Kimchi Sodium and Vegetable Trade-off
The honest scientific summary of kimchi is that it is a high-sodium fermented vegetable with documented probiotic and chemopreventive benefits, eaten in a country with one of the highest gastric cancer incidence rates in the developed world and one of the highest national sodium intakes. None of these statements contradict each other — they coexist, and the practical answer to "is kimchi good for me" depends on which framework you weight and what the rest of your diet looks like. This page walks through the Korean cohort epidemiology, the proposed sodium-and-gastric-cancer mechanism, the cardiovascular trade-offs, the lower-sodium home and commercial variants, and how to think about kimchi in a Western dietary context that already has its own sodium pressures from processed food.
Table of Contents
- Kimchi Sodium Content in Numbers
- The Korean Dietary Sodium Pattern
- The Gastric Cancer Signal
- Proposed Mechanism: Salt + Mucosal Damage + H. pylori
- Cardiovascular Trade-offs
- Confounding and the Whole-Diet Question
- Low-Sodium Kimchi Variants
- Home-Fermentation Guidance
- Who Should and Should Not Eat Kimchi
- Bottom Line
- Key Research Papers
- Connections
- Featured Videos
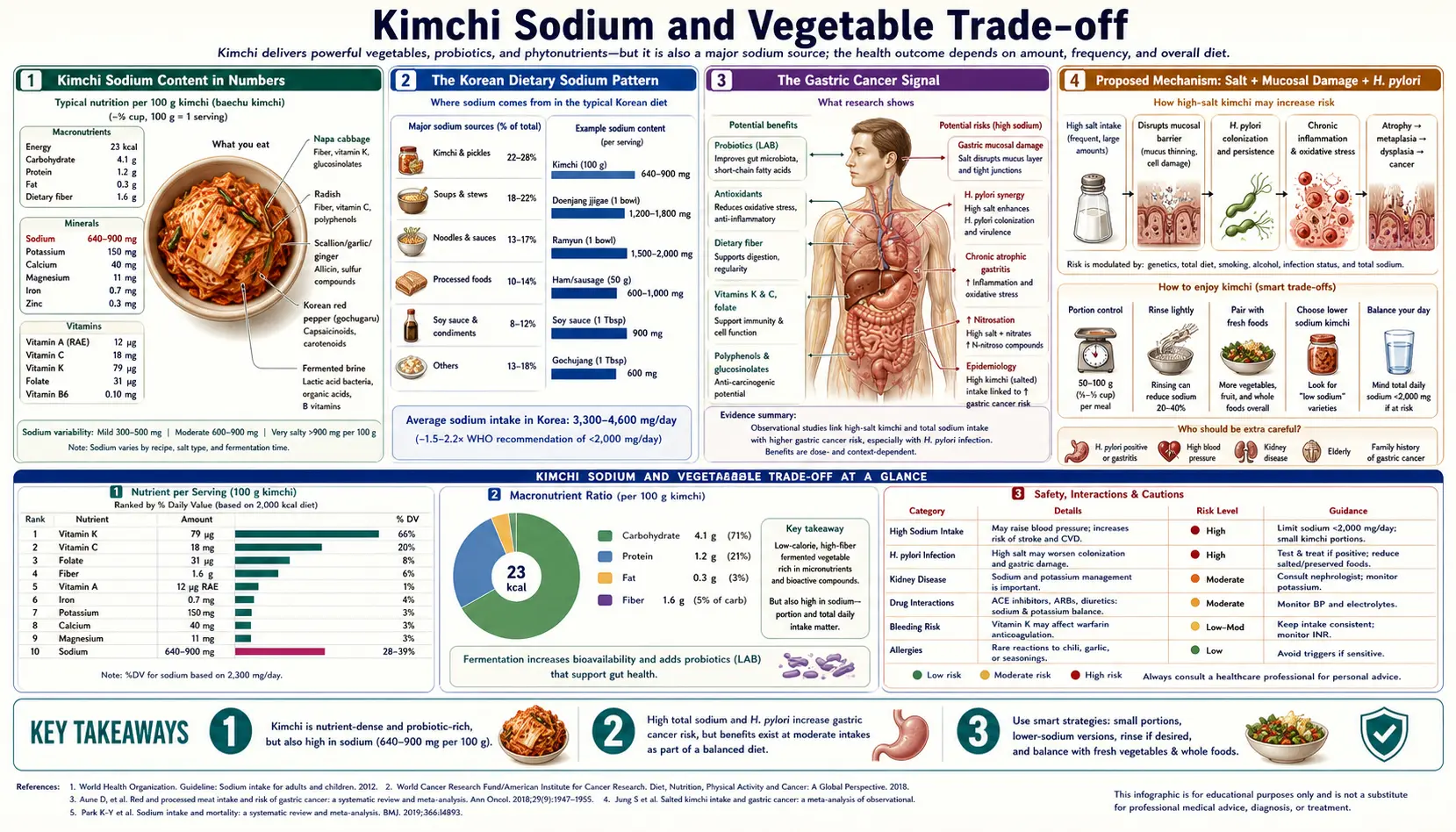
Kimchi Sodium Content in Numbers
The sodium content of kimchi is much higher than most consumers realize. Reference values from USDA, Korean Food Composition Database, and published analyses:
- Commercial baechu kimchi (napa cabbage) — 600-1,200 mg sodium per 100 g (1.5-3% salt by weight)
- Traditional kimjang home kimchi — often higher, 800-1,500 mg sodium per 100 g, reflecting the historical preservation requirement of higher salt for winter-long storage
- Kkakdugi (radish cube kimchi) — similar range, 600-1,000 mg per 100 g
- Dongchimi (water kimchi) — lower in the cabbage portion (300-500 mg per 100 g), but the brine is consumed and contains the bulk of the sodium
- Modern "low-sodium" commercial kimchi — 300-500 mg per 100 g, with the practical limit set by fermentation safety (below ~1.5% salt the fermentation outcome becomes unpredictable and food-safety risk rises)
For context, the American Heart Association recommended limit for total daily sodium intake is 1,500-2,300 mg per day. A single 100 g serving of commercial kimchi delivers 30-80% of that entire daily limit. A traditional Korean meal pattern of 100 g kimchi per meal, three meals per day, exceeds the entire AHA daily sodium recommendation from kimchi alone, before any other food.
