Ashwagandha for Sleep Quality
Ashwagandha is one of the few botanical sleep aids supported by polysomnography and validated self-report instruments rather than just by subjective testimonial. The pivotal trial — Langade 2021, an 8-week randomized double-blind placebo-controlled study in 80 subjects (40 with diagnosed insomnia, 40 healthy volunteers) — documented that 300 mg of root extract twice daily reduced sleep onset latency by 28%, improved total sleep time, reduced wake-after-sleep-onset, and improved the Pittsburgh Sleep Quality Index (PSQI). The mechanism is the most unusual story in botanical pharmacology: triethylene glycol, a small water-soluble molecule isolated from Ashwagandha leaves, crosses the blood-brain barrier and induces sleep by acting at the GABA-A receptor in mouse models. Combined with the cortisol-lowering effect of root withanolides on the HPA axis, the result is a botanical that addresses both sleep onset (acute GABAergic facilitation) and sleep maintenance (lowered nocturnal cortisol). This page walks through the trial evidence, the triethylene glycol discovery, the mechanism, and the practical comparison with melatonin, magnesium glycinate, valerian, and L-theanine.
Table of Contents
- The Langade 2021 PSQI Trial
- Triethylene Glycol — The Unusual Sleep-Active Molecule
- Cortisol Reduction and Sleep Architecture
- Effect in Diagnosed Insomnia vs Healthy Sleepers
- Sleep Onset Latency, Total Sleep Time, and Efficiency
- Comparison with Melatonin
- Comparison with Magnesium Glycinate and L-Theanine
- Comparison with Valerian and Herbal Sedatives
- Dosing and Timing for Sleep Indications
- Cautions for Sleep-Focused Use
- Key Research Papers
- Connections
- Featured Videos
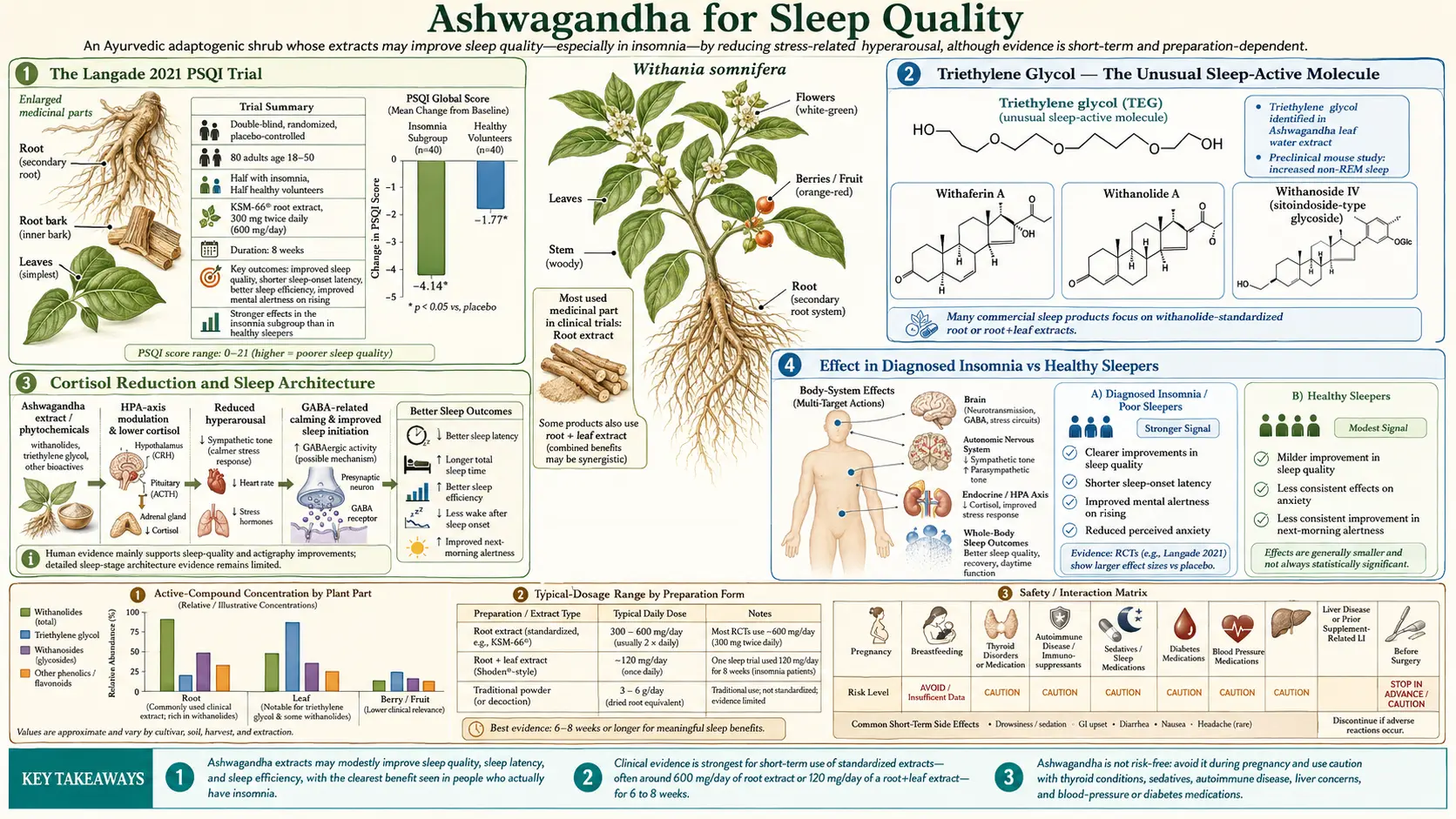
The Langade 2021 PSQI Trial
Langade and colleagues published the most rigorous Ashwagandha-for-insomnia trial in the Journal of Ethnopharmacology in 2021. The design was a double-blind, randomized, parallel-group, placebo-controlled study running for 8 weeks. Eighty subjects were enrolled in two strata: 40 healthy volunteers (PSQI < 5) and 40 patients with diagnosed insomnia (PSQI > 5 and meeting ICSD-3 criteria). Within each stratum, subjects were randomized 1:1 to either 300 mg of KSM-66 root extract twice daily, or matched placebo.
