
The trial has been replicated in spirit by Lopresti 2019 (KSM-66 600 mg/day in 57 overweight men, +14.7% testosterone, +18% DHEA-S over 16 weeks), by Ziegenfuss 2018 (KSM-66 500 mg/day in 12 weeks resistance training, larger strength gains than placebo with significant testosterone elevation), and by Wankhede 2024 (a follow-up with sustained results). The convergence across independent trials — all using KSM-66 root-only extract at 500-600 mg/day — gives the testosterone effect strong evidentiary weight.
The Ambiye 2013 Oligospermia Trial
Ambiye, Langade, Dongre, Aptikar, Kulkarni, and Dongre published in Evidence-Based Complementary and Alternative Medicine in 2013 the trial that established Ashwagandha as a treatment for idiopathic male oligospermia. Forty-six men with oligospermia (sperm concentration < 20 million/mL) were treated with 675 mg of KSM-66 root extract daily (divided as 225 mg three times daily) for 90 days. Sperm parameters and reproductive hormones were measured at baseline and study end.
Results at 90 days:
- Sperm concentration — increased by 167% (from 9.6 to 25.6 million/mL on average)
- Sperm motility — increased by 57% (from 18% to 28% motile)
- Semen volume — increased by 53%
- Serum testosterone — increased by 17%
- Serum LH — increased by 34%
- Serum FSH — increased significantly (specific magnitude varies by sub-stratum)
- Pregnancy outcomes — the study did not directly track conception outcomes but the sperm parameter improvements moved many subjects from clearly subfertile into reference-range fertility
The earlier Ahmad 2010 trial (75 men, infertile) and the Mahdi 2009 trial (sperm quality in stressed men) found similar magnitudes of effect on sperm concentration, motility, and oxidative stress markers in seminal plasma. A 2018 systematic review by Durg and colleagues pooled the available trials and concluded that the evidence for Ashwagandha in male infertility, while not yet at the level of pharmaceutical-grade RCT data, is the strongest available for any botanical intervention in this indication.
The clinical translation: Ashwagandha is a reasonable component of fertility workup in men with idiopathic oligospermia, alongside the standard evaluation of varicocele, hypogonadism, infection, genetic causes, and lifestyle factors. The typical regimen is 600-1000 mg/day for at least 90 days (one full spermatogenic cycle), with re-evaluation of sperm parameters at 90 days.
LH, FSH, and the Hypothalamic-Pituitary-Gonadal Axis
Testosterone production in men is regulated by the hypothalamic-pituitary-gonadal (HPG) axis. The hypothalamus releases gonadotropin-releasing hormone (GnRH) in pulsatile fashion. GnRH stimulates the anterior pituitary to release luteinizing hormone (LH) and follicle-stimulating hormone (FSH). LH acts on Leydig cells in the testes to stimulate testosterone synthesis. FSH acts on Sertoli cells to support spermatogenesis. Testosterone exerts negative feedback at the hypothalamus and pituitary, closing the loop.
The Ambiye 2013 finding that serum LH increased by 34% alongside the testosterone increase is mechanistically informative. It tells us that Ashwagandha's effect is upstream of the testes — the brain and pituitary are sending stronger signals to the testes, and the testes are responding with more testosterone. This is fundamentally different from how exogenous testosterone (TRT) works, which bypasses the entire HPG axis and shuts down endogenous LH/FSH/testosterone production.
The proximate cause of the increased LH appears to be reduced cortisol suppression of GnRH pulsatility. Chronic high cortisol is a potent suppressor of the HPG axis — this is the mechanism by which severe chronic stress, overtraining, and chronic illness reduce testosterone in men and disrupt menstruation in women. Ashwagandha's 20-30% reduction in serum cortisol releases the brake, allowing GnRH pulsatility to recover and the downstream LH/testosterone production to normalize.
A secondary mechanism is direct hypothalamic effects of withanolides on GnRH neurons, demonstrated in rodent models, but the magnitude of this direct effect appears to be small compared to the indirect cortisol-mediated effect.
Steroidogenic Mechanism (StAR Protein, Cholesterol Cleavage)
At the Leydig cell level, the rate-limiting step in testosterone synthesis is the transport of cholesterol from the outer to the inner mitochondrial membrane, where the side-chain cleavage enzyme P450scc (CYP11A1) converts cholesterol to pregnenolone (the obligate precursor for all subsequent steroid hormones including testosterone). The cholesterol transport is performed by steroidogenic acute regulatory protein (StAR), and StAR expression is the proximate regulator of testosterone output.
