Lentils for Folate and Pregnancy
One cooked cup of lentils contains 358 micrograms of dietary folate equivalents (DFE) — approximately 90% of the 400 mcg DFE pregnancy RDA in a single serving. This makes lentils the densest natural plant source of folate outside of leafy greens and one of the few foods that can credibly carry a woman of childbearing age to folate sufficiency without fortified breakfast cereal or a synthetic folic acid supplement. The clinical importance was established by the 1991 MRC Vitamin Study, which demonstrated a 72% reduction in neural tube defect recurrence with periconceptional folic acid, and confirmed by Czeizel and Dudas (NEJM 1992) for first-occurrence prevention. The story has gained nuance with the recognition that approximately 10-15% of the population carries the MTHFR C677T homozygous polymorphism, which reduces conversion of synthetic folic acid to active 5-methyltetrahydrofolate — and for those individuals, the natural food folate in lentils (already in the polyglutamate form readily processed to active 5-MTHF) may be preferable to the synthetic fortification form. This page covers the chemistry, the pivotal trials, the MTHFR story, and practical menu strategies for pregnant women, women planning pregnancy, and adults using folate as part of homocysteine and cardiovascular risk management.
Table of Contents
- Folate Numbers: 358 mcg DFE Per Cup
- Folate vs Folic Acid: The Chemistry Distinction
- Folate in One-Carbon Metabolism
- Neural Tube Defects and the MRC Trial
- Periconceptional Timing: Why 4 Weeks Before Pregnancy Matters
- The MTHFR C677T Polymorphism
- 5-MTHF vs Synthetic Folic Acid Supplementation
- U.S. Fortification Policy and Its Effects
- Beyond Pregnancy: Homocysteine, Cardiovascular Disease, Cognition
- Practical Pregnancy Menu Engineering
- Cautions (Including the Folate Trap)
- Key Research Papers
- Connections
- Featured Videos
Folate Numbers: 358 mcg DFE Per Cup
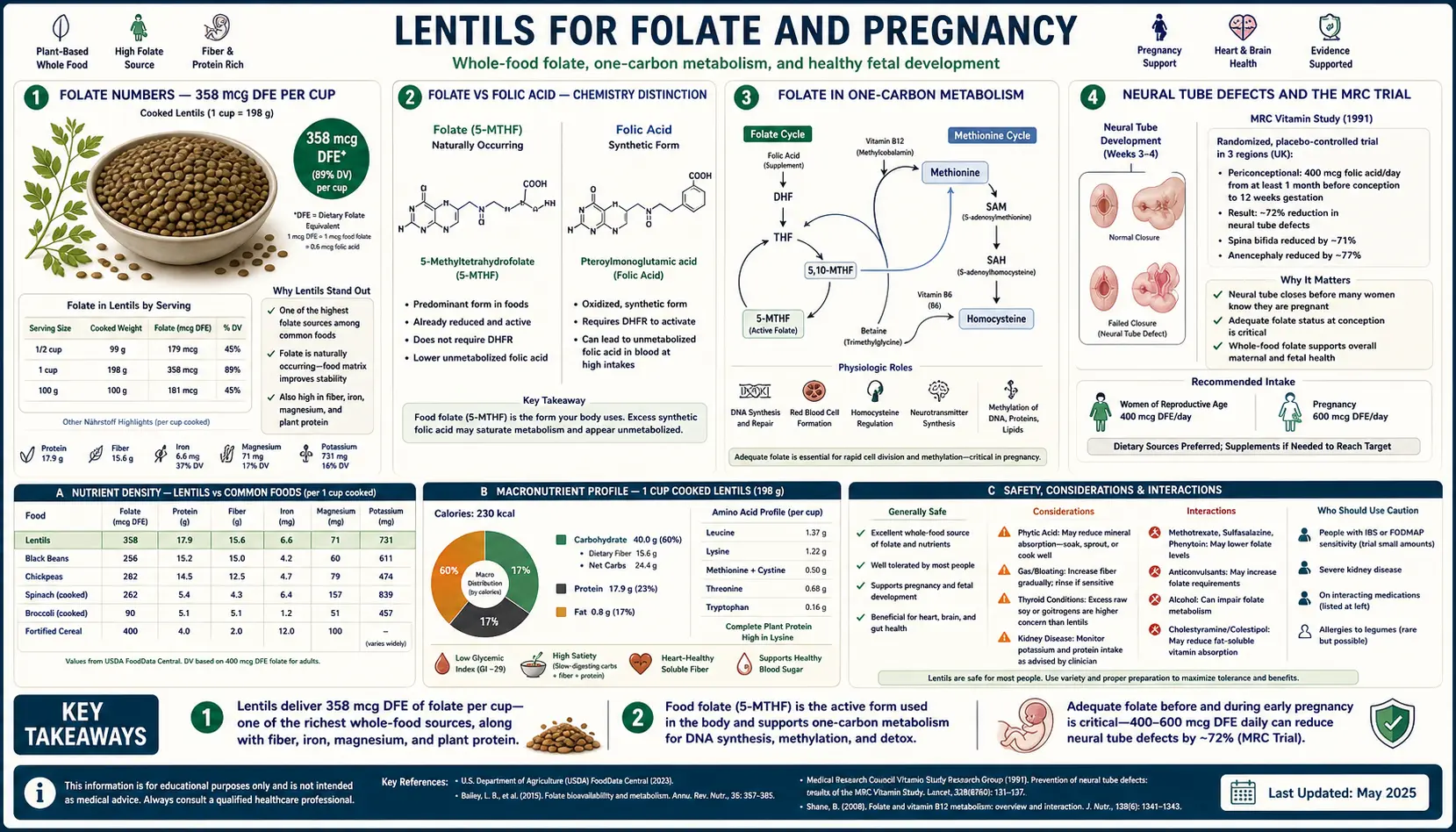
USDA FoodData Central lists 358 mcg of dietary folate equivalents (DFE) per 198 g cooked cup of lentils. The DFE unit accounts for the fact that synthetic folic acid (in supplements and fortified foods) is absorbed about 1.7 times more efficiently than naturally occurring food folate — 100 mcg of folic acid is roughly equivalent to 170 mcg DFE.
The pregnancy RDA is 600 mcg DFE/day; the non-pregnant adult RDA is 400 mcg DFE/day. A single cup of lentils therefore supplies approximately:
- 90% of the non-pregnant adult RDA (358 / 400)