This is not a small effect. Kimchi is genuinely a high-sodium food. The question is how that sodium intake interacts with the rest of the diet and with individual health risk factors.
The Korean Dietary Sodium Pattern
Korea has one of the highest national average sodium intakes in the developed world. KNHANES (Korean National Health and Nutrition Examination Survey) data over the past two decades have documented average sodium intake around 4,000-5,000 mg per day — roughly double the WHO recommendation and well above even the AHA upper-bound. The Korean government has run sustained national campaigns to reduce sodium intake, with measurable success: average intake has declined from approximately 5,300 mg/day in 2010 to approximately 3,300-3,500 mg/day in recent surveys, though still above target.
The major dietary contributors to Korean sodium intake, in approximate descending order:
- Soups and stews (jjigae, guk) — salted broths and stews are eaten at most meals; cumulatively the largest single sodium category
- Kimchi — second-largest single category; contributes roughly 15-25% of total daily sodium in traditional patterns
- Salt-fermented seafood (jeotgal) — concentrated salty condiments
- Fermented soybean pastes (doenjang, gochujang) — used in soups, marinades, sauces
- Soy sauce (ganjang) — primary salt-delivery condiment in many dishes
- Salted side dishes (banchan) — the array of small dishes accompanying rice; many are salted vegetables, dried fish, or pickled items
Critically, the Korean sodium signal is not from one food. Reducing only kimchi while leaving the other contributors unchanged would have a modest effect on total intake. The successful Korean public-health response has been broader — reformulating instant noodles, reducing soup and stew sodium, reformulating commercial kimchi, and educating consumers about hidden sodium in convenience foods.
The Gastric Cancer Signal
Korea has historically had one of the highest gastric (stomach) cancer incidence rates in the world, peaking at approximately 80 cases per 100,000 population per year in the 1990s. Rates have declined significantly with improved H. pylori eradication and dietary changes, but Korea remains in the top group globally. The Korean National Cancer Center has run a national gastric cancer screening program (biennial upper endoscopy starting at age 40) since 1999, which has substantially reduced gastric cancer mortality through early detection.
