Lentils for Soluble Fiber and Cholesterol
In 1990, James Anderson and colleagues at the University of Kentucky published a landmark trial in the American Journal of Clinical Nutrition showing that hypercholesterolemic men eating one cup of beans or oat bran daily for three weeks experienced approximately 19% reductions in total cholesterol and 24% reductions in LDL cholesterol. The Anderson data, replicated across dozens of subsequent trials, established legume soluble fiber as a legitimate, evidence-based dietary intervention for elevated LDL — producing effect sizes that approach the lower end of low-intensity statin therapy without the side-effect profile. A single cup of cooked lentils delivers about 8 grams of soluble fiber, the dose at which the LDL-lowering mechanism (bile-acid sequestration and short-chain fatty acid feedback inhibition of hepatic cholesterol synthesis) measurably engages. This page walks through the mechanism, the major trial data including the 2014 CMAJ meta-analysis by Ha et al. that established a 5% LDL reduction per daily 130 g pulse serving, and the Portfolio Diet framework that stacks lentils with nuts, plant sterols, and viscous fibers for additive effect.
Table of Contents
- Soluble vs Insoluble Fiber: Why the Distinction Matters
- Lentil Fiber Content: 8 g Soluble Per Cup
- Mechanism 1: Bile-Acid Sequestration
- Mechanism 2: SCFA Feedback Inhibition of Cholesterol Synthesis
- The 1990 Anderson Trial and Its Successors
- The 2014 Ha Meta-Analysis: 5% LDL Per Cup
- The Portfolio Diet — Stacking Interventions
- Lentils vs Statins: When Each Is Appropriate
- Secondary Benefits: Blood Pressure and Glycemic Control
- Practical Protocol: One Cup Per Day
- Cautions
- Key Research Papers
- Connections
- Featured Videos
Soluble vs Insoluble Fiber: Why the Distinction Matters
Dietary fiber is the umbrella term for plant-derived carbohydrate that resists digestion by human pancreatic and small-intestinal enzymes. It splits into two functionally distinct subcategories with different physiologic effects:
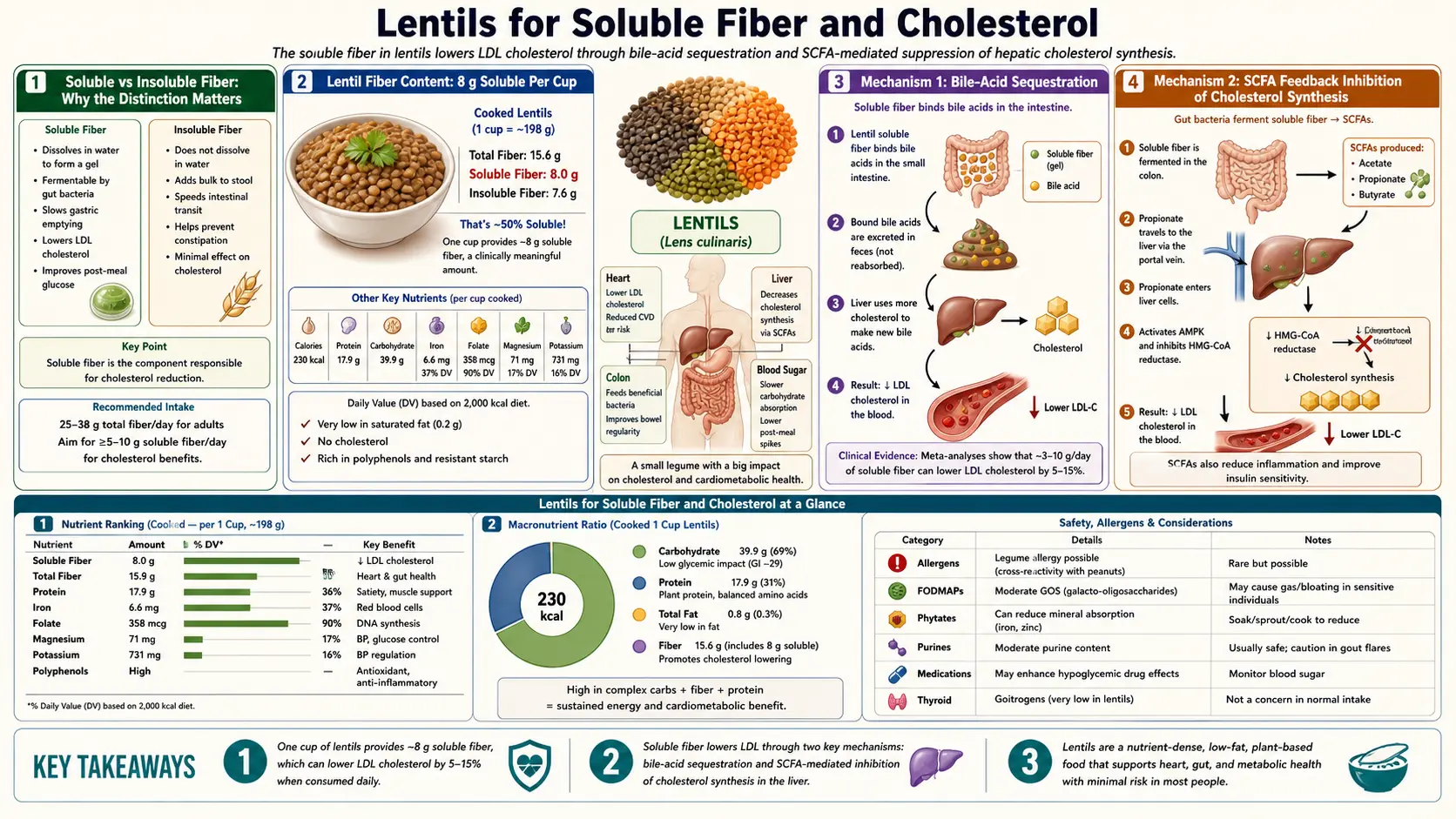
- Soluble fiber dissolves in water to form a viscous gel inside the gut lumen. The viscosity slows gastric emptying, delays glucose absorption (the basis for the low glycemic index of lentils), traps bile acids and dietary cholesterol (the basis for LDL reduction), and provides fermentable substrate for colonic bacteria. Major dietary sources: oat beta-glucan, psyllium husk, legume gum (the major form in lentils, chickpeas, and beans), apple and citrus pectin.
