Pork for Thiamine (B1) Density
Pork is the single richest dietary source of thiamine (vitamin B1) per gram in the human food supply — roughly 8 times the thiamine concentration of beef, chicken, or lamb. A 3-oz (85 g) serving of pork loin delivers about 0.7 mg of thiamine, more than half the adult RDA. The mechanism is rooted in pig metabolism: pig skeletal muscle relies more heavily on glycolytic pathways and pyruvate dehydrogenase flux than ruminant muscle, and thiamine pyrophosphate (TPP) is the obligate cofactor at that metabolic junction. This page walks through the chemistry, the historical context of beriberi in polished-rice cultures, why traditional Asian and Eastern European cuisines pair pork with carbohydrate-heavy staples, and the modern populations — alcoholics, bariatric patients, diabetics on chronic metformin — for whom thiamine status is clinically relevant.
Table of Contents
- Thiamine Chemistry and the TPP Cofactor
- Why Pork Concentrates Thiamine So Heavily
- Serving-Size Data Across Cuts
- Beriberi History and Polished-Rice Cultures
- Cooking Losses (Boiling, Frying, Roasting)
- Alcohol and Thiamine Deficiency (Wernicke-Korsakoff)
- Diabetes, Metformin, and Subclinical Thiamine Deficiency
- Bariatric Surgery and Thiamine Loss
- Food Thiamine vs. Supplements
- Key Research Papers
- Connections
- Featured Videos
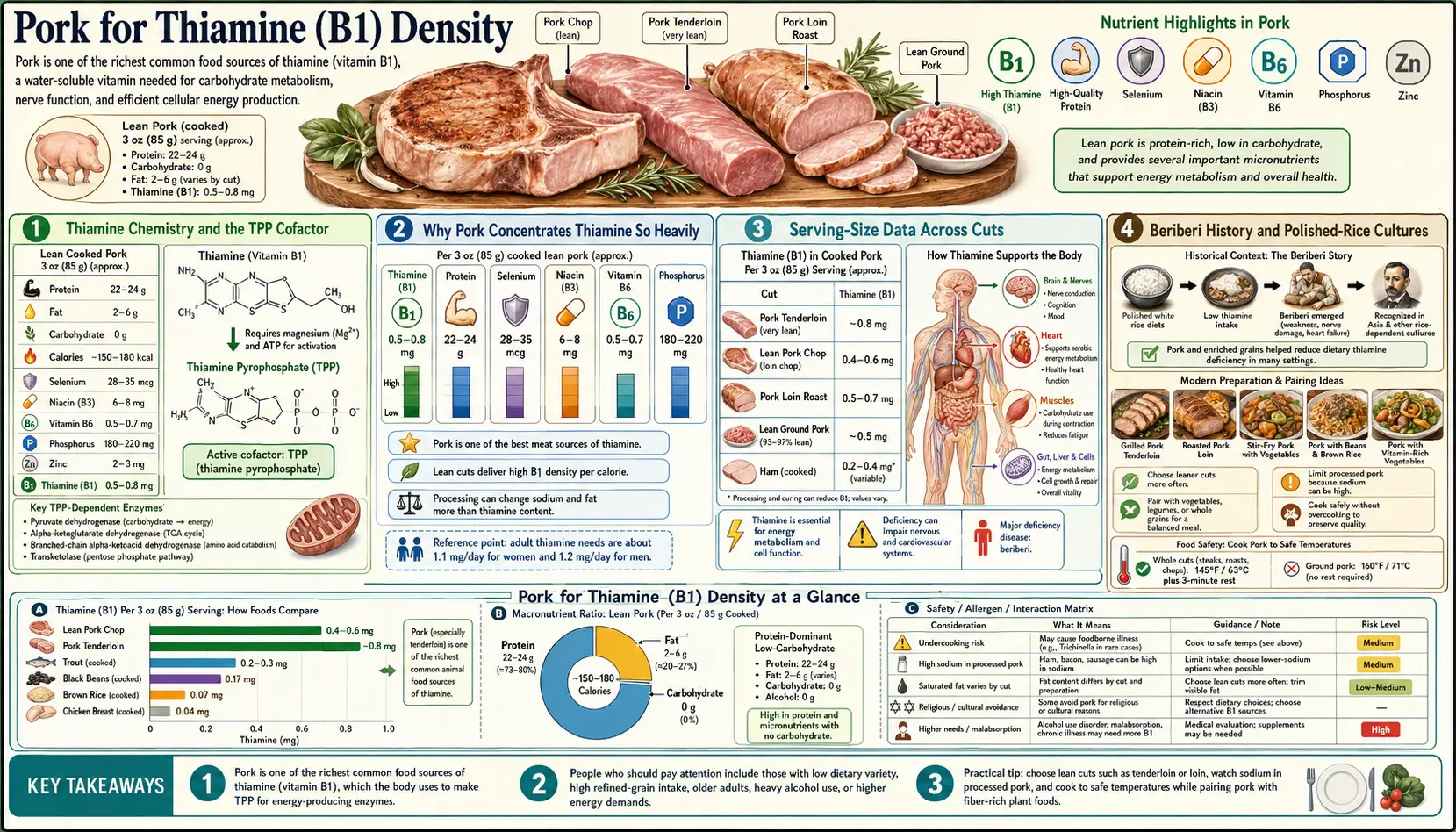
Thiamine Chemistry and the TPP Cofactor
Thiamine (vitamin B1) is a small water-soluble molecule composed of a pyrimidine ring linked by a methylene bridge to a thiazole ring with a hydroxyethyl side chain. Once inside cells, it is rapidly phosphorylated by thiamine pyrophosphokinase to form thiamine pyrophosphate (TPP), the biologically active cofactor.
TPP is the essential cofactor for several enzymes operating at critical metabolic junctions:
- Pyruvate dehydrogenase complex (PDH) — converts pyruvate (the end product of glycolysis) to acetyl-CoA, the entry molecule for the Krebs cycle. Without TPP, glucose-derived carbon cannot enter mitochondrial oxidative metabolism, and lactate accumulates instead.
- Alpha-ketoglutarate dehydrogenase — a rate-limiting enzyme within the Krebs cycle itself.
- Branched-chain alpha-keto acid dehydrogenase (BCKAD) — catabolizes the branched-chain amino acids leucine, isoleucine, and valine.