The dietary risk factor analysis from Korean cohort studies has consistently identified high-salt fermented foods as the principal modifiable risk factor for gastric cancer in this population. The signal includes:
- High kimchi intake — the highest-quintile consumers (typically >200 g/day kimchi) show elevated gastric cancer risk compared to lower-quintile consumers, with risk ratios in the 1.5-2.5 range in pooled analyses
- High salt-fermented seafood (jeotgal) intake — similar pattern, possibly stronger than kimchi
- High soup / stew intake — sodium delivery vehicle
- Pickled vegetables generally — same pattern in Japan with takuan, umeboshi, salt-fermented Chinese vegetables in China
The signal is not unique to Korean kimchi — it appears in similar form for traditional high-salt fermented foods across northeast Asia, central Asia, and parts of Europe (including the historical association between salt-pickled foods and gastric cancer in pre-refrigeration northern European populations). The pattern strongly implicates dietary sodium as the relevant exposure rather than any specific Korean ingredient.
Proposed Mechanism: Salt + Mucosal Damage + H. pylori
The mechanistic story behind sodium and gastric cancer involves an interaction with Helicobacter pylori infection — an intracellular gastric pathogen present in roughly 50% of the Korean adult population (down from 60-70% in the 1990s after national eradication efforts). The proposed pathway:
- High dietary sodium damages the gastric mucosal barrier — the gastric mucus-bicarbonate layer is normally a physical and chemical barrier protecting epithelial cells from the acidic luminal environment. Hyperosmolar salt exposure damages this barrier, exposing epithelial cells to acid and to luminal bacteria.
- Mucosal damage facilitates H. pylori colonization and effects — H. pylori already established in the gastric niche can more easily damage epithelial cells when the mucosal barrier is compromised. The CagA virulence factor (in CagA-positive H. pylori strains) is injected into gastric epithelial cells and disrupts cell signaling in ways that promote malignant transformation.
- Chronic atrophic gastritis develops — the combined insult of salt damage and H. pylori inflammation, sustained over decades, produces atrophic gastritis (loss of normal gastric glandular tissue), intestinal metaplasia (replacement with intestinal-type epithelium), dysplasia, and eventually adenocarcinoma
- N-nitroso compounds amplify the signal — nitrites and nitrates from various dietary sources (including fermented foods) can be reduced to bacterial-derived N-nitroso compounds in the achlorhydric stomach, which are direct carcinogens
The key insight is that the gastric cancer risk is concentrated in H. pylori-positive high-salt consumers. H. pylori-negative individuals with the same sodium intake have a much smaller incremental risk. Korea's national H. pylori eradication efforts have been a major driver of the gastric cancer incidence decline over the past 20 years, more than dietary change alone.
For more on H. pylori specifically, see our Helicobacter pylori page.
Cardiovascular Trade-offs
Beyond gastric cancer, high sodium intake has well-established cardiovascular effects: it raises blood pressure (with substantial individual variation in salt-sensitivity), increases left ventricular hypertrophy, accelerates renal damage in patients with pre-existing kidney disease, and is associated with cerebrovascular events. The Korean population shows higher rates of hypertension and stroke than would be predicted from BMI and other risk factors alone, consistent with the high-sodium dietary contribution.
The cardiovascular calculation for kimchi is more straightforward than the gastric cancer calculation:
- Normotensive individuals with normal kidney function — modest kimchi consumption (50-100 g/day) probably does not produce meaningful cardiovascular harm in the context of an otherwise sensible diet. The potassium in cabbage partially offsets the sodium effect on blood pressure.
- Salt-sensitive hypertensives, especially African-American, elderly, and pre-existing CKD — even modest kimchi consumption can produce measurable BP rises within hours. These patients should approach kimchi cautiously or use only low-sodium variants.
- Heart failure (especially HFpEF and HFrEF on diuretics) — sodium restriction is a cornerstone of management. Regular kimchi consumption is not compatible with serious heart failure management; small occasional servings are fine.
- Advanced CKD on sodium restriction — same consideration; the typical CKD diet allows ~2,000 mg/day total sodium, which a single 200 g kimchi serving could exceed
The probiotic and chemopreventive benefits of kimchi do not offset the cardiovascular effects of sodium in patients with established sodium-sensitive disease. The risk-benefit calculus is individual, not universal.
Confounding and the Whole-Diet Question
The Korean cohort epidemiology of kimchi-and-gastric-cancer is complicated by serious confounding. High-kimchi consumers are typically also high consumers of:
- Salt-fermented seafood (jeotgal) — possibly the larger gastric carcinogen signal
- Salted soups and stews
- Smoked and grilled meats (charred surface contains polycyclic aromatic hydrocarbons, also gastric carcinogens)
- Lower fresh-fruit-and-vegetable intake (the calories displaced by the heavy starch + side dish + kimchi pattern)
- Higher H. pylori carriage rates (older birth cohorts)
Disentangling the kimchi-specific effect from these covariates is methodologically difficult. Some studies, after adjustment, find that the kimchi-specific gastric cancer signal narrows substantially — the residual effect being driven mainly by the salt content rather than any kimchi-specific carcinogen. Other studies find a persistent kimchi signal even after adjustment. The honest reading is that kimchi is part of a broader high-salt dietary pattern that elevates gastric cancer risk, and the kimchi-specific marginal contribution depends on the other dietary choices made alongside it.