- Insoluble fiber does not dissolve. It acts as bulk-forming, transit-accelerating material that increases stool weight and reduces colonic transit time. It is the dominant fiber type in wheat bran, vegetable cell walls, and the seed coats of grains and legumes. It does not engage the bile-acid sequestration pathway and does not measurably affect LDL cholesterol.
This distinction is why "high-fiber" foods are not all equivalent for cholesterol-lowering. A bowl of Raisin Bran (high in insoluble wheat-bran fiber) does not have the LDL effect of a bowl of oatmeal (high in soluble beta-glucan). Lentils sit toward the soluble-fiber-rich end of the spectrum — roughly half of their 16 g total fiber per cup is soluble, making them comparable to oats and rolled barley on a per-serving basis.
Lentil Fiber Content: 8 g Soluble Per Cup
USDA FoodData Central lists 15.6 g total dietary fiber per 198 g cooked cup of lentils. Detailed compositional studies (Tosh et al. and Quinones et al.) place the soluble fraction at approximately 50% of total fiber, or about 7.5-8 g of soluble fiber per cup. The dominant soluble fibers in lentils are:
- Legume gum / galactomannans — storage polysaccharides in the endosperm of legume seeds, accounting for most of the viscosity-forming behavior
- Pectin — concentrated in the seed coat and cotyledon cell walls
- Beta-glucans — present in smaller quantities than in oats but still meaningful
- Resistant starch (Type 2 and Type 3) — not technically classified as fiber by all definitions but functionally fermentable and behaving similarly to soluble fiber
For comparison, the soluble fiber content per typical serving of common foods:
- Lentils, 1 cup cooked: ~8 g soluble fiber
- Black beans, 1 cup cooked: ~5 g
- Chickpeas, 1 cup cooked: ~5 g
- Oatmeal, 1 cup cooked: ~2 g (beta-glucan)
- Psyllium husk supplement (Metamucil), 1 tbsp: ~4 g
- Apple with skin, 1 medium: ~1 g
- Brussels sprouts, 1 cup cooked: ~2 g
- Avocado, 1 medium: ~2 g
The US Institute of Medicine adequate intake recommendation is 14 g of total fiber per 1,000 kcal consumed — approximately 25 g/day for women and 38 g/day for men. The average American consumes only 15-17 g/day. A single cup of lentils closes about 50% of the average American fiber deficit and supplies roughly the entire daily soluble fiber target.