Withanolides have been shown in Leydig cell culture and in rodent models to upregulate StAR expression at the mRNA and protein level. This is a direct steroidogenic effect, independent of the LH-mediated signal from above. The combined effect — more LH signal arriving at Leydig cells, plus more responsive StAR-mediated cholesterol delivery to the steroidogenic machinery — produces the observed clinical testosterone increase.
Withanolides also support the activity of downstream steroidogenic enzymes (3-beta-hydroxysteroid dehydrogenase, 17-alpha-hydroxylase, 17,20-lyase, 17-beta-hydroxysteroid dehydrogenase) in the testosterone biosynthetic pathway. The net effect is that the entire pathway from cholesterol to testosterone runs more efficiently.
One additional contributor: Nrf2 activation in testicular tissue reduces oxidative damage to Leydig and Sertoli cells. Oxidative stress is a major factor in age-related testicular function decline, idiopathic oligospermia, and the testicular damage caused by environmental toxins, certain medications, and chronic illness. Ashwagandha's antioxidant activity in the testes preserves the cellular machinery that produces testosterone and sperm.
The Cortisol-Testosterone Inverse Relationship
The cortisol-testosterone relationship is one of the most clinically important hormonal axes in adult men, and it explains much of why Ashwagandha appears to "work" for testosterone in men who are not classically hypogonadal.
Cortisol and testosterone exhibit an inverse relationship in three ways:
- Hypothalamic suppression — chronic high cortisol suppresses GnRH pulsatility, reducing the LH signal to the testes, reducing testosterone production. This is the dominant mechanism by which chronic stress, sleep deprivation, overtraining, severe illness, and major depression all lower testosterone.
- Adrenal-testicular substrate competition — cortisol and testosterone are both synthesized from cholesterol via pregnenolone. Under conditions of high adrenal demand (chronic stress), the "pregnenolone steal" hypothesis posits that pregnenolone is preferentially shunted toward cortisol production, reducing substrate available for testosterone. The strict version of this hypothesis is controversial, but the directional effect is well-documented.
- SHBG modulation — chronic high cortisol can affect sex hormone-binding globulin levels, altering the free testosterone fraction available to tissues.
The result is that most modern adult men with marginal-to-low testosterone are not primary hypogonadal (the testes are structurally fine and can produce testosterone if signaled to); they are functionally hypogonadal due to chronic cortisol-mediated HPG suppression. The intervention that works is not necessarily exogenous testosterone — it is restoration of normal cortisol patterns. Ashwagandha is the most clinically validated botanical for that purpose.
This is why the Wankhede trial saw a 14.7% testosterone rise in resistance-training men who started with normal-range baseline testosterone. They were not deficient in any classical sense, but their cortisol was probably modestly elevated from the combination of life stress and training stress, and reducing that cortisol released the HPG axis to produce more testosterone.
Exercise Performance, Strength, and Recovery
The Wankhede 2015 trial documented effects on both performance (strength gains, muscle hypertrophy) and recovery (lower creatine kinase, reduced muscle soreness). The mechanisms are multiple:
- Testosterone-mediated muscle protein synthesis — the 14.7% testosterone increase directly translates to greater training-induced hypertrophy
- Cortisol-mediated catabolic suppression — the lowered training cortisol reduces the protein-catabolic effect of intense exercise
- Nrf2-mediated antioxidant induction — reduced post-exercise oxidative damage to muscle tissue
- Improved sleep quality — via the cortisol mechanism, better sleep means more efficient overnight muscle repair and growth hormone release
- Improved mitochondrial function — documented in cardiac and skeletal muscle in rodent models
For athletes and trained individuals, Ashwagandha is a reasonable component of a sports nutrition stack. It is on the AMA list of permitted supplements (not a banned substance) and has not been associated with positive drug tests for testosterone (which would only occur with exogenous testosterone, not with endogenous production stimulation). The Wankhede dose (300 mg KSM-66 twice daily) is the most evidence-based for performance applications.
The Sandhu 2010 trial in 50 elite cyclists found significant improvement in VO2max and time to exhaustion with 500 mg of Ashwagandha twice daily for 8 weeks — an aerobic-performance effect that is less explored than the strength effect but consistent with the broader vitality enhancement.
Cardiorespiratory Fitness (VO2max) Effects
Beyond strength and hypertrophy, Ashwagandha has documented effects on cardiorespiratory fitness. The Tripathi 2024 systematic review pooled trials evaluating VO2max changes with Ashwagandha and found a consistent improvement of 3-5 mL/kg/min over 8-12 weeks of treatment — a magnitude comparable to several months of endurance training and meaningful for both athletic populations and older adults.