- 60% of the pregnancy RDA (358 / 600)
- 72% of the lactation RDA (358 / 500)
For comparison, the densest natural food folate sources per serving:
- Beef liver, 3 oz cooked: 215 mcg DFE
- Lentils, 1 cup cooked: 358 mcg DFE
- Chickpeas, 1 cup cooked: 282 mcg DFE
- Asparagus, 1 cup cooked: 268 mcg DFE
- Spinach, 1 cup cooked: 263 mcg DFE
- Black beans, 1 cup cooked: 256 mcg DFE
- Broccoli, 1 cup cooked: 84 mcg DFE
- Romaine lettuce, 1 cup raw: 64 mcg DFE
- Orange, 1 medium: 39 mcg DFE
- Egg, 1 large: 22 mcg DFE
Lentils outperform every other commonly-eaten plant food for folate density per serving. They also outperform beef liver, which though slightly less dense per serving carries the practical complication that liver is rarely consumed in the same volume as a bowl of lentil soup.
Folate vs Folic Acid: The Chemistry Distinction
The terms "folate" and "folic acid" are often used interchangeably in popular discourse but they are chemically distinct molecules with different metabolic pathways:
- Folate (vitamin B9) — the umbrella term and the form found in food. Natural food folate exists as polyglutamate-tagged tetrahydrofolate derivatives (typically 5-methyltetrahydrofolate, 5-formyltetrahydrofolate, and 10-formyltetrahydrofolate). The polyglutamate tags must be cleaved by intestinal gamma-glutamyl hydrolase before absorption.
- Folic acid — the fully oxidized, synthetic form added to fortified flour, breakfast cereals, and most supplements. It is not naturally found in food in any meaningful quantity. Folic acid is more stable to heat and oxidation than natural folate, which is why it was chosen for fortification programs.
- 5-Methyltetrahydrofolate (5-MTHF or methylfolate) — the active form that crosses the blood-brain barrier and serves as methyl donor in one-carbon metabolism. All other folate forms must be converted to 5-MTHF before they can be biologically used.
Both folate and folic acid eventually feed into the same 5-MTHF pool, but they take different conversion paths:
- Food folate path — intestinal hydrolysis to monoglutamate, conversion to 5-MTHF in the intestinal mucosa, transport in plasma to tissues. Direct and efficient.
- Folic acid path — absorbed as folic acid, must be reduced first to dihydrofolate (DHF) and then to tetrahydrofolate (THF) by dihydrofolate reductase (DHFR), then methylated to 5-MTHF by 5,10-methylenetetrahydrofolate reductase (MTHFR). The two-step conversion is rate-limited by DHFR activity, which varies several-fold between individuals.