Outcomes were measured at baseline, 6 weeks, and 8 weeks using the Pittsburgh Sleep Quality Index (PSQI — the gold standard self-report instrument with seven component scores: subjective sleep quality, sleep onset latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleep medication, daytime dysfunction). Anxiety and overall mental alertness were tracked as secondary outcomes.
Results at 8 weeks (Ashwagandha vs placebo, insomnia subgroup):
- Sleep onset latency — reduced from approximately 105 minutes at baseline to 75 minutes (28% improvement) vs minimal change in placebo
- Total sleep time — increased from approximately 4.4 hours at baseline to 6.0 hours (37% increase) vs modest improvement in placebo
- Sleep efficiency — increased from 75% to 83%
- PSQI total score — reduced from 12.7 to 6.0 (47% reduction) vs reduction from 13.0 to 11.0 in placebo
- Anxiety (HAM-A) — reduced by 56% vs 17% in placebo
- Mental alertness on rising — improved significantly without daytime grogginess
- Adverse events — mild and indistinguishable from placebo; no withdrawals
In the healthy-volunteer subgroup, improvements were smaller in absolute magnitude (these subjects started with adequate sleep) but statistically significant in onset latency, total sleep time, and PSQI score. This pattern — larger effect in the symptomatic population, smaller-but-real effect in healthy subjects — is characteristic of restorative interventions rather than pure sedatives.
An earlier Langade trial in 2019 in 60 patients with insomnia and anxiety produced similar magnitudes of effect with the same KSM-66 extract over 10 weeks, anchoring the result with a prior independent test.
Triethylene Glycol — The Unusual Sleep-Active Molecule
The most surprising finding in Ashwagandha pharmacology over the past decade was published by Kaushik and colleagues in PLOS ONE in 2017. The team at the National Institute of Advanced Industrial Science and Technology in Japan was investigating which component of Ashwagandha was responsible for the sleep-promoting activity observed in mouse models. They fractionated water extracts of Ashwagandha leaves and tested each fraction for sleep induction using a tryptophan-induced sleep model. The active fraction was unexpectedly small, polar, and water-soluble — not the lipophilic withanolides that had been assumed to drive sleep activity.