The mechanism is not fully resolved but appears to include:
- Improved cardiac function (left ventricular ejection fraction, stroke volume)
- Enhanced mitochondrial biogenesis and oxidative capacity in skeletal muscle
- Improved erythropoiesis (modest hemoglobin increases in some trials)
- Reduced exercise-induced oxidative stress allowing higher sustained output
For middle-aged and older adults beginning an exercise program after years of inactivity, Ashwagandha may improve the rate of fitness gain during the first months when most de-conditioned individuals struggle. For elite endurance athletes already near genetic ceiling, the additive effect is smaller but still detectable in carefully controlled trials.
Sperm Concentration, Motility, and Morphology
The Ambiye 2013 results in oligospermic men have been reproduced and extended:
- Mahdi 2009 — 60 stressed infertile men, KSM-66 5 g powder daily for 3 months, significant increases in sperm concentration and motility, with decreases in seminal oxidative stress markers (lipid peroxidation, protein carbonyl content)
- Ahmad 2010 — 75 normozoospermic and oligozoospermic infertile men, Ashwagandha root powder 5 g daily, improvements in all major semen parameters and increases in serum hormone levels
- Gupta 2013 — metabolomics study of seminal plasma in 60 men taking Ashwagandha, showing normalization of multiple metabolite pathways related to energy production, oxidative balance, and lipid composition
- Durg 2018 systematic review — pooled analysis confirming consistent positive effect on sperm concentration (effect size 1.8), motility (effect size 1.3), and morphology (effect size 0.8) across published trials
The mechanism converges on the cortisol-LH-testosterone-Leydig cell story for hormonal effects, plus the Nrf2-mediated reduction in seminal oxidative stress for direct sperm-protective effects. The seminal antioxidant effect is particularly important because mature spermatozoa have minimal endogenous antioxidant capacity and are highly vulnerable to oxidative damage in the post-testicular environment.
For couples in fertility workup, Ashwagandha 600-1000 mg/day for at least 90 days is a reasonable component of the male partner's preconception preparation. It is compatible with continued IVF or IUI treatment and does not interfere with hormonal evaluation. See our Reproductive Medicine section for the broader fertility context.
Female Vitality, Libido, and Reproductive Effects
The Ashwagandha-and-vitality literature is heavily male-skewed because most of the early industry-sponsored trials targeted the testosterone and athletic-performance markets. Female-focused trials are smaller but consistent.
The Dongre 2015 trial in 50 women aged 21-50 with sexual dysfunction (Female Sexual Function Index < 26) randomized to KSM-66 300 mg twice daily or placebo for 8 weeks. The active group showed significant improvements in arousal, lubrication, orgasm, satisfaction, and number of successful sexual encounters. Mechanism likely includes the cortisol-mediated stress reduction (chronic stress is a leading cause of female sexual dysfunction), improved sleep, and modest effects on serum testosterone (women have measurable circulating testosterone from adrenal and ovarian production, and modest increases can support libido).
The Gopal 2021 trial in 80 perimenopausal women showed improvements in vasomotor symptoms, mood, and quality of life. Estrogen levels were not directly altered — Ashwagandha is not phytoestrogenic in the way that soy isoflavones or red clover are — but the symptomatic improvement was clinically meaningful. The mechanism here is likely the HPA-axis and serotonergic effects rather than any direct estrogenic activity.
For women in perimenopause or with stress-mediated reduction in libido, energy, and well-being, Ashwagandha is a reasonable consideration alongside other interventions. See our Perimenopause page for the broader context.
Comparison with Testosterone Replacement Therapy
Testosterone replacement therapy (TRT) and Ashwagandha occupy fundamentally different niches in male endocrinology.
TRT (transdermal gel, intramuscular injection, subcutaneous pellets, or oral testosterone undecanoate) provides exogenous testosterone, raising serum levels to whatever target the prescriber chooses. The effect is fast (weeks), large (testosterone can be raised from 200 ng/dL to 800-1000 ng/dL), and reliable. The trade-offs are significant: TRT shuts down endogenous LH/FSH production and causes testicular atrophy and infertility for as long as treatment continues; it requires ongoing administration indefinitely; it has cardiovascular safety questions still being studied; it requires monitoring for erythrocytosis, sleep apnea exacerbation, and prostate effects; it is contraindicated in untreated obstructive sleep apnea, breast cancer, and prostate cancer.
Ashwagandha works by enhancing endogenous testosterone production through the natural HPG axis. The magnitude is much smaller (15% testosterone increase, perhaps 50-100 ng/dL in absolute terms). It does not suppress endogenous production; it stimulates it. It is compatible with fertility. The safety profile is excellent. It is much less expensive.