Mechanism 1: Bile-Acid Sequestration
The liver synthesizes approximately 400-800 mg of new bile acids per day from cholesterol, conjugates them with glycine or taurine, and secretes them via the bile duct into the small intestine where they emulsify dietary fats for absorption. Under normal circumstances, the body recycles bile acids efficiently — approximately 95% are reabsorbed in the terminal ileum and returned to the liver via the portal circulation (the enterohepatic circulation), and only about 5% are lost in feces each day.
Soluble fiber from lentils binds bile acids in the small intestinal lumen and prevents them from being reabsorbed in the ileum. The bile-acid-fiber complex passes into the colon and is excreted. The liver then has to draw down its cholesterol pool to synthesize replacement bile acids — and a substantial fraction of that drawdown comes from LDL particles, which the liver removes from circulation via LDL receptor upregulation. The end result is measurable reductions in plasma LDL cholesterol.
This is the same mechanism used by pharmaceutical bile-acid sequestrants like cholestyramine (Questran), colestipol (Colestid), and colesevelam (Welchol) — first-generation cholesterol-lowering drugs that bind bile acids in the gut. Lentil soluble fiber operates by the identical molecular logic, just at a lower magnitude of effect (drugs are dose-titrated to bind nearly all luminal bile acids; food fiber binds only a fraction).
The downstream effects:
- Hepatic CYP7A1 (cholesterol-7-alpha-hydroxylase, the rate-limiting enzyme for bile acid synthesis) is upregulated
- Hepatic HMG-CoA reductase (the rate-limiting enzyme for cholesterol synthesis, also the statin target) is partially upregulated to replenish cholesterol used for new bile acids
- Hepatic LDL receptor expression increases to capture circulating LDL for cholesterol input
- Plasma LDL cholesterol decreases as a net result
Mechanism 2: SCFA Feedback Inhibition of Cholesterol Synthesis
The second mechanism operates downstream in the colon. Soluble fiber that escapes binding to bile acids passes into the colon where it is fermented by anaerobic bacteria, producing short-chain fatty acids (SCFAs) — primarily acetate, propionate, and butyrate, in a typical ratio of roughly 60:20:20.
Propionate, in particular, is absorbed across the colonic epithelium, enters the portal circulation, and reaches the liver where it inhibits cholesterol synthesis at the HMG-CoA reductase step — the same enzyme targeted by statin drugs. Animal models and some human metabolic studies suggest that hepatic propionate exposure can reduce de novo cholesterol synthesis by 10-30%.
Butyrate, while a less effective cholesterol-synthesis inhibitor, is the dominant energy substrate for colonocytes (the cells lining the colon) and the molecular signal maintaining tight junction integrity in the colonic epithelium. Butyrate signaling through GPR43 and HDAC inhibition has anti-inflammatory effects on the gut-immune axis that may indirectly affect cardiovascular risk through reduced systemic inflammation.
Acetate, the most abundant SCFA produced, is largely used for de novo lipogenesis in adipose tissue and as an energy substrate in muscle, with smaller effects on hepatic lipid metabolism.
The combined effect — bile-acid sequestration plus SCFA-mediated cholesterol synthesis inhibition — produces the dose-dependent LDL reductions seen in legume trials. The two mechanisms are partially independent, which is why combining lentils with oats (different SCFA profile, different bile-acid binding affinity) produces incrementally additive rather than redundant effects.
The 1990 Anderson Trial and Its Successors
James Anderson's 1990 paper in the American Journal of Clinical Nutrition (Hypocholesterolemic effects of oat-bran or bean intake for hypercholesterolemic men) was the landmark demonstration that food-level legume intake produced cholesterol-lowering effects comparable to early-generation drugs. The design:
- 20 hypercholesterolemic men (mean baseline LDL 240 mg/dL)
- Randomized to receive 100 g/day of oat bran (about 1 cup cooked) or 100 g/day of pinto/navy beans (about 1.2 cups cooked) for 21 days
- Wash-in metabolic ward stabilization, then crossover design
- Outcomes: total cholesterol, LDL, HDL, triglycerides at baseline and 21 days
Results: total cholesterol fell by approximately 19% in the bean group and 19% in the oat-bran group. LDL fell by 24% in the bean group and 23% in the oat-bran group. HDL was preserved. Triglycerides did not change significantly. The effect sizes were comparable to early statin trials of the era (lovastatin 20 mg produced approximately 25-30% LDL reduction).