Mass spectrometry and NMR identified the active molecule as triethylene glycol — a simple polyethylene glycol (HOCH2CH2OCH2CH2OCH2CH2OH, also known as TEG or 2,2'-ethylenedioxydiethanol). This was a startling result: TEG is a common industrial solvent and humectant, present in liquid laundry detergents, household disinfectants, and as a base for many cosmetic preparations. It would not have appeared on any reasonable list of expected botanical sleep actives.
Yet the Kaushik experiments were rigorous. Synthetic triethylene glycol, administered to mice at doses equivalent to those produced by Ashwagandha leaf extract, replicated the sleep-induction profile of the whole leaf extract. The effect was blocked by flumazenil, the GABA-A benzodiazepine-site antagonist, suggesting that TEG was acting at or near the GABA-A receptor — consistent with how Ashwagandha withanolides had previously been characterized.
The clinical implications are still being worked out. Most commercial Ashwagandha products are root extracts (KSM-66 is root-only), which would contain little or no leaf-derived TEG. Sensoril, as a full-spectrum root-and-leaf extract, contains both withanolides and any TEG present in the leaf material. Traditional Ayurvedic kshirapaka preparations (root powder simmered in milk) would not extract much TEG either. The Langade trials used KSM-66 root extract and produced robust sleep effects without leaf TEG, suggesting that the cortisol-lowering and GABAergic withanolide mechanisms are themselves sufficient for the sleep benefit — TEG may be an additional contribution rather than the primary actor.
Cortisol Reduction and Sleep Architecture
The HPA-axis story explored in the Stress & Anxiety deep dive is half the explanation for the sleep effect. Cortisol follows a strong diurnal rhythm in healthy individuals: peak in the first hour after waking (the "cortisol awakening response"), gradual decline through the day, and a nadir near the start of sleep that supports both initiation of sleep and the deep slow-wave sleep that dominates the first half of the night.
In chronic stress and insomnia, this pattern flattens or inverts. Evening cortisol fails to fall to the normal nadir. Subjects experience a "wired and tired" state at bedtime — physically exhausted but mentally activated. Sleep onset is prolonged. Once asleep, elevated nocturnal cortisol suppresses growth hormone release (which normally peaks during the first slow-wave episode), reduces REM sleep duration, and increases wake-after-sleep-onset (WASO) and early-morning awakening.
Ashwagandha's reduction of morning cortisol is accompanied by restoration of the diurnal pattern, with lower evening cortisol — even when total cortisol output across the 24-hour cycle is only modestly reduced. The Lopresti 2019 trial documented this with detailed salivary cortisol sampling: morning cortisol reduced by approximately 23%, but evening cortisol reduced even more dramatically, and the diurnal slope steepened toward normal.
The downstream effect on sleep architecture is restored slow-wave sleep, longer REM episodes, and improved sleep efficiency — all measurable on polysomnography in subsequent smaller studies that combined Ashwagandha with sleep monitoring. The subjective experience is that sleep "feels deeper" and morning rising is easier.
Effect in Diagnosed Insomnia vs Healthy Sleepers
One of the strengths of the Langade 2021 design was stratifying the analysis into diagnosed insomnia patients and healthy volunteers. The dual analysis answers a clinically important question: is Ashwagandha a sleep aid only for people with insomnia, or does it produce gains in normal sleepers too?
The answer is mostly the former. Insomnia patients showed dramatic improvements — sleep onset latency reduced by approximately 30 minutes, total sleep time increased by approximately 90 minutes, PSQI reduced by half. Healthy sleepers showed smaller absolute gains — sleep onset latency reduced by approximately 9 minutes, total sleep time increased by approximately 25 minutes, PSQI improved by a small but significant amount.
This restorative pattern (large effect on dysfunction, small effect in normal) is what would be expected from a normalizing adaptogen rather than a pharmacologic sedative. A sedative-hypnotic like zolpidem would produce similar dose-dependent sedation regardless of baseline status — it would put both groups to sleep faster, with attendant risks of over-sedation in normal sleepers. Ashwagandha's pattern matches the broader Ayurvedic concept of a rasayana that restores balance rather than imposing a uniform effect.
For clinical practice, this means Ashwagandha is most appropriately recommended for patients with measured sleep disturbance, chronic stress, evening anxiety, or signs of HPA-axis dysregulation. It is not a particularly useful intervention for occasional jet lag in a normal sleeper (melatonin would be a better choice) or for purely behavioral sleep restriction in shift workers (sleep hygiene and chronotherapy take priority).
