Kefir Gut Microbiome and Immune Function
The mechanism by which kefir produces clinical effect is not direct — the bacteria in kefir do not, for the most part, permanently colonize the gut. Instead, kefir acts through transient passage that produces three durable effects: ecological reshaping of the resident gut microbiome (favoring Bifidobacterium, Faecalibacterium prausnitzii, and other short-chain-fatty-acid producers), direct modulation of the gut-associated lymphoid tissue (GALT) by both live cells and their secreted metabolites, and competitive exclusion of pathobionts through bacteriocin production and pH lowering. The clinical literature in this area — particularly in Helicobacter pylori eradication, irritable bowel syndrome, inflammatory bowel disease, and antibiotic-associated diarrhea — consistently shows clinically meaningful benefit, with effect sizes that compare favorably with high-dose single-strain commercial probiotics.
Table of Contents
- The Gut-Associated Lymphoid Tissue (GALT)
- Short-Chain Fatty Acid Production and GPR43 Signaling
- Th17 / Treg Balance and Butyrate
- Bacteriocin Production and Pathobiont Exclusion
- H. pylori Eradication as Adjunct Therapy
- Irritable Bowel Syndrome Evidence
- Inflammatory Bowel Disease Evidence
- Antibiotic-Associated Diarrhea Prevention
- Systemic Immune Effects Beyond the Gut
- Cautions and Patient Selection
- Key Research Papers
- Connections
- Featured Videos
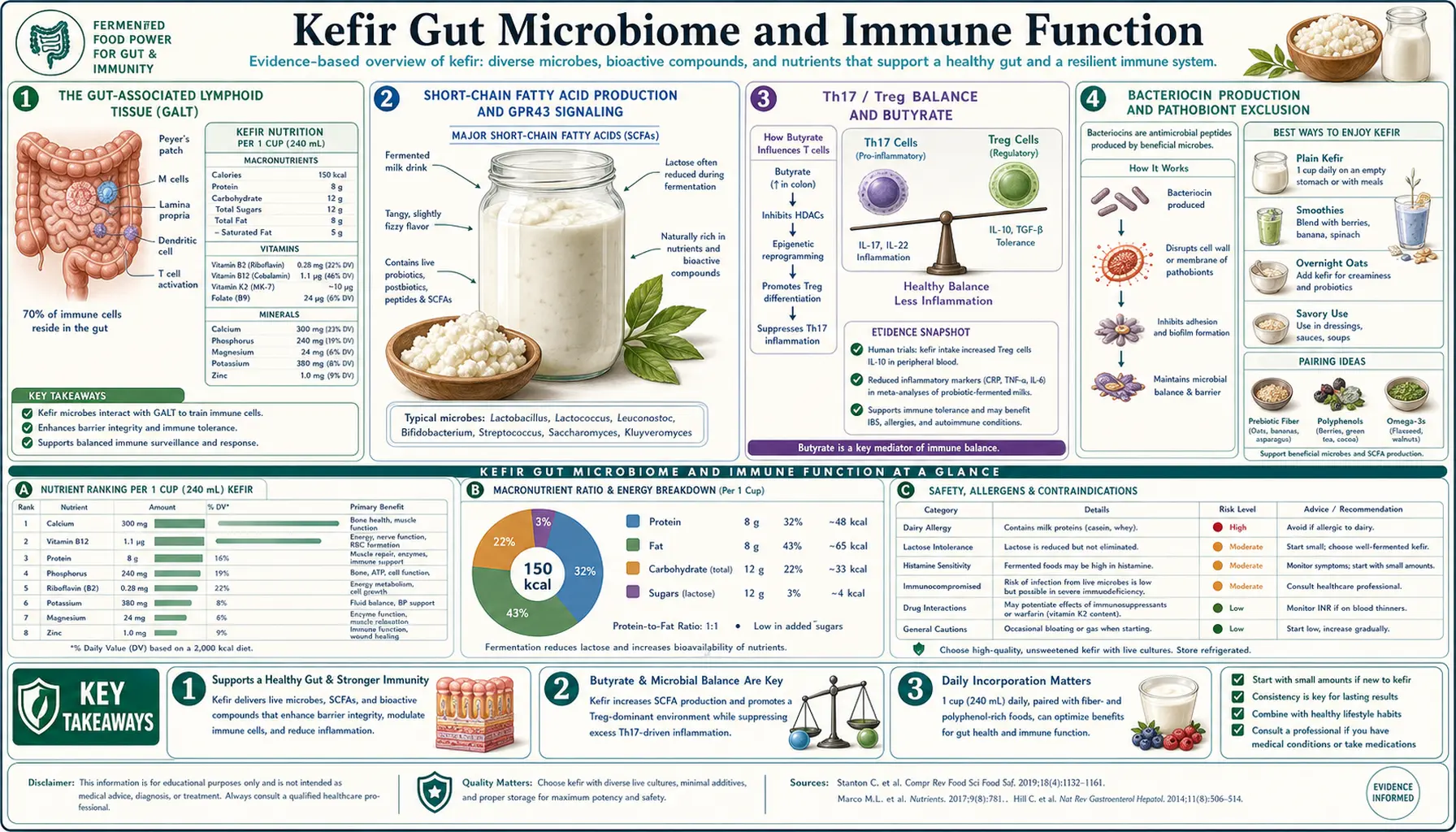
The Gut-Associated Lymphoid Tissue (GALT)
The gut-associated lymphoid tissue (GALT) is the largest single immune organ in the human body, containing approximately 70% of all immune cells. It is anatomically organized into discrete structures (Peyer's patches in the small intestine, isolated lymphoid follicles, mesenteric lymph nodes, and the appendix) plus diffuse populations of intraepithelial lymphocytes and lamina propria lymphocytes distributed throughout the gut wall. The GALT is in continuous dialogue with the gut microbiome through several interfaces: M cells in the Peyer's patch epithelium sample luminal contents; dendritic cells extend processes between epithelial cells to directly sample the lumen; and microbial metabolites (short-chain fatty acids, bacteriocins, surface proteins, peptidoglycan fragments) cross the epithelium to signal directly to lamina propria immune cells.