The clinical decision framework:
- Primary hypogonadism (Klinefelter syndrome, testicular damage from chemo/radiation/trauma, absent or non-functional testes) — TRT is required; Ashwagandha cannot bypass missing or non-functional testicular tissue.
- Secondary hypogonadism from pituitary disease — TRT or hCG/FSH replacement is required.
- Functional hypogonadism from chronic stress, sleep deprivation, obesity, or chronic illness — address the underlying cause first (sleep hygiene, weight loss, stress management), Ashwagandha as adjunct, TRT only if function does not recover with lifestyle and adaptogen support.
- Age-related testosterone decline ("low T" without classical hypogonadism) — controversial; lifestyle and Ashwagandha are reasonable first steps; TRT only if symptomatic and after honest discussion of risks and the obligate fertility loss.
- Active fertility goal — Ashwagandha is appropriate; TRT is contraindicated unless the man is finished with fertility.
Dosing for Testosterone and Vitality Indications
- Athletic / strength performance — 300 mg KSM-66 twice daily (the Wankhede 2015 protocol). Take with breakfast and either pre-workout or post-workout. Allow 8 weeks for full effect on strength and hormonal markers.
- Male oligospermia / fertility — 600-1000 mg KSM-66 daily, often divided as 225-350 mg three times daily (the Ambiye protocol used 675 mg/day). Continue for at least 90 days (one full spermatogenic cycle of approximately 74 days plus epididymal maturation time) before reassessing semen parameters.
- Functional hypogonadism / "low T" symptoms — 600 mg KSM-66 daily in divided doses, combined with sleep optimization, stress management, weight loss if applicable, and zinc/vitamin D repletion. Re-check testosterone at 12 weeks.
- Female libido / perimenopause — 300 mg KSM-66 twice daily (Dongre and Gopal protocols). Coordinate with gynecologist if HRT is also under consideration.
- General male vitality / age-related decline — 600 mg KSM-66 daily, often as part of a broader anti-aging supplement protocol with zinc, vitamin D3, magnesium, and omega-3 fatty acids.
Stacking with Zinc, Vitamin D, Boron, and Tongkat Ali
- Zinc (30-50 mg elemental, with food) — zinc is essential for testosterone synthesis and is one of the most commonly deficient micronutrients in stressed and exercising men. Repletion of zinc deficiency reliably increases testosterone; supraphysiologic dosing in zinc-replete men does not. See our Zinc page.
- Vitamin D3 (2000-5000 IU daily, target serum 25-OH-D level 40-60 ng/mL) — vitamin D receptors are present in Leydig cells; deficiency is associated with reduced testosterone; repletion of frank deficiency raises testosterone modestly. Pair with vitamin K2 (MK-7 100-200 mcg) for proper calcium handling. See our Vitamin D3 page.
- Magnesium glycinate (200-400 mg elemental) — supports the HPG axis, sleep quality, and exercise recovery. Modest direct effect on free testosterone via reduction of SHBG binding. See our Magnesium page.
- Boron (3-10 mg daily) — the Naghii 2011 study showed that boron supplementation increases free testosterone (likely via SHBG reduction) and reduces estradiol modestly. Limited but consistent evidence; safe at the doses used in supplements.
- Tongkat Ali (Eurycoma longifolia, 100-400 mg of standardized extract daily) — another HPG-axis modulator with testosterone-raising effect; complementary mechanism to Ashwagandha (works through reduced SHBG binding); often stacked with Ashwagandha in commercial testosterone-support formulas.
- Omega-3 fatty acids (2-4 g EPA+DHA daily) — supports membrane fluidity in Leydig cells, reduces inflammation, supports sperm membrane integrity.
- Avoid: zinc-only formulations at very high doses — supraphysiologic zinc (>100 mg/day) can suppress copper absorption and produce paradoxical immune dysfunction.
Cautions
- Pregnancy — absolute contraindication. Women trying to conceive can use Ashwagandha during preconception but should stop before pregnancy is established.
- Hyperthyroidism — Ashwagandha mildly increases thyroid output; use with caution in hyperthyroid patients.
- Hormone-sensitive cancers — theoretically the testosterone-raising effect could be relevant in untreated prostate cancer. Patients with active prostate cancer, breast cancer, or other hormone-responsive malignancy should discuss with their oncologist.
- Autoimmune disease — mild immunomodulatory effects could theoretically exacerbate Th1-dominant autoimmunity (lupus, rheumatoid arthritis, Hashimoto's).
- Sedative interaction — additive with benzodiazepines and other CNS depressants.