Sleep Onset Latency, Total Sleep Time, and Efficiency
Three core sleep metrics deserve unpacking because they are the most commonly improved by Ashwagandha:
- Sleep onset latency (SOL) — the time from "lights out" to the first epoch of consensus-scored sleep. Normal SOL is approximately 10-20 minutes. SOL > 30 minutes is considered abnormal; SOL > 60 minutes is severe sleep onset insomnia. Ashwagandha trials consistently show 25-30% reduction in SOL, most dramatic in subjects with baseline SOL > 30 minutes.
- Total sleep time (TST) — the cumulative duration of actual sleep across the time-in-bed window. Normal adult TST is 7-9 hours. TST < 6 hours is associated with adverse cardiovascular and metabolic outcomes. The Langade insomnia subgroup gained approximately 90 minutes of TST over 8 weeks — a clinically substantial improvement that moves average subjects from clear sleep deprivation territory into adequate-sleep range.
- Sleep efficiency — TST as a percentage of total time in bed (TIB). Healthy sleep efficiency is > 85%. Sleep efficiency < 80% is the central diagnostic feature of insomnia — the patient is allocating adequate time to sleep but spending too much of it awake. Ashwagandha-treated subjects in the Langade trial moved from approximately 75% to 83% sleep efficiency — near-normal.
The improvement in sleep efficiency is particularly important because it reduces the most distressing subjective experience of insomnia — lying in bed awake, watching the clock, anticipating tomorrow's exhaustion. Reducing wake-after-sleep-onset and reducing the late-night anxiety cycle that develops around chronic insomnia are often more clinically meaningful than the headline total-sleep-time number.
Comparison with Melatonin
Melatonin and Ashwagandha occupy different niches in the sleep-supplement landscape. They are often combined, not competing.
Melatonin (0.3 to 5 mg, 30-60 minutes before bedtime) is fundamentally a circadian-rhythm shift agent — it is the hormone the pineal gland releases when darkness falls, signaling night to the suprachiasmatic nucleus and downstream sleep circuits. It is most effective for delayed sleep phase disorder, jet lag, shift work disorder, and for older adults whose endogenous melatonin production has declined. It is less effective as a pure sleep aid in chronic insomnia in otherwise healthy adults, because the deficit there is not melatonin signaling but cortisol dysregulation and behavioral conditioning.
Ashwagandha works through cortisol reduction and GABAergic anxiolysis, not through circadian phase shift. It is most effective for chronic stress-induced insomnia, anxiety-driven sleep onset difficulty, and sleep maintenance problems associated with elevated nocturnal cortisol. It is less useful for purely circadian disorders like jet lag.
The two combine cleanly:
- Melatonin 0.5-1 mg at 9 pm to entrain the circadian signal
- Ashwagandha 300 mg root extract with dinner and 300 mg one hour before bed for cortisol/anxiety
- Optional magnesium glycinate at bedtime for additional GABAergic support
This three-component stack is a common starting point in integrative sleep medicine for patients with chronic insomnia who want to avoid prescription hypnotics. It is generally safe, non-habit-forming, and effective in the 60-70% range over 6-8 weeks of consistent use.
Comparison with Magnesium Glycinate and L-Theanine
Magnesium glycinate (200-400 mg elemental magnesium at bedtime) and L-theanine (200 mg, 1-3 times daily including bedtime) are the other two commonly stacked nutritional sleep supports.
Magnesium glycinate provides two simultaneous interventions. First, magnesium is an NMDA receptor antagonist (blocking glutamate-mediated neural excitation) and a positive modulator at GABA-A. Second, the glycine moiety is itself a primary inhibitory neurotransmitter in the brainstem and spinal cord. Most stressed adults are mildly magnesium-deficient. Replacing the deficit with the well-tolerated glycinate form improves sleep onset and sleep quality in the meta-analyses, particularly in older adults and stressed populations. Magnesium glycinate complements Ashwagandha well — they work through different mechanisms.
L-theanine increases alpha-wave EEG activity (the "relaxed but alert" pattern), increases brain GABA and glycine, and modulates dopamine and serotonin in ways that produce subjective calming. It does not directly sedate. Its strength is in reducing the racing thoughts and ruminative anxiety that often delay sleep onset. L-theanine and Ashwagandha can be combined safely — they act through different molecular targets.