- Transketolase — an enzyme of the pentose phosphate pathway, generating ribose-5-phosphate for nucleotide synthesis and NADPH for antioxidant defense.
The clinical consequence of thiamine deficiency is that high-flux glycolytic tissues (heart muscle, brain, peripheral nerves) cannot complete the transition from glycolysis to oxidative phosphorylation. Lactic acid accumulates. ATP production drops. The clinical manifestations — cardiac failure (wet beriberi), peripheral neuropathy (dry beriberi), and brain dysfunction (Wernicke encephalopathy) — all trace back to this single metabolic block.
The half-life of thiamine in human tissue is short (10-20 days) and the body stores only 25-30 mg total. A diet completely devoid of thiamine produces measurable clinical signs in 2-3 weeks. There is no slow chronic depletion buffer comparable to the year-long liver storage of vitamin B12 or the months-long storage of vitamin A.
Why Pork Concentrates Thiamine So Heavily
The dramatic concentration of thiamine in pork muscle (compared to beef, chicken, or lamb) is not coincidence. Pig skeletal muscle has a distinctive metabolic profile:
- Higher proportion of type IIB (fast glycolytic) fibers compared to grazing ruminants whose muscle is dominated by slower oxidative fibers
- Greater reliance on glycolytic metabolism for ATP production during muscle activity
- Correspondingly higher TPP requirement at the pyruvate dehydrogenase step
- Higher steady-state intracellular thiamine concentration to support that enzyme activity
The pig essentially constructs and stores thiamine in its muscle tissue as part of normal physiology, not as an emergency reserve. When humans eat pork, they recover that biological investment as dietary thiamine.
The other notable feature of pork thiamine is its chemical form. In raw and cooked pork, most thiamine is present as free thiamine and as thiamine pyrophosphate (TPP) — both of which are well absorbed after gastric and intestinal hydrolysis to free thiamine. There is no significant antinutrient binding factor in pork to interfere with absorption, in contrast to certain raw fish and shellfish that contain heat-labile thiaminases capable of destroying ingested thiamine.