Kefir microbes and their metabolites engage this dialogue at multiple points. The viable cells, even when transient, are sampled by dendritic cells and trigger appropriate Th-cell responses. The kefiran exopolysaccharide is detected by Toll-like receptor 2 (TLR2) on macrophages, producing a mild and balanced cytokine response. The lactic acid lowers luminal pH, suppressing acid-sensitive pathobionts. The bacteriocins selectively kill competing bacteria. And the resident gut microbiome is fed by the prebiotic components of kefir, with measurable downstream changes in Bifidobacterium and short-chain fatty acid producer abundance after 2-4 weeks of daily consumption.
The net effect is an immunomodulatory rather than immunosuppressive or immunostimulatory signal — kefir tends to push the GALT toward a balanced regulatory state rather than either extreme, which is mechanistically consistent with its clinical effect of improving both excess-inflammation conditions (IBS, IBD) and infection-defense conditions (H. pylori, antibiotic-associated diarrhea).
Short-Chain Fatty Acid Production and GPR43 Signaling
The downstream metabolic effect of kefir on the gut microbiome is concentrated in increased production of short-chain fatty acids (SCFAs) by resident gut bacteria — particularly acetate, propionate, and butyrate. SCFAs are produced by fermentation of dietary fiber and resistant starch by colonic anaerobes including Bifidobacterium, Faecalibacterium prausnitzii, Roseburia, and Eubacterium. Kefir does not directly produce most of these SCFAs (kefir microbes produce primarily lactic and acetic acid), but kefir consumption shifts the resident colonic microbiota toward higher-SCFA-producing communities, with measurable increases in fecal butyrate within 2-4 weeks.
The SCFAs in turn produce wide-ranging effects:
- Butyrate is the preferred energy substrate of colonocytes, providing 60-70% of their oxidative metabolism. Increased butyrate supply restores colonocyte energy status and barrier function.
- SCFAs bind G-protein-coupled receptors GPR41, GPR43, and GPR109A on intestinal epithelial cells, dendritic cells, T cells, and enteroendocrine cells, triggering anti-inflammatory signaling cascades.
- Butyrate is an HDAC inhibitor at physiological colonic concentrations, with downstream effects on gene expression in both the host epithelium and lamina propria immune cells.
- SCFAs strengthen the colonic mucus barrier by upregulating mucin-2 (Muc2) production by goblet cells.
- SCFAs promote Treg differentiation via GPR43 signaling, biasing the local immune environment toward tolerance and away from inflammation.
These mechanisms link kefir consumption to measurable improvements in gut barrier function (reduced lipopolysaccharide translocation, lower serum zonulin), reduced inflammatory cytokines (TNF-alpha, IL-6, IL-17), and clinical improvement in conditions characterized by gut barrier dysfunction.