The decision tree for sleep stacking:
- Sleep onset difficulty with racing thoughts — L-theanine first; add Ashwagandha if persistent
- Sleep onset difficulty with general anxiety and elevated cortisol — Ashwagandha first
- Sleep maintenance difficulty (wake at 3 am, can't return to sleep) — cortisol pattern is dysregulated; Ashwagandha most likely to help
- Delayed sleep phase (can't fall asleep until 2 am, would sleep until 10 am if allowed) — melatonin first
- Restless sleep with muscle tension or cramping — magnesium glycinate first
Comparison with Valerian and Herbal Sedatives
Valerian, passionflower, lemon balm, and hops are the classical Western herbal sedatives, all acting primarily through GABA-A facilitation. Valerian root extract at 300-600 mg before bedtime has modest efficacy in some trials and no benefit in others; meta-analyses suggest a small effect on subjective sleep quality with high heterogeneity.
Compared to valerian, Ashwagandha:
- Has stronger evidence base (multiple positive RCTs vs mixed results for valerian)
- Addresses cortisol pathology in addition to GABA
- Lacks the distinctive odor that makes valerian capsules unpleasant for many users
- Does not produce the "hangover" feeling some users report with valerian
- Has documented daytime use without sedation (valerian is purely bedtime)
For purely situational acute insomnia (one-night sleep difficulty before a big event), a fast-acting herbal sedative like passionflower or lemon balm at bedtime may work better than Ashwagandha, which takes weeks to build its full effect. For chronic insomnia and stress-related sleep disturbance, Ashwagandha is the better-evidenced and more durable choice.
Dosing and Timing for Sleep Indications
The Langade trial used KSM-66 root extract at 300 mg twice daily, taken with breakfast and dinner. This dosing pattern produces continuous coverage and avoids the trap of expecting a single bedtime dose to act like a hypnotic.
Practical sleep-focused dosing options:
- Standard — 300 mg KSM-66 with dinner, 300 mg one hour before bedtime. Take with food (the withanolides are fat-soluble; absorption improves with a small fat-containing meal or a teaspoon of nut butter).
- Sensoril for evening focus — 125-250 mg Sensoril one hour before bedtime, often combined with magnesium glycinate. The higher withanolide concentration and leaf TEG content may produce a stronger acute GABA effect than KSM-66.
- Traditional kshirapaka — 3-5 grams of root powder simmered in 1 cup whole milk with a pinch of cardamom and a teaspoon of ghee, consumed one hour before bedtime. Pleasant taste, decent withanolide extraction, the calming ritual itself contributes to sleep readiness.
- Stacked sleep formula — 300 mg KSM-66 + 200 mg L-theanine + 200 mg magnesium glycinate + 0.5 mg melatonin, all one hour before bed. Four mechanisms (cortisol/GABA, alpha-wave/glycine, NMDA antagonism, circadian phase). Often more effective than any single component for chronic refractory insomnia.
Allow 4-8 weeks for full sleep effect. The acute GABAergic component may produce mild perceptible calming from the first dose, but the durable architecture improvements emerge as cortisol patterns remodel.
Cautions for Sleep-Focused Use
- Pregnancy — absolute contraindication. Use other sleep aids in pregnancy (magnesium glycinate is generally accepted as safe; melatonin is controversial but used; benzodiazepines and Z-drugs are contraindicated).
- Driving and machinery the next morning — Ashwagandha generally does not produce daytime sedation, but a small subset of users report mild morning grogginess on initial days of use. Start on a weekend or low-demand period.
- Sedative interaction — additive with benzodiazepines, opioids, alcohol, and prescription hypnotics. Patients tapering off prescription hypnotics commonly use Ashwagandha as part of the transition; co-administration during the taper is reasonable, but the full taper should still be supervised.
- Sleep apnea — Ashwagandha is not a treatment for obstructive sleep apnea. Anyone with loud snoring, witnessed apneas, or daytime hypersomnolence should be evaluated for OSA before assuming Ashwagandha will resolve the sleep complaint. Adding any GABAergic agent to untreated severe OSA can worsen nocturnal hypoxemia.
- Hyperthyroidism — Ashwagandha mildly increases thyroid output, which can worsen insomnia in hyperthyroid patients. Patients with insomnia caused by hyperthyroidism should avoid Ashwagandha.