At supplementation doses above approximately 200-400 mcg/day, DHFR can become saturated, and unmetabolized folic acid (UMFA) begins to circulate in plasma. The long-term clinical significance of circulating UMFA is debated — some studies suggest possible associations with reduced natural killer cell function, masking of B12 deficiency, and possible cancer-cell proliferation in those with pre-existing neoplasia. Food folate from lentils does not produce UMFA because the conversion happens before plasma entry.
Folate in One-Carbon Metabolism
Folate's role in metabolism is to carry and donate single carbon units (methyl, methylene, formyl groups) for biosynthesis of:
- Purines (adenine and guanine) — required for DNA and RNA synthesis. Folate-dependent reactions add carbons C2 and C8 to the purine ring during de novo purine synthesis.
- Thymidylate (dTMP) — required for DNA synthesis specifically. The conversion of dUMP to dTMP requires 5,10-methylenetetrahydrofolate as the methyl donor; this step is targeted by the chemotherapy drug methotrexate, which inhibits DHFR and depletes the folate pool.
- Methionine — folate (as 5-MTHF) donates a methyl group to homocysteine in the methionine synthase reaction (B12-dependent), regenerating methionine. Methionine is then activated to S-adenosylmethionine (SAM), the universal methyl donor for over 200 methylation reactions including DNA methylation, neurotransmitter synthesis, and phospholipid synthesis.
The downstream consequences of folate deficiency therefore include:
- Impaired DNA synthesis — manifests as megaloblastic anemia (large, immature red blood cells because cell division is impaired), the classical hematologic sign of folate deficiency
- Elevated homocysteine — because the folate-dependent remethylation pathway cannot keep up with homocysteine production from methionine breakdown. Elevated homocysteine is an independent cardiovascular risk factor.
- Hypomethylation of DNA and proteins — can affect gene expression, epigenetic regulation, neurotransmitter synthesis (serotonin, dopamine), and myelination
- Neural tube defect — the most catastrophic and most-studied consequence of folate deficiency, occurring in the rapidly dividing neural plate cells around days 21-28 post-conception when the neural tube closes
For a broader discussion of folate biochemistry independent of lentils, see our Folate (Vitamin B9) page.
Neural Tube Defects and the MRC Trial
Neural tube defects (NTDs) are catastrophic congenital malformations resulting from failure of neural tube closure during weeks 3-4 of embryonic development. The major NTDs:
- Anencephaly — failure of cranial neural tube closure, leading to absence of the cerebral hemispheres and most of the skull. Universally fatal at or shortly after birth.
- Spina bifida — failure of caudal neural tube closure, with herniation of meninges and/or spinal cord through a vertebral defect. Causes variable degrees of lower extremity paralysis, neurogenic bladder, and hydrocephalus.
- Encephalocele — herniation of brain tissue through a skull defect.
Pre-fortification baseline incidence was approximately 1-2 per 1,000 live births in most populations, with strong geographic variation (higher in parts of China, Ireland, Egypt; lower in parts of South America).
The 1991 MRC Vitamin Study, conducted across 33 centers in 7 countries, randomized 1,817 women with a prior NTD pregnancy to one of four arms: folic acid 4 mg/day, multivitamin (no folic acid), folic acid + multivitamin, or placebo. Results:
- Folic acid arms had 72% reduction in NTD recurrence (6/593 vs 21/602; relative risk 0.28)
- Multivitamin without folic acid showed no significant protection
- The trial was stopped early on ethical grounds — the effect was so strong that continuing placebo was no longer acceptable
The 1992 Czeizel and Dudas NEJM trial extended the result to first-occurrence prevention (women without prior NTD history), randomizing 4,753 women to multivitamin including 0.8 mg folic acid or placebo. The folic acid arm had no NTDs vs 6 in the placebo arm.
The combined evidence led to the U.S. Public Health Service 1992 recommendation that all women of childbearing age consume 400 mcg of folic acid daily, and to mandatory folic acid fortification of cereal grain products in the United States (1998), Canada (1998), and over 80 other countries.
Periconceptional Timing: Why 4 Weeks Before Pregnancy Matters
Neural tube closure occurs between days 21-28 post-conception, which corresponds to roughly 5-6 weeks of gestation counted from the last menstrual period — before most women are aware they are pregnant. By the time a missed period or positive pregnancy test prompts the start of folic acid supplementation, the critical window for NTD prevention has already closed.