This is fundamentally a different question from "does kimchi cause gastric cancer in a low-salt Western dietary context?" The answer to that question is essentially unstudied because nobody eats 200 g/day kimchi in isolation while maintaining an otherwise low-sodium diet. Plausibly, the Westernized pattern of 50-100 g/day kimchi as part of a diet with modest total sodium (2,500-3,500 mg/day) does not carry the gastric cancer risk seen in the Korean cohorts. But this is extrapolation, not direct evidence.
Low-Sodium Kimchi Variants
Several practical approaches reduce kimchi sodium while preserving most of the probiotic and Brassica chemistry benefits:
- Commercial reduced-sodium kimchi — many Korean and Korean-American brands now offer 30-50% reduced-sodium versions. The fermentation is generally fine at 1.5-2% salt (the practical lower limit for reproducible LAB-dominant fermentation), and the flavor is identifiable as kimchi though slightly less pungent than the traditional version.
- Dongchimi (water kimchi) — the cabbage and radish are eaten without the brine, substantially reducing sodium intake per serving
- Rinsing kimchi briefly before serving — a quick water rinse reduces surface salt by 20-30%, with minor flavor impact. Useful for elderly or hypertensive consumers who want some kimchi without the full sodium load.
- Home fermentation at 1.5-1.8% salt — controllable, the fermentation outcome is usually fine, and the sodium content is 40-50% lower than commercial
- Potassium chloride salt substitution — partial replacement of sodium chloride with potassium chloride (typical ratios up to 30% KCl) is used in some commercial reduced-sodium products. KCl has a slightly bitter aftertaste but is generally acceptable at moderate substitution ratios. The added potassium has its own modest cardiovascular benefit (further offsets the sodium effect on BP). Note that KCl is contraindicated in advanced CKD and in patients on potassium-sparing diuretics or ACE inhibitors.
- Smaller serving sizes — 30-50 g per meal instead of 100 g per meal reduces the sodium exposure proportionally while still providing the live LAB, sulforaphane, and bioactive load
Home-Fermentation Guidance
Home fermentation gives the consumer direct control over the salt content, the seasonings, the fermentation timing, and the absence of preservatives and additives sometimes added to commercial products. Basic outline for reduced-sodium home kimchi (adapt to taste):
- Salt and brine the cabbage at 1.5-2% salt — for 2 kg napa cabbage, use 30-40 g coarse sea salt (no iodine, which can inhibit fermentation). Toss the quartered cabbage with salt, then submerge in light brine (3% brine, made with the same coarse salt) for 2-3 hours, weighting if needed to keep submerged. Rinse briefly and drain.
- Prepare the seasoning paste — grated Korean radish, scallion, garlic, ginger, gochugaru (Korean chili powder — use 2-4 tablespoons per kg cabbage depending on heat tolerance), and optional fermented seafood (saeujeot or anchovy sauce; use small amounts — these are concentrated sodium sources). Vegan: omit seafood, add 1-2 tablespoons of soaked dried shiitake plus 1 tablespoon of miso for umami.
- Mix and pack — rub the paste into the cabbage layers, pack tightly into a glass or onggi jar leaving 1-2 inches headspace, weight or use a fermentation airlock to maintain anaerobic conditions
- Ferment at room temperature 1-3 days — until you see active bubbling and a clearly sour taste develops. Then refrigerate.
- Refrigerator-ferment 1-3 weeks — the slow cold fermentation produces the mat-i-deulda flavor and the maximum LAB density. The kimchi continues to evolve in flavor for several weeks before passing peak quality.
Total sodium in this preparation will be approximately 300-500 mg per 100 g of finished kimchi — significantly less than commercial. The fermentation will still proceed reliably because the 1.5-2% salt is above the threshold for selecting LAB over spoilage organisms.