- Restless legs syndrome / periodic limb movement disorder — Ashwagandha does not directly help; iron status, dopamine agonists, and other targeted treatments take priority.
- Insomnia secondary to depression — if the insomnia is the somatic feature of major depression, the depression should be treated. Ashwagandha may be a reasonable adjunct (it has weak antidepressant signal in some trials) but is not a standalone treatment for depression-related insomnia.
See our Insomnia page for the broader evaluation and management framework, and our Sleep Hygiene page for the foundational behavioral interventions that should accompany any pharmacologic or supplement strategy.
Key Research Papers
- Langade D, Thakare V, Kanchi S, Kelgane S (2021). Clinical evaluation of the pharmacological impact of ashwagandha root extract on sleep in healthy volunteers and insomnia patients: a double-blind, randomized, parallel-group, placebo-controlled study. Journal of Ethnopharmacology. — PubMed
- Langade D, Kanchi S, Salve J, Debnath K, Ambegaokar D (2019). Efficacy and safety of ashwagandha (Withania somnifera) root extract in insomnia and anxiety: a double-blind, randomized, placebo-controlled study. Cureus. — PubMed
- Kaushik MK, Kaul SC, Wadhwa R, Yanagisawa M, Urade Y (2017). Triethylene glycol, an active component of Ashwagandha (Withania somnifera) leaves, is responsible for sleep induction. PLOS ONE. — PubMed
- Deshpande A, Irani N, Balkrishnan R, Benny IR (2020). A randomized, double blind, placebo controlled study to evaluate the effects of ashwagandha (Withania somnifera) extract on sleep quality in healthy adults. Sleep Medicine. — PubMed
- Cheah KL, Norhayati MN, Husniati Yaacob L, Abdul Rahman R (2021). Effect of ashwagandha (Withania somnifera) extract on sleep: a systematic review and meta-analysis. PLOS ONE. — PubMed
- Lopresti AL, Smith SJ, Malvi H, Kodgule R (2019). An investigation into the stress-relieving and pharmacological actions of an ashwagandha extract. Medicine (Baltimore). — PubMed
- Salve J, Pate S, Debnath K, Langade D (2019). Adaptogenic and anxiolytic effects of ashwagandha root extract. Cureus. — PubMed
- Kelgane SB, Salve J, Sampara P, Debnath K (2020). Efficacy and tolerability of ashwagandha root extract in the elderly for improvement of general well-being and sleep: a prospective, randomized, double-blind, placebo-controlled study. Cureus. — PubMed
- Speers AB, Cabey KA, Soumyanath A, Wright KM (2021). Effects of Withania somnifera on stress and stress-related neuropsychiatric disorders anxiety, depression, and insomnia. Current Neuropharmacology. — PubMed
- Verma N, Gupta SK, Tiwari S, Mishra AK (2021). Safety of ashwagandha root extract: a randomized, placebo-controlled, study in healthy volunteers. Complementary Therapies in Medicine. — PubMed
- Mehta AK, Binkley P, Gandhi SS, Ticku MK (1991). Pharmacological effects of Withania somnifera root extract on GABA-A receptor complex. Indian Journal of Medical Research. — PubMed
- Pandey A, Bani S, Sangwan PL, Koul A, Bhagat A, Khajuria RK (2018). Multifunctional neuroprotective effect of withanone, a compound from Withania somnifera roots. Cytokine. — PubMed
PubMed Topic Searches
- PubMed: Ashwagandha sleep RCTs
- PubMed: Withania sleep latency
- PubMed: TEG and sleep
- PubMed: Ashwagandha PSQI
- PubMed: Evening cortisol
- PubMed: Ashwagandha in the elderly
- PubMed: Sleep architecture
- PubMed: Ashwagandha sleep meta-analysis
- PubMed: Melatonin vs ashwagandha
- PubMed: KSM-66 sleep trials
- PubMed: Adaptogen sleep effects
- PubMed: GABA-A mechanism
Connections
- Ashwagandha Overview
- Ashwagandha Benefits Hub
- Ashwagandha for Stress & Anxiety
- Ashwagandha for Cognitive Function
- Ashwagandha for Testosterone
- Insomnia
- Anxiety
- Sleep Hygiene
- Stress Management
- Lemon Balm
- Holy Basil (Tulsi)
- Magnesium
- Glycine
- Bacopa Monnieri
- All Herbs