This is why all major guidelines (CDC, ACOG, WHO) recommend that women of childbearing age maintain folate sufficiency continuously rather than starting only after pregnancy is confirmed. The operational target is 400 mcg DFE/day before conception, increasing to 600 mcg DFE/day once pregnancy is confirmed.
For women with a prior NTD pregnancy (recurrence risk approximately 3% without supplementation), the recommended dose increases to 4 mg/day starting at least 4 weeks before conception — the MRC trial dose. For women with diabetes, those taking certain anticonvulsants (valproate, carbamazepine), or those with high BMI, the higher 4 mg dose is also typically recommended.
Roughly 50% of U.S. pregnancies are unplanned, which means a substantial fraction of NTD prevention opportunities are missed if intake depends on conscious preconception planning. This is the rationale for mandatory fortification — it elevates baseline folate intake across the entire population regardless of pregnancy intent.
The lentil contribution: a woman of childbearing age eating one cup of lentils daily, plus the background of fortified grain products and other vegetables, easily meets the 400 mcg DFE/day target without supplementation. This is the simplest food-based pathway to preconception folate sufficiency.
The MTHFR C677T Polymorphism
The MTHFR (methylenetetrahydrofolate reductase) gene encodes the enzyme that converts 5,10-methylene-THF to 5-methyl-THF (the active circulating folate form). A single nucleotide polymorphism at position 677 (C→T) substitutes valine for alanine at codon 222, producing a thermolabile enzyme with reduced activity:
- CC homozygous (wild type) — approximately 45-50% of the U.S. population. Normal enzyme activity.
- CT heterozygous — approximately 40-45% of the population. Approximately 65% of normal enzyme activity. Usually clinically silent.
- TT homozygous — approximately 10-15% of the U.S. population (higher in Mediterranean and Hispanic populations, lower in African populations). Approximately 30% of normal enzyme activity. Associated with mildly elevated homocysteine, slightly increased NTD risk, and reduced ability to convert synthetic folic acid to active 5-MTHF.
A second common polymorphism, A1298C, has smaller individual effects but compound heterozygotes (677CT + 1298AC) have intermediate phenotypes between CC and TT.
The clinical relevance for folate supplementation:
- TT homozygotes derive less benefit from synthetic folic acid because they cannot efficiently methylate it to active 5-MTHF. They may circulate higher levels of unmetabolized folic acid.
- TT homozygotes derive full benefit from food folate (already enters the metabolism as 5-MTHF after intestinal conversion) or from supplemental L-methylfolate.
- TT homozygotes who consume only synthetic folic acid as their folate source may have higher homocysteine and slightly higher NTD risk than CC homozygotes consuming the same total folate intake.
This is a meaningful argument for lentils as a folate source in preconception planning — they bypass the MTHFR conversion bottleneck entirely. For a more detailed discussion of MTHFR-aware supplementation strategies, see our Folate page.
5-MTHF vs Synthetic Folic Acid Supplementation
For women with confirmed or suspected MTHFR polymorphism (or any preconception woman who wants to bypass the conversion question), supplemental L-5-methyltetrahydrofolate is increasingly recommended. The most-studied branded forms are Metafolin (calcium L-5-MTHF, Merck) and Quatrefolic (glucosamine L-5-MTHF).
Typical preconception dosing for confirmed MTHFR TT homozygotes:
- 400-800 mcg of L-5-methylfolate daily (equivalent to or higher than 400 mcg folic acid)
- Started 3-4 months before planned conception
- Continued through pregnancy and lactation
The Pietrzik et al. 2010 review in Clinical Pharmacokinetics compared L-5-MTHF and folic acid: both raise plasma folate similarly when given to MTHFR CC patients; L-5-MTHF produces meaningfully higher red blood cell folate in TT patients; L-5-MTHF does not produce circulating unmetabolized folic acid (UMFA).
For women without MTHFR testing or with CC/CT genotype, standard folic acid or L-5-MTHF are both effective; the choice often comes down to cost and supplement form preference. Lentils as a daily food source provide the same 5-MTHF-equivalent endpoint without supplementation.