Th17 / Treg Balance and Butyrate
The Th17/Treg balance is one of the most studied axes in modern immunology. Th17 cells produce IL-17 and IL-22 and are central to defense against extracellular bacteria and fungi but also drive multiple autoimmune conditions when chronic and untargeted (psoriasis, ankylosing spondylitis, inflammatory bowel disease, multiple sclerosis). Treg cells produce IL-10 and TGF-beta and maintain peripheral tolerance to self-antigens, commensal microbes, and food antigens.
Butyrate, produced in increased amounts by the kefir-modulated gut microbiome, is a powerful regulator of this balance. Butyrate promotes Treg differentiation via GPR43 signaling and inhibits Th17 differentiation through HDAC inhibition that affects the transcription factor RORgt. The net effect of increased butyrate availability is a shift in the local mucosal immune environment toward tolerance and away from chronic Th17-driven inflammation.
This is the mechanistic basis for the observed clinical effect of kefir in inflammatory bowel disease, where Th17/Treg disequilibrium with excess Th17 activity is one of the immunopathological hallmarks. It is also part of the explanation for kefir's effect in allergic and atopic disease, where loss of tolerance to harmless antigens is the underlying problem.
Bacteriocin Production and Pathobiont Exclusion
Several kefir Lactobacillus species produce bacteriocins — ribosomally-synthesized antimicrobial peptides that selectively kill competing bacteria while leaving the producing strain and most other commensals unharmed. The best-characterized kefir bacteriocins include kefiricin from L. kefiri, lactocin S from various Lactobacillus species, and nisin-class bacteriocins from Lactococcus lactis. These peptides:
- Selectively kill many gram-positive pathobionts, including Listeria monocytogenes, Staphylococcus aureus, and certain Clostridium species
- Operate in the low-pH environment of the upper GI tract where most antibiotic peptides are degraded
- Function in synergy with the lactic-acid-driven pH drop that excludes acid-sensitive pathogens
- Have no documented resistance development, unlike conventional antibiotics
The competitive exclusion produced by bacteriocin-secreting kefir microbes is part of the explanation for the protective effect against Clostridium difficile infection observed in some clinical and preclinical studies, and for the reduced post-antibiotic dysbiosis seen when kefir is consumed during and after antibiotic courses.
H. pylori Eradication as Adjunct Therapy
The strongest body of clinical evidence for kefir in any disease is in Helicobacter pylori eradication. H. pylori is a gram-negative spiral bacterium that colonizes the gastric mucosa and is the dominant cause of peptic ulcer disease and gastric cancer worldwide. Standard treatment is "triple therapy" — a proton pump inhibitor plus two antibiotics (typically clarithromycin and amoxicillin or metronidazole) for 7-14 days. The treatment is moderately effective (eradication rates of 60-80% in many series due to growing antibiotic resistance) and has substantial side effects (taste disturbance, nausea, antibiotic-associated diarrhea, vaginal yeast infection, oral thrush).
The 2011 Bekar et al. randomized trial enrolled 82 H. pylori-positive Turkish patients to receive either standard triple therapy alone or triple therapy plus 250 mL kefir twice daily for 14 days. Results:
- Eradication rate at 8 weeks post-treatment: 78% in kefir group vs 50% in control (statistically significant)
- Frequency of treatment-related diarrhea was significantly lower in the kefir group
- Patient-reported epigastric symptom relief was significantly better in the kefir group
- No serious adverse events attributable to kefir
Several subsequent studies and meta-analyses have replicated the benefit, with effect sizes ranging from a 10% to 25% improvement in eradication rate when kefir is added to standard therapy. The mechanism is thought to involve direct competitive inhibition of H. pylori by kefir bacteriocins and lactic acid, plus the reduction in antibiotic-associated diarrhea (which improves adherence and probably enhances apparent eradication by reducing nausea-driven dose missing). For the broader picture of H. pylori management, see our H. pylori page.
Irritable Bowel Syndrome Evidence
Irritable bowel syndrome (IBS) is the most common gastrointestinal diagnosis worldwide, affecting 10-15% of adults in Western populations. The pathophysiology is incompletely understood but involves gut microbiome alterations (loss of diversity, reduced Bifidobacterium, expansion of methanogens in IBS-C), low-grade mucosal inflammation, increased gut permeability, visceral hypersensitivity, and altered gut-brain axis signaling. Probiotics broadly are an established treatment option, with meta-analyses showing approximately 25-30% improvement in symptom scores over placebo.
Kefir specifically has been studied in several small trials. The Yilmaz 2019 trial in 31 IBS patients showed significant improvements in abdominal pain, bloating, and stool consistency after 4 weeks of 400 mL/day kefir. Other trials have shown similar benefits, generally larger than what is seen with single-strain probiotic supplements. The species diversity advantage of kefir likely contributes to the relatively robust IBS effect.