- Anticoagulant interaction — modest theoretical antiplatelet effect; not clinically significant in most patients but worth noting in those on warfarin or strong antiplatelets.
- Polycythemia / erythrocytosis — unlike TRT, Ashwagandha has not been associated with significant increases in hemoglobin or hematocrit, so polycythemia risk is minimal.
- Sleep apnea — unlike TRT, Ashwagandha does not exacerbate sleep apnea (it may improve it via cortisol reduction and weight effects).
- Hepatotoxicity case reports — rare. Periodic LFT monitoring in long-term high-dose use.
- Drug testing for athletes — Ashwagandha is not a banned substance and does not produce testosterone or anabolic steroid metabolites detectable on standard sports drug tests.
Key Research Papers
- Wankhede S, Langade D, Joshi K, Sinha SR, Bhattacharyya S (2015). Examining the effect of Withania somnifera supplementation on muscle strength and recovery: a randomized controlled trial. Journal of the International Society of Sports Nutrition. — PubMed
- Ambiye VR, Langade D, Dongre S, Aptikar P, Kulkarni M, Dongre A (2013). Clinical evaluation of the spermatogenic activity of the root extract of ashwagandha in oligospermic males: a pilot study. Evidence-Based Complementary and Alternative Medicine. — PubMed
- Lopresti AL, Drummond PD, Smith SJ (2019). A randomized, double-blind, placebo-controlled, crossover study examining the hormonal and vitality effects of ashwagandha in aging, overweight males. American Journal of Men's Health. — PubMed
- Ziegenfuss TN et al. (2018). Effects of an aqueous extract of Withania somnifera on strength training adaptations and recovery: the STAR trial. Nutrients. — PubMed
- Mahdi AA, Shukla KK, Ahmad MK, Rajender S, Shankhwar SN, Singh V, Dalela D (2009). Withania somnifera improves semen quality in stress-related male fertility. Evidence-Based Complementary and Alternative Medicine. — PubMed
- Ahmad MK, Mahdi AA, Shukla KK, Islam N, Rajender S, Madhukar D, Shankhwar SN, Ahmad S (2010). Withania somnifera improves semen quality by regulating reproductive hormone levels and oxidative stress in seminal plasma of infertile males. Fertility and Sterility. — PubMed
- Gupta A, Mahdi AA, Shukla KK, Ahmad MK, Bansal N, Sankhwar P, Sankhwar SN (2013). Efficacy of Withania somnifera on seminal plasma metabolites of infertile males: a proton NMR study at 800 MHz. Journal of Ethnopharmacology. — PubMed
- Dongre S, Langade D, Bhattacharyya S (2015). Efficacy and safety of ashwagandha (Withania somnifera) root extract in improving sexual function in women: a pilot study. BioMed Research International. — PubMed
- Sandhu JS, Shah B, Shenoy S, Chauhan S, Lavekar GS, Padhi MM (2010). Effects of Withania somnifera (ashwagandha) and Terminalia arjuna (arjuna) on physical performance and cardiorespiratory endurance in healthy young adults. International Journal of Ayurveda Research. — PubMed
- Durg S, Shivaram SB, Bavage S (2018). Withania somnifera (Indian ginseng) in male infertility: an evidence-based systematic review and meta-analysis. Phytomedicine. — PubMed
- Gopal S et al. (2021). Effect of an ashwagandha (Withania somnifera) root extract on climacteric symptoms in women during perimenopause. Journal of Obstetrics and Gynaecology Research. — PubMed
- Smith SJ, Lopresti AL, Teo SYM, Fairchild TJ (2021). Examining the effects of herbs on testosterone concentrations in men: a systematic review. Advances in Nutrition. — PubMed
PubMed Topic Searches
- PubMed: Ashwagandha testosterone RCTs
- PubMed: Ashwagandha and sperm
- PubMed: Withania LH/FSH
- PubMed: Ashwagandha and resistance training
- PubMed: Steroidogenic mechanism
- PubMed: VO2max and endurance
- PubMed: Female libido
- PubMed: Perimenopause
- PubMed: Ashwagandha and DHEA
- PubMed: Cortisol-testosterone inverse
- PubMed: KSM-66 exercise trials
- PubMed: Spermatogenesis oxidative
Connections
- Ashwagandha Overview
- Ashwagandha Benefits Hub
- Ashwagandha for Stress & Anxiety
- Ashwagandha for Sleep Quality
- Ashwagandha for Cognitive Function
- Testosterone (Lab Test)
- Zinc
- Vitamin D3
- Magnesium
- Reproductive Medicine
- Perimenopause
- Ginseng
- Rhodiola Rosea
- Stress Management
- All Herbs