Serving-Size Data Across Cuts
USDA FoodData Central thiamine values for common pork cuts, per 3-oz (85 g) cooked serving:
- Pork loin (roasted) — ~0.72 mg thiamine (60% RDA)
- Pork tenderloin — ~0.81 mg thiamine (68% RDA)
- Pork chop (boneless, broiled) — ~0.65 mg thiamine (54% RDA)
- Pork shoulder (pulled, roasted) — ~0.55 mg thiamine (46% RDA)
- Ham (lean, cured) — ~0.45 mg thiamine (38% RDA)
- Bacon (pan-fried, 3 slices) — ~0.10 mg thiamine (8% RDA)
- Ground pork (cooked) — ~0.57 mg thiamine (48% RDA)
For comparison (3-oz cooked):
- Beef sirloin — ~0.10 mg thiamine (8% RDA)
- Chicken breast — ~0.06 mg thiamine (5% RDA)
- Lamb chop — ~0.07 mg thiamine (6% RDA)
- Salmon — ~0.30 mg thiamine (25% RDA)
The pork-beef gap of approximately 7-8x reflects the species-specific muscle metabolism described above. Salmon is the only other commonly eaten animal protein with meaningful thiamine content, but still trails pork by more than half.
A single serving of pork tenderloin or loin gets an adult most of the way to the RDA of thiamine in one meal. Cured ham and bacon are lower because of curing and processing losses, but still substantially above beef and chicken.
Beriberi History and Polished-Rice Cultures
The historical context for thiamine deficiency is the introduction of industrial rice polishing in 19th-century Asia. White polished rice removes the thiamine-rich bran and germ, leaving only the starchy endosperm. In cultures where polished rice became the dominant calorie source and other thiamine sources (pork, organ meats, legumes, whole grains) were limited, beriberi became epidemic.
Christiaan Eijkman, working at a military hospital in Java in the 1890s, noticed that chickens fed leftover polished rice from the prison kitchen developed paralytic neuropathy, while chickens fed brown rice did not. Eijkman's observation eventually led to the isolation of thiamine by Casimir Funk in 1912 — the first “vital amine” (hence “vitamine,” later shortened to vitamin).
The cultures that retained thiamine-adequate diets despite eating polished rice did so by pairing rice meals with thiamine-rich animal foods. Cantonese cuisine uses pork in nearly every meal — char siu, pork dumplings, wonton soup, pork-and-rice clay pot dishes, lap cheong sausage with rice. Filipino cuisine centers on lechon (roasted whole pig), longanisa sausage, sisig, and adobo — almost always with rice. Vietnamese cuisine uses pork as the dominant protein in pho, bun thit nuong, banh mi, and countless rice dishes. Korean cuisine features samgyeopsal (pork belly) and bossam alongside rice and kimchi.
The biochemical logic is elegant: high-carbohydrate meals require thiamine to convert glucose-derived pyruvate to acetyl-CoA. Pairing carbohydrate-heavy rice with thiamine-rich pork delivers both substrate and cofactor in the same meal. Cultures that pair polished rice with low-thiamine proteins (chicken, white fish) and few thiamine-rich legumes are at substantially higher risk of marginal deficiency.
Modern beriberi is rare in well-fed populations but persists in pockets: refugee camps with rationed white rice and minimal protein, certain prison populations, and chronic alcoholics worldwide.
Cooking Losses (Boiling, Frying, Roasting)
Thiamine is the most heat-labile and water-leachable of the B vitamins. Cooking method matters substantially:
- Boiling (without consuming the liquid) — up to 40% thiamine loss to the cooking water
- Stewing or braising (consuming the liquid) — only 5-15% loss, since the water-soluble thiamine is recovered in the broth
- Roasting — 15-25% loss
- Frying — 15-30% loss
- Grilling/broiling — 20-30% loss
- Microwaving — 10-20% loss (fast cooking time minimizes degradation)
- Curing (ham, bacon) — nitrite-cured products show further losses; cured ham retains roughly 50-60% of the thiamine of fresh pork loin
Two practical implications: (1) When pork is the principal thiamine source in a meal, use the cooking liquid — soups, stews, and braises preserve far more thiamine than methods that discard the liquid. (2) Sulfites in some cured pork products can accelerate thiamine destruction; this is a minor effect in modern processing but is worth noting.