For IBS patients, the practical protocol is: introduce kefir gradually (50 mL/day for one week, ramping to 250-400 mL/day over 2-3 weeks), prefer home-fermented over commercial, and assess effect at 4-6 weeks. For more on IBS management, see our IBS page and SIBO page (relevant because some apparent IBS is actually SIBO, and kefir effects in SIBO are more variable).
Inflammatory Bowel Disease Evidence
Inflammatory bowel disease (IBD) — Crohn's disease and ulcerative colitis — involves chronic immune-mediated inflammation of the gut. Disease activity is associated with reduced microbiome diversity, loss of butyrate-producing species, increased Th17 activity, and disrupted gut barrier function — all of which kefir mechanistically addresses.
The clinical trial evidence in IBD is smaller than in IBS but consistently favorable. A 2014 trial of 25 Crohn's patients showed improved Bifidobacterium abundance and reduced inflammatory markers after 4 weeks of daily kefir consumption. Multiple animal-model studies of L. kefiranofaciens M1 (isolated from kefir grains) demonstrate dose-dependent reduction in disease activity score and histological inflammation in chemically-induced colitis models.
For IBD patients, kefir is best regarded as an adjunct to standard therapy (5-ASA, immunomodulators, biologics) rather than a primary treatment. Start with small volumes (25-50 mL/day) and increase based on tolerance — some IBD patients have transient symptom worsening when introducing any new fermented food. Patients on immunosuppression (especially anti-TNF biologics, JAK inhibitors, methotrexate) should discuss with their gastroenterologist before adding live-microbe foods. For more on IBD, see our Crohn's page.
Antibiotic-Associated Diarrhea Prevention
Antibiotic-associated diarrhea (AAD) affects 5-30% of patients receiving systemic antibiotics, with rates highest in elderly hospitalized patients and those receiving broad-spectrum agents (clindamycin, broad-spectrum cephalosporins, carbapenems, fluoroquinolones). The most dangerous form is Clostridium difficile colitis, which causes 15,000-30,000 deaths per year in the United States. Probiotic supplementation reduces AAD risk by approximately 50% in meta-analyses, with strain-specific evidence strongest for Saccharomyces boulardii (a yeast) and Lactobacillus rhamnosus GG.
Kefir contains both yeasts (similar mechanism to S. boulardii) and high-diversity lactic acid bacteria, and is a reasonable food-based alternative to commercial probiotic capsules during antibiotic courses. The practical protocol: 100-200 mL kefir 2-3 hours after each antibiotic dose for the duration of the course and for 1-2 weeks after completion. Timing matters — consuming kefir concurrent with the antibiotic kills most of the kefir microbes before they can reach the gut.
Importantly, several kefir species (notably L. kefiranofaciens and L. kefiri) have intrinsic resistance to many antibiotics including amoxicillin, clarithromycin, and metronidazole, which is one mechanism behind the H. pylori triple-therapy benefit discussed above.
Systemic Immune Effects Beyond the Gut
Although kefir microbes act primarily at the gut, downstream systemic immune effects have been documented. The Adiloglu 2013 trial measured serum cytokines before and after 6 weeks of daily kefir consumption in 18 healthy adults. Results showed:
- Increased Th1 cytokines (IFN-gamma, IL-12) — supports antiviral and intracellular bacterial immunity
- Increased IL-10 (regulatory) — reflects increased Treg activity
- Decreased Th2 cytokines (IL-4, IL-5) — relevant to allergic disease
- No change in TNF-alpha in healthy subjects (but reductions in disease states characterized by elevated TNF-alpha)
The pattern is consistent with a balanced immunomodulatory effect — not generic stimulation, but a shift toward antiviral (Th1) and regulatory (Treg) phenotypes with reduction in allergic (Th2) signaling. Animal-model trials of kefir in allergic disease (asthma, atopic dermatitis, food allergy) have consistently shown reductions in allergic markers, mechanistically explained by the Th2-suppressing effect plus increased Treg activity.
For viral respiratory infection prevention, the evidence is suggestive but not definitive. Several observational studies have associated regular fermented-dairy consumption with reduced respiratory infection incidence, but no large controlled trial of kefir specifically for respiratory infection prevention exists. The biological plausibility is strong (Th1 skewing, mucosal IgA enhancement, increased natural killer cell activity) but the clinical evidence remains preliminary.