U.S. Fortification Policy and Its Effects
Mandatory U.S. folic acid fortification of enriched cereal grain products began in January 1998, requiring 140 mcg folic acid per 100 g of grain product. Predicted effects: approximately 100 mcg/day additional folate intake at the population level. Observed effects (per CDC surveillance):
- NTD incidence declined from approximately 10.7 per 10,000 live births pre-fortification to approximately 6.8 per 10,000 post-fortification — approximately 36% reduction, preventing roughly 1,300 NTD-affected pregnancies per year
- Mean serum folate in U.S. adults approximately doubled
- Plasma homocysteine declined population-wide
- The proportion of women of childbearing age with red blood cell folate below the NTD-protective threshold (906 nmol/L per WHO 2015 guidance) declined from approximately 25% to under 5%
The 2015 Tinker et al. Birth Defects Research paper estimated that despite fortification, approximately 23% of U.S. women of childbearing age still have suboptimal red blood cell folate, particularly women in their teens and early 20s, Hispanic women, and women with high BMI who have higher folate requirements. The lentil-as-folate-source strategy is particularly relevant for these gap populations.
Several countries have not implemented mandatory fortification (most of Europe, including the UK until 2024 when it began phased implementation), citing concerns about unmetabolized folic acid and potential cancer-cell proliferation. In unfortified countries, food folate from lentils, leafy greens, and citrus carries greater importance as the primary intake source.
Beyond Pregnancy: Homocysteine, Cardiovascular Disease, Cognition
Outside the pregnancy context, folate intake is most relevant for its role in regulating plasma homocysteine. Elevated homocysteine (hyperhomocysteinemia, >15 micromol/L) is:
- An independent risk factor for atherosclerotic cardiovascular disease
- An independent risk factor for stroke (particularly small-vessel disease)
- Associated with cognitive decline and dementia in observational studies
- Associated with osteoporosis and increased fracture risk
The remethylation of homocysteine to methionine requires both 5-MTHF (from folate) and methylcobalamin (from vitamin B12). Folate deficiency, B12 deficiency, or B6 deficiency (B6 is required for the alternative trans-sulfuration pathway to cystathionine) all elevate homocysteine.
Several large randomized trials of folate-plus-B-vitamin supplementation in established cardiovascular disease have shown modest or no reduction in cardiovascular events (HOPE-2, NORVIT, VISP), despite robust homocysteine lowering. This has tempered enthusiasm for folate supplementation as a CVD intervention, but the underlying mechanistic logic remains intact for dietary intake — population-level folate sufficiency from food sources contributes to lower baseline homocysteine and likely lower lifetime CVD risk.
For cognitive endpoints, the Smith and Refsum 2016 Annual Review of Nutrition summarizes evidence that B vitamin supplementation (folate, B12, B6) in elderly individuals with elevated homocysteine and mild cognitive impairment slows brain atrophy and improves cognitive performance. The most consistent benefit is seen in those with both elevated homocysteine and adequate omega-3 status — suggesting nutrient interactions rather than single-nutrient effects.
Practical Pregnancy Menu Engineering
A daily intake pattern that delivers the 600 mcg DFE pregnancy folate target primarily from food, with lentils as anchor:
- Breakfast — whole grain toast (fortified, ~70 mcg DFE) with avocado and a glass of orange juice (~80 mcg DFE), or a smoothie with spinach (~100 mcg DFE per cup).
- Lunch — lentil soup or salad (1 cup = 358 mcg DFE), with a side of broccoli or asparagus (~80 mcg DFE).
- Snack — orange or strawberries (~30-40 mcg DFE).
- Dinner — salmon or chicken with a leafy-green salad (romaine, spinach, arugula; ~60-100 mcg DFE) and brown rice.
- Daily total — approximately 700-800 mcg DFE, comfortably above the 600 mcg pregnancy target without supplementation.
For a woman with confirmed MTHFR TT polymorphism or for additional safety margin, a 400-800 mcg L-5-methylfolate supplement can be added on top of the food-based intake without producing the UMFA concerns that high-dose folic acid would raise.
The conventional ACOG recommendation remains a daily prenatal vitamin with 400-800 mcg folic acid throughout the pregnancy and during preconception planning. The food-based approach (anchored by daily lentils) and the supplement-based approach are complementary, not exclusive — many obstetricians recommend both.
Cautions (Including the Folate Trap)
- The B12 / Folate Trap — high folate intake can mask the hematologic signs of vitamin B12 deficiency (the megaloblastic anemia) while doing nothing to prevent the neurologic damage that B12 deficiency also causes. A B12-deficient patient supplementing with high-dose folate may have normal hemoglobin and MCV while irreversible peripheral neuropathy and subacute combined degeneration of the spinal cord progress unrecognized. Practical implication: in any folate-supplementing adult, check serum B12 at least annually, particularly in vegetarians, vegans, those on metformin, and adults over 50 (10-30% of whom have B12 absorption impairment from atrophic gastritis).