Even after typical cooking losses, a 3-oz serving of roasted pork loin still delivers about 0.55 mg thiamine — nearly half the adult RDA. No realistic cooking method depletes pork thiamine to the trace levels found in beef or chicken.
Alcohol and Thiamine Deficiency (Wernicke-Korsakoff)
Chronic alcohol use is the single most common cause of thiamine deficiency in developed countries. The mechanism is multifactorial:
- Reduced dietary intake — alcoholics derive a substantial fraction of calories from ethanol, displacing nutritionally dense food
- Reduced intestinal absorption — ethanol directly impairs the active transport mechanism for thiamine in the proximal small intestine
- Reduced hepatic activation — alcoholic liver disease impairs the phosphorylation of thiamine to TPP
- Increased metabolic demand — ethanol metabolism itself increases the metabolic requirement for B vitamins
Wernicke encephalopathy is the acute neurological emergency triad of ophthalmoplegia (eye movement abnormalities), ataxia (gait instability), and confusion. Untreated, mortality is 17% and most survivors progress to permanent Korsakoff syndrome — severe anterograde and retrograde amnesia, confabulation, executive dysfunction.
The standard ER protocol for any altered alcoholic patient is empiric IV thiamine 500 mg three times daily for three days, then maintenance — given before any glucose-containing IV fluid, because giving glucose first can precipitate Wernicke encephalopathy in a thiamine-deficient patient by acutely depleting residual TPP through the suddenly-activated PDH pathway.
For chronic alcoholic patients who continue to drink, oral thiamine 100 mg daily plus a B-complex supplement reduces but does not eliminate risk of progression to Wernicke-Korsakoff. Food sources alone are inadequate when ongoing alcohol use impairs absorption.
Diabetes, Metformin, and Subclinical Thiamine Deficiency
Type 2 diabetic patients have been documented to have lower plasma thiamine concentrations than non-diabetic controls in multiple studies. Two mechanisms contribute:
- Increased urinary loss — hyperglycemia drives osmotic diuresis, accelerating urinary thiamine excretion. Diabetic patients can lose 15-fold more thiamine in urine than non-diabetic controls.
- Metformin and B12 / thiamine absorption — chronic metformin use is well-known to impair vitamin B12 absorption; emerging data suggest a smaller but real effect on thiamine absorption as well.
The clinical relevance is twofold. First, the diabetic complication of peripheral neuropathy — classically attributed entirely to hyperglycemia-driven nerve damage — may have a thiamine-deficiency component in some patients. Benfotiamine, a fat-soluble thiamine derivative with much higher tissue penetration than thiamine HCl, has been studied as adjunctive treatment for diabetic neuropathy with modest but real benefit in several randomized trials.
Second, for diabetic patients eating a typical Western diet (low pork consumption, refined grains), dietary thiamine intake may be marginal at the same time that urinary losses are elevated. Including pork as a regular protein in the diabetic diet — pork tenderloin, pork chops, lean ham — addresses both the macronutrient profile (lean protein) and the thiamine balance.
Bariatric Surgery and Thiamine Loss
Bariatric surgery patients are at high risk of acute thiamine deficiency, particularly after Roux-en-Y gastric bypass and biliopancreatic diversion procedures that bypass the proximal small intestine — the principal site of thiamine absorption.
The most acute risk is in the first 6 months post-operation, when persistent vomiting (a common complication of stomal narrowing or bariatric beriberi) compounds the malabsorption. Cases of Wernicke encephalopathy after bariatric surgery have been reported with normal-appearing nutritional intake on standardized supplement regimens; the deficiency develops faster than supplementation can compensate when absorption is impaired and vomiting is ongoing.
Bariatric protocols typically include 50-100 mg of supplemental thiamine daily indefinitely, parenteral thiamine for any post-operative patient with persistent vomiting, and food-source emphasis on lean pork, fortified grain products, and legumes for ongoing maintenance.