Cautions and Patient Selection
- Severe immunosuppression — patients with HIV/AIDS at low CD4 count, post-organ-transplant on potent immunosuppressants, chemotherapy-induced neutropenia, primary immunodeficiency. The risk of opportunistic infection from any live-microbe food (including kefir) is non-zero in these populations. Discuss with the transplant/oncology team before adding kefir.
- Histamine intolerance — some kefir species produce biogenic amines including histamine during fermentation. Patients with severe histamine intolerance or mast cell activation syndrome may experience headache, flushing, or GI symptoms with kefir. Shorter ferment times reduce histamine content.
- SIBO with severe bloating — in patients with active SIBO, any high-fermentation food including kefir can transiently worsen bloating. Address SIBO first (typically with rifaximin or herbal antimicrobials) before introducing high-dose kefir. After SIBO resolution, kefir can support post-treatment gut recovery.
- Severe lactose intolerance — most lactose-intolerant patients tolerate kefir well because of the dramatic reduction in lactose during fermentation. The minority who do not tolerate any dairy-based kefir can use water kefir (tibicos) — see our Tibicos page.
- Galactosemia — the rare genetic disorder of galactose metabolism is an absolute contraindication to any dairy product including kefir.
- Children under 12 months — cow's milk is generally not recommended as a primary beverage under 12 months. Kefir made from breast milk or formula is not standard practice and should not be undertaken without pediatric input.
- Alcohol-restricted populations — mature kefir contains 0.5-2% alcohol from yeast fermentation, which may be relevant for those in alcohol recovery or with strict religious restrictions.
Key Research Papers
- Bekar O, Yilmaz Y, Gulten M (2011). Kefir improves the efficacy and tolerability of triple therapy in eradicating Helicobacter pylori. Journal of Medicinal Food. — PubMed
- Yilmaz I, Dolar ME, Ozpinar H (2019). Effect of administering kefir on the changes in fecal microbiota and symptoms of inflammatory bowel disease. Turkish Journal of Gastroenterology. — PubMed
- Adiloglu AK, Gonulates N, Isler M, Senol A (2013). The effect of kefir consumption on human immune system: a cytokine study. Mikrobiyoloji Bulteni. — PubMed
- Vinderola CG et al. (2005). Effects of the oral administration of the products derived from milk fermentation by kefir microflora on immune stimulation. Journal of Dairy Research. — PubMed
- Hsieh HH, Wang SY, Chen TL, Huang YL, Chen MJ (2012). Effects of cow's and goat's milk as fermentation media on the microbial ecology of sugary kefir grains. International Journal of Food Microbiology. — PubMed
- Bourrie BCT, Willing BP, Cotter PD (2016). The microbiota and health-promoting characteristics of the fermented beverage kefir. Frontiers in Microbiology. — PubMed
- de Moreno de LeBlanc A, Matar C, Farnworth E, Perdigon G (2007). Study of immune cells involved in the antitumor effect of kefir in a murine breast cancer model. Journal of Dairy Science. — PubMed
- Hertzler SR, Clancy SM (2003). Kefir improves lactose digestion and tolerance in adults with lactose maldigestion. Journal of the American Dietetic Association. — PubMed
- Tu MY et al. (2015). The prophylactic effects of kefir against irradiation-induced damage. Journal of Functional Foods. — PubMed
- Maeda H, Zhu X, Suzuki S, Suzuki K, Kitamura S (2004). Structural characterization and biological activities of an exopolysaccharide kefiran. Journal of Agricultural and Food Chemistry. — PubMed
- Carasi P et al. (2015). Impact of kefir derived Lactobacillus kefiri on the mucosal immune response and gut microbiota. Journal of Immunology Research. — PubMed
- Hsieh HH, Wang SY, Liu YJ, Chen TL, Chen MJ (2012). Lactobacillus kefiranofaciens M1 isolated from milk kefir grains ameliorates experimental colitis. British Journal of Nutrition. — PubMed
PubMed Topic Searches
- PubMed: Kefir H. pylori
- PubMed: Kefir IBS
- PubMed: Kefir IBD/colitis
- PubMed: Kefir immune cytokines
- PubMed: SCFA butyrate Treg
Connections
- Kefir Overview
- Kefir Benefits Hub
- Probiotic Diversity
- Tibicos vs Milk Kefir
- Make Kefir at Home
- Irritable Bowel Syndrome
- SIBO
- H. pylori Infection
- Crohn's Disease
- Probiotics
- Immune Boosting
- Fermented Foods
- Yogurt
- Vitamin D3
- All Foods