- Methotrexate interaction — methotrexate is a DHFR inhibitor used as chemotherapy and for autoimmune disease (rheumatoid arthritis, psoriasis). Its therapeutic effect depends partly on inducing folate-restricted conditions in dividing cells. High-dose folate supplementation can blunt methotrexate efficacy. Low-dose folate (1 mg/day folic acid) is conventionally given alongside methotrexate to reduce side effects without negating the therapeutic effect, but the dose is carefully balanced. Pregnant women with autoimmune disease on methotrexate face complex decisions; consult a maternal-fetal medicine specialist.
- Anti-epileptic drug interactions — phenytoin, phenobarbital, carbamazepine, valproate all reduce folate levels and increase NTD risk. Women on these drugs who could become pregnant are usually advised to take 4-5 mg folic acid daily, well above the standard preconception dose.
- Possible cancer interaction — high-dose folic acid supplementation (above 1 mg/day) has been associated in some studies with increased risk of recurrence in patients with prior colorectal adenomas. The mechanism is uncertain. Food folate from lentils is not implicated and likely protective rather than promotional.
- Unmetabolized folic acid (UMFA) — circulating UMFA from doses above ~200 mcg of folic acid has been associated in observational data with reduced natural killer cell function. The clinical significance is debated. Food folate does not produce UMFA.
- Lentil-specific cautions — see the cautions sections on Plant Protein and Iron and Soluble Fiber and Cholesterol for gas/bloating during adaptation, drug-absorption timing, and warfarin INR considerations.
Key Research Papers
- MRC Vitamin Study Research Group (1991). Prevention of neural tube defects: results of the Medical Research Council Vitamin Study. Lancet, 338(8760):131-137. — PubMed
- Czeizel AE, Dudas I (1992). Prevention of the first occurrence of neural-tube defects by periconceptional vitamin supplementation. NEJM, 327(26):1832-1835. — PubMed
- Frosst P et al. (1995). A candidate genetic risk factor for vascular disease: a common mutation in methylenetetrahydrofolate reductase. Nature Genetics, 10(1):111-113. — PubMed
- Pietrzik K, Bailey L, Shane B (2010). Folic acid and L-5-methyltetrahydrofolate: comparison of clinical pharmacokinetics and pharmacodynamics. Clinical Pharmacokinetics, 49(8):535-548. — PubMed
- Williams J et al. (2015). Updated estimates of neural tube defects prevented by mandatory folic acid fortification — United States, 1995-2011. MMWR, 64(1):1-5. — PubMed
- Tinker SC et al. (2015). U.S. women of childbearing age who are at possible increased risk of a neural tube defect-affected pregnancy. Birth Defects Research Part A: Clinical and Molecular Teratology, 103(6):517-526. — PubMed
- Crider KS et al. (2012). Folate and DNA methylation: a review of molecular mechanisms and the evidence for folate's role. Advances in Nutrition, 3(1):21-38. — PubMed
- Smith AD, Refsum H (2016). Homocysteine, B vitamins, and cognitive impairment. Annual Review of Nutrition, 36:211-239. — PubMed
- Lassi ZS et al. (2013). Folic acid supplementation during pregnancy for maternal health and pregnancy outcomes. Cochrane Database of Systematic Reviews. — PubMed
- Bailey LB et al. (2015). Biomarkers of nutrition for development — folate review. Journal of Nutrition, 145(7):1636S-1680S. — PubMed
- Botto LD et al. (1999). Neural-tube defects. NEJM, 341(20):1509-1519. — PubMed
- Pfeiffer CM et al. (2012). Estimation of trends in serum and RBC folate in the U.S. population from pre- to postfortification using assay-adjusted data from NHANES. Journal of Nutrition, 142(5):886-893. — PubMed
PubMed Topic Searches
- PubMed: Folate and NTD prevention
- PubMed: MTHFR C677T polymorphism
- PubMed: 5-MTHF vs folic acid
- PubMed: Folate, homocysteine, CVD
- PubMed: Folic acid fortification impact
Connections
- Lentils (Main Page)
- Lentils Benefits Hub
- Lentils for Plant Protein and Iron
- Lentils for Cholesterol
- Soaking and Phytates
- Folate (Vitamin B9)
- Vitamin B12
- Vitamin B6
- Pregnancy
- Neural Tube Defects
- Megaloblastic Anemia
- Homocysteine
- MTHFR Genetic Testing
- Spinach
- Asparagus
- Organ Meats (Liver)
- Chickpeas