Subsequent trials with lentils specifically (rather than the mixed-bean Anderson protocol) have produced effect sizes typically in the 5-15% LDL reduction range, smaller than the original Anderson numbers because:
- The Anderson population had higher baseline cholesterol (greater reduction potential)
- Modern populations have already incorporated more fiber and unsaturated fat into their backgrounds, leaving less room for additional effect
- Lentils have somewhat lower soluble fiber per gram than pinto beans (about 8 g vs 11 g per cup)
The robust modern estimate from the 2014 Ha meta-analysis in CMAJ is approximately 5% LDL reduction from one daily 130 g serving of pulses (lentils, beans, chickpeas, dry peas) over 6 weeks. This is a clinically meaningful, evidence-grade effect.
The 2014 Ha Meta-Analysis: 5% LDL Per Cup
The Ha et al. 2014 meta-analysis published in the Canadian Medical Association Journal (Effect of dietary pulse intake on established therapeutic lipid targets for cardiovascular risk reduction) pooled 26 randomized controlled trials enrolling 1,037 participants. Key findings:
- Median pulse dose was 130 g/day (about 1 cup cooked)
- Median trial duration was 6 weeks
- Pulse consumption reduced LDL cholesterol by approximately 0.17 mmol/L (6.6 mg/dL), corresponding to about a 5% reduction from baseline LDL of approximately 130 mg/dL
- Effects on HDL and triglycerides were small and not statistically significant
- Effect was consistent across lentils, beans, chickpeas, and dry peas, with no significant heterogeneity by pulse type
The 5% LDL reduction may sound modest, but applied at the population level it corresponds to a meaningful cardiovascular event reduction. The 2010 Cholesterol Treatment Trialists' Collaboration meta-analysis of 26 statin trials established that each 1.0 mmol/L (38.7 mg/dL) reduction in LDL produced approximately a 21% reduction in major vascular events. A 5% LDL reduction from baseline 130 mg/dL corresponds to about 6.5 mg/dL absolute reduction, equating to roughly a 3.5% relative reduction in major vascular events over 5 years — not by itself transformative, but cumulative when stacked with other dietary changes.
The Portfolio Diet — Stacking Interventions
David Jenkins and colleagues at the University of Toronto developed the Portfolio Diet in the early 2000s as a deliberately stacked dietary protocol combining multiple individually-modest LDL-lowering interventions to produce additively large effects. The four pillars:
- Plant sterols / stanols — 2 g/day, from sterol-fortified margarine or supplements. Reduces cholesterol absorption from the gut. Approximately 10% LDL reduction at this dose.
- Soluble fiber — 10 g/day, from oats, barley, psyllium, eggplant, okra, and legumes including lentils. Bile-acid sequestration + SCFA feedback. Approximately 5-7% LDL reduction.
- Soy protein — 50 g/day, from tofu, soy milk, tempeh, or soy meat substitutes. Approximately 5% LDL reduction.
- Nuts — 30 g/day (about a small handful), particularly almonds and walnuts. Provides monounsaturated fats, plant sterols, and arginine. Approximately 5% LDL reduction.
In the pivotal 2003 Jenkins JAMA paper, the Portfolio Diet produced approximately 30% LDL reduction over 4 weeks — comparable to a low-intensity statin (lovastatin 20 mg/day produced 31%). In the longer-term 2011 trial published in JAMA, the Portfolio Diet sustained approximately 13-14% LDL reduction at 6 months even in free-living conditions (versus more aggressive metabolic ward control).
Lentils are an attractive addition to the soluble-fiber pillar because they simultaneously provide the soy protein equivalent for those who don't tolerate soy — in effect collapsing two pillars into one food. A typical "lentil-stacked" Portfolio Diet substitution might be a daily cup of lentil soup or lentil-based dal instead of separate tofu and oatmeal courses.
Lentils vs Statins: When Each Is Appropriate
The comparison is not lentils-versus-statins but rather a question of which combination of interventions makes sense at a given baseline cardiovascular risk:
- Low cardiovascular risk (10-year ASCVD risk <5%) — lifestyle alone is generally sufficient. A daily cup of lentils contributes to a Portfolio-style dietary pattern that addresses LDL without medication. Most reasonable target.
- Borderline risk (5-7.5%) — lifestyle intensification is the first step. A daily lentil serving combined with weight loss, exercise, smoking cessation, and stress management can shift this category back below the lifestyle threshold for many patients.