For more on the surgical bypass mechanism and its impact on fat-soluble vitamins, see our Vitamin A Immune Function page, which covers the same malabsorptive pattern for retinol.
Food Thiamine vs. Supplements
For most healthy adults, thiamine needs (RDA: 1.2 mg/day for men, 1.1 mg/day for women) are easily met by food alone, particularly if pork features regularly in the diet. A single 3-oz serving of pork loin plus a slice of whole-grain bread plus a serving of legumes routinely exceeds the RDA.
Thiamine supplements are appropriate in specific contexts:
- Active alcohol use — oral 100 mg daily, despite impaired absorption
- Chronic metformin therapy — consider 50-100 mg daily, especially with concomitant B12 supplementation
- Bariatric surgery patients — per bariatric protocols, indefinitely
- Chronic loop diuretic therapy — furosemide and torsemide can accelerate thiamine urinary loss; consider supplementation in patients on long-term high-dose diuretics for heart failure
- Pregnancy and lactation — modestly increased requirement (1.4 mg/day RDA); standard prenatal vitamins cover this
- Diabetic neuropathy — benfotiamine 150-300 mg twice daily has the best evidence base
Food thiamine and supplemental thiamine HCl are biochemically interchangeable once absorbed; the form does not matter for the underlying biochemistry. Benfotiamine is a special case — its lipophilic structure produces 5-10x higher intracellular concentrations than thiamine HCl, which appears to matter clinically for diabetic neuropathy but not for general thiamine status maintenance.
Key Research Papers
- Lonsdale D (2006). A review of the biochemistry, metabolism and clinical benefits of thiamin(e) and its derivatives. Evidence-Based Complementary and Alternative Medicine. — PubMed
- Sechi G, Serra A (2007). Wernicke's encephalopathy: new clinical settings and recent advances in diagnosis and management. Lancet Neurology. — PubMed
- Thornalley PJ et al. (2007). High prevalence of low plasma thiamine concentration in diabetes linked to a marker of vascular disease. Diabetologia. — PubMed
- Stracciari A et al. (2012). Cognitive functioning after bariatric surgery: Wernicke-Korsakoff syndrome. Obesity Surgery. — PubMed
- Stroh C et al. (2014). Beriberi, a severe complication after metabolic surgery. Obesity Facts. — PubMed
- Stirban A et al. (2006). Benfotiamine prevents macro- and microvascular endothelial dysfunction and oxidative stress following a meal rich in advanced glycation end products in individuals with type 2 diabetes. Diabetes Care. — PubMed
- Manzetti S et al. (2014). Thiamine function, metabolism, uptake, and transport. Biochemistry. — PubMed
- Carpenter KJ (2000). Beriberi, White Rice, and Vitamin B: A Disease, a Cause, and a Cure. University of California Press. — PubMed
- Latt N, Dore G (2014). Thiamine in the treatment of Wernicke encephalopathy in patients with alcohol use disorders. Internal Medicine Journal. — PubMed
- Said HM (2011). Intestinal absorption of water-soluble vitamins in health and disease. Biochemical Journal. — PubMed
- Kerns JC, Arundel C, Chawla LS (2015). Thiamin deficiency in people with obesity. Advances in Nutrition. — PubMed
- Page GLJ et al. (2011). Thiamine deficiency in diabetes mellitus and the impact of thiamine replacement on glucose metabolism and vascular disease. International Journal of Clinical Practice. — PubMed
PubMed Topic Searches
- PubMed: Pork thiamine content
- PubMed: TPP and pyruvate dehydrogenase
- PubMed: Wernicke-Korsakoff syndrome
- PubMed: Benfotiamine diabetic neuropathy
- PubMed: Beriberi and polished rice
Connections
- Pork Overview
- Pork Benefits Hub
- Pork Selenium and Iodine
- Heritage Pork Breeds
- Lard Rendering
- Vitamin B1 (Thiamine)
- Vitamin B12
- Peripheral Neuropathy
- Type 2 Diabetes
- Heart Failure
- All Food
- Beef
- Lentils
- Organ Meats
- Alcohol