Who Should and Should Not Eat Kimchi
Kimchi is reasonable in moderation for:
- Healthy adults without hypertension, kidney disease, or heart failure, eating a generally low-to-moderate sodium baseline diet
- Patients with constipation or IBS who tolerate fiber and capsaicin
- Patients with food allergies and atopic conditions (LAB strains have favorable Treg effects)
- Adults interested in fermented food diversity and Brassica vegetable intake
Kimchi requires caution or avoidance in:
- Salt-sensitive hypertension — use only low-sodium variants and small portions
- Advanced chronic kidney disease — both sodium and potassium content are concerns
- Heart failure on sodium restriction — small occasional servings only
- History of gastric cancer or significant atrophic gastritis — minimize high-salt foods
- Active H. pylori infection without eradication therapy — the salt + bacteria interaction is the relevant mechanism
- Histamine intolerance or mast cell activation — fermented food histamine content can be problematic
- Severe immunocompromise (post-transplant, neutropenia, advanced HIV without ART) — live-bacteria food safety concern, though kimchi LAB are generally regarded as safe
- Children under 1 year — salt content and choking hazard from the cabbage texture
Bottom Line
Kimchi is a high-sodium fermented vegetable with real probiotic and Brassica-chemoprevention benefits. In the context of the broader high-sodium Korean dietary pattern, heavy lifelong kimchi consumption is associated with elevated gastric cancer risk via the salt-and-mucosal-damage mechanism in H. pylori-positive individuals. In the context of a moderate-sodium Western dietary pattern with modest kimchi consumption (50-100 g/day, perhaps a few times per week rather than three times daily), the risk-benefit balance is much more favorable.
The practical recommendation:
- Choose properly fermented (not pasteurized, not "fresh" geotjeori) kimchi to capture the live LAB benefit
- Eat moderate servings (50-100 g) with meals, not every meal
- Use reduced-sodium variants or home-ferment with 1.5-2% salt when possible
- Pay attention to total daily sodium intake from all sources, not just kimchi
- If H. pylori-positive, prioritize eradication therapy and approach high-salt fermented foods cautiously thereafter
- If hypertensive, in heart failure, or with advanced CKD, treat kimchi as an occasional small-portion food rather than a daily side dish
Key Research Papers
- Lee SA et al. (2003). Effect of diet and Helicobacter pylori infection to the risk of early gastric cancer. Journal of Epidemiology. — PubMed
- Kim HJ et al. (2002). Dietary factors and gastric cancer in Korea: a case-control study. International Journal of Cancer. — PubMed
- Tsugane S, Sasazuki S (2007). Diet and the risk of gastric cancer: review of epidemiological evidence. Gastric Cancer. — PubMed
- D'Elia L et al. (2012). Habitual salt intake and risk of gastric cancer: a meta-analysis of prospective studies. Clinical Nutrition. — PubMed
- Wang XQ et al. (2009). Review of salt consumption and stomach cancer risk: epidemiological and biological evidence. World Journal of Gastroenterology. — PubMed
- Cho SS et al. (2016). Trends in the prevalence of metabolic syndrome and its components in Korean adults: results from the KNHANES 1998-2014. Endocrinology and Metabolism. — PubMed
- Park J et al. (2018). Sodium intake estimation in Korean adults using 24-hour urine collection. Nutrition Research and Practice. — PubMed
- Song HJ et al. (2014). The relationship between sodium intake and obesity prevalence in Korean adults. Korean Journal of Community Nutrition. — PubMed
- Ha SK (2014). Dietary salt intake and hypertension. Electrolyte & Blood Pressure. — PubMed
- Kim SH et al. (2017). Reduced-sodium kimchi development for the elderly. Journal of the Korean Society of Food Science and Nutrition. — PubMed
- Suh M et al. (2017). Trends in body mass index and prevalence of obesity in Korean adults 1998 to 2014. Journal of Korean Medical Science. — PubMed
- Choi BY et al. (2010). The association between salt-sensitive blood pressure and high-salt foods in Korean adults. Korean Circulation Journal. — PubMed
PubMed Topic Searches
- PubMed: Kimchi sodium and gastric cancer
- PubMed: Salt + H. pylori + gastric cancer
- PubMed: KNHANES sodium intake
- PubMed: Low-sodium kimchi reformulation
- PubMed: Sodium and hypertension meta-analyses
Connections
- Kimchi Overview
- Kimchi Benefits Hub
- Lactobacillus Strains
- Sulforaphane and Cabbage
- Korean Tradition and Variants
- Sodium
- Potassium
- Hypertension
- Heart Failure
- Chronic Kidney Disease
- Gastric Cancer
- Helicobacter pylori
- Sauerkraut
- Yogurt
- DASH Diet