- Intermediate risk (7.5-20%) — the ACC/AHA guidelines recommend considering statin therapy at this level, with shared decision-making between patient and clinician. Lifestyle including lentils remains foundational; statins add an independent 25-50% LDL reduction on top.
- High risk (>20% 10-year risk, or established ASCVD) — high-intensity statin (atorvastatin 40-80 mg or rosuvastatin 20-40 mg) is the standard of care. Lentils remain part of the dietary backbone but are not a statin substitute at this risk level.
- Familial hypercholesterolemia (FH) — baseline LDL above 190 mg/dL even in young patients — lifestyle including lentils is inadequate. Maximum-intensity statins, ezetimibe, and PCSK9 inhibitors are typically required.
For patients who cannot tolerate statins due to myalgia (3-10% of statin users), the food-based portfolio approach including lentils becomes more important by default. For those who tolerate statins, the dietary and pharmacologic approaches are additive rather than competitive.
Secondary Benefits: Blood Pressure and Glycemic Control
Beyond LDL cholesterol, regular lentil intake produces measurable benefits in two adjacent cardiovascular risk factors:
Blood pressure. The 2014 Jayalath et al. meta-analysis of 8 RCTs (n=554) examining pulse intake and blood pressure found systolic blood pressure reductions of approximately 2.25 mmHg and diastolic reductions of approximately 0.71 mmHg, statistically significant for systolic. The proposed mechanisms: high potassium content (731 mg per cup, more than a banana), magnesium content (71 mg per cup), and fiber-mediated effects on endothelial function. A 2 mmHg systolic reduction is modest individually but at the population level corresponds to about a 6% reduction in stroke mortality and a 4% reduction in coronary heart disease mortality.
Glycemic control. Lentils have a glycemic index of approximately 30 (low; for comparison, white rice is 73, white bread is 75, watermelon is 76). The Jenkins 2012 Archives of Internal Medicine trial randomized 121 type 2 diabetic patients to either a low-glycemic-index diet emphasizing pulses (about 1 cup/day) or a high-cereal-fiber control diet for 3 months. The pulse-rich group achieved HbA1c reduction of approximately 0.5% absolute, comparable to many pharmacologic monotherapies for early diabetes management. The Sievenpiper 2009 Diabetologia meta-analysis of 41 pulse-intake trials confirmed consistent effects on fasting glucose and HbA1c in both diabetic and non-diabetic populations.
The combined lipid, blood pressure, and glycemic effects of regular lentil consumption are why several large observational cohorts (Bazzano 2001 NHANES analysis, Aune 2016 meta-analysis) have documented approximately 11-14% reductions in overall cardiovascular mortality and approximately 22% reduction in coronary heart disease incidence among the highest pulse-consuming quintiles vs the lowest.
Practical Protocol: One Cup Per Day
The dose at which lentils produce measurable cardiovascular benefit is approximately 1 cup cooked daily (or 130 g, equivalent to about 1/2 cup dry weight). Operationally:
- Daily lentil soup — the simplest implementation. Red lentils + onion + carrot + celery + canned tomato + cumin + lemon juice, simmered 25 minutes. One large bowl meets the daily target.
- Daily dal-and-rice or mujadara at one meal — the traditional Indian / Middle Eastern implementations, well-documented for compliance and acceptability.
- Lentil salad at lunch — cooked French green lentils with olive oil, mustard, parsley, and shallot, kept refrigerated for 3-4 days of grab-and-go lunches.
- Sprouted lentil garnish — raw sprouted lentils added to salads, sandwiches, or stir-fries provides higher mineral bioavailability (see Soaking and Phytates) and approximately equivalent fiber to cooked lentils.
- Replace red meat with lentils at 2-3 dinners per week — lentil bolognese, lentil tacos, lentil shepherd's pie. Each substitution adds about 8 g soluble fiber and removes about 3 g saturated fat, compounding the LDL benefit.
Reasonable expectations for response: a 4-8 week trial of daily 1-cup lentil intake should produce 5-10% LDL reduction in a previously lentil-free diet. Track with a fasting lipid panel at baseline and 8 weeks; if no measurable effect emerges, consider whether the intake target is genuinely being met (most non-responders are sub-dose) and whether other dietary components are offsetting the gains (saturated fat from cheese, butter, fatty meat will blunt the response).
Cautions
- Gas and bloating during adaptation — the raffinose and stachyose oligosaccharides in lentils ferment in the colon and produce gas. Start at 1/4 to 1/3 cup daily and increase over 2-4 weeks. The gut microbiome adapts — populations that habitually eat legumes do not experience the same effect. Beano (alpha-galactosidase) can ease the transition.
- Drug interactions — high fiber intake can reduce absorption of certain medications. Notable: levothyroxine, digoxin, certain antibiotics. Separate medication timing from the lentil-containing meal by at least 2 hours.
- Mineral binding (phytates) — at very high legume intakes (multiple cups per day for extended periods) the phytic acid load can measurably reduce zinc, iron, and calcium absorption. Mitigated by soaking and sprouting; see Soaking and Phytates.
- Vitamin K interaction with warfarin — lentils contain modest vitamin K (~3 mcg per cup, low compared to leafy greens at 500+). Sudden large increases in lentil intake are unlikely to destabilize warfarin INR, but consistency is the operative principle — introduce gradually and maintain a stable intake.
- Acute kidney injury / advanced CKD — lentils are moderately high in potassium and phosphorus. Patients with CKD stage 4-5 or hyperkalemia on ACE inhibitors / ARBs / spironolactone should discuss appropriate serving sizes with their nephrologist or renal dietitian.
- Histamine intolerance / mast cell activation syndrome — canned and aged lentil products may contain elevated histamine. Freshly cooked from dry lentils is preferable for histamine-sensitive individuals.
Key Research Papers
- Anderson JW et al. (1990). Hypocholesterolemic effects of oat-bran or bean intake for hypercholesterolemic men. American Journal of Clinical Nutrition, 52(3):495-499. — PubMed
- Ha V et al. (2014). Effect of dietary pulse intake on established therapeutic lipid targets for cardiovascular risk reduction: a systematic review and meta-analysis of randomized controlled trials. CMAJ, 186(8):E252-262. — PubMed
- Bazzano LA et al. (2011). Non-soy legume consumption lowers cholesterol levels: a meta-analysis of randomized controlled trials. Nutrition, Metabolism & Cardiovascular Diseases, 21(2):94-103. — PubMed
- Jenkins DJ et al. (2003). Effects of a dietary portfolio of cholesterol-lowering foods vs lovastatin on serum lipids and C-reactive protein. JAMA, 290(4):502-510. — PubMed
- Jenkins DJ et al. (2011). Effect of a dietary portfolio of cholesterol-lowering foods given at 2 levels of intensity of dietary advice on serum lipids in hyperlipidemia. JAMA, 306(8):831-839. — PubMed
- Brown L et al. (1999). Cholesterol-lowering effects of dietary fiber: a meta-analysis. American Journal of Clinical Nutrition, 69(1):30-42. — PubMed
- Jayalath VH et al. (2014). Effect of dietary pulses on blood pressure: a systematic review and meta-analysis of controlled feeding trials. American Journal of Hypertension, 27(1):56-64. — PubMed
- Sievenpiper JL et al. (2009). Effect of non-oil-seed pulses on glycaemic control: a systematic review and meta-analysis of randomised controlled experimental trials in people with and without diabetes. Diabetologia, 52(8):1479-1495. — PubMed
- Jenkins DJ et al. (2012). Effect of legumes as part of a low glycemic index diet on glycemic control and cardiovascular risk factors in type 2 diabetes. Archives of Internal Medicine, 172(21):1653-1660. — PubMed
- Bazzano LA et al. (2001). Legume consumption and risk of coronary heart disease in US men and women: NHANES I Epidemiologic Follow-up Study. Archives of Internal Medicine, 161(21):2573-2578. — PubMed
- Cholesterol Treatment Trialists' (CTT) Collaboration (2010). Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet, 376(9753):1670-1681. — PubMed
- Hartley L et al. (2016). Dietary fibre for the primary prevention of cardiovascular disease. Cochrane Database of Systematic Reviews. — PubMed
PubMed Topic Searches
- PubMed: Lentil cholesterol clinical trials
- PubMed: Soluble fiber bile acid sequestration
- PubMed: Propionate and cholesterol synthesis
- PubMed: Portfolio Diet (Jenkins)
- PubMed: Pulses and cardiovascular disease
Connections
- Lentils (Main Page)
- Lentils Benefits Hub
- Lentils for Plant Protein and Iron
- Lentils for Folate
- Soaking and Phytates
- Oats (Beta-Glucan)
- Beans
- Chickpeas
- Hypercholesterolemia
- Atherosclerosis
- Hypertension
- Type 2 Diabetes
- Lipid Panel
- Heart Health (Cardiology)
- Magnesium
- Potassium