Kale, Vitamin K, and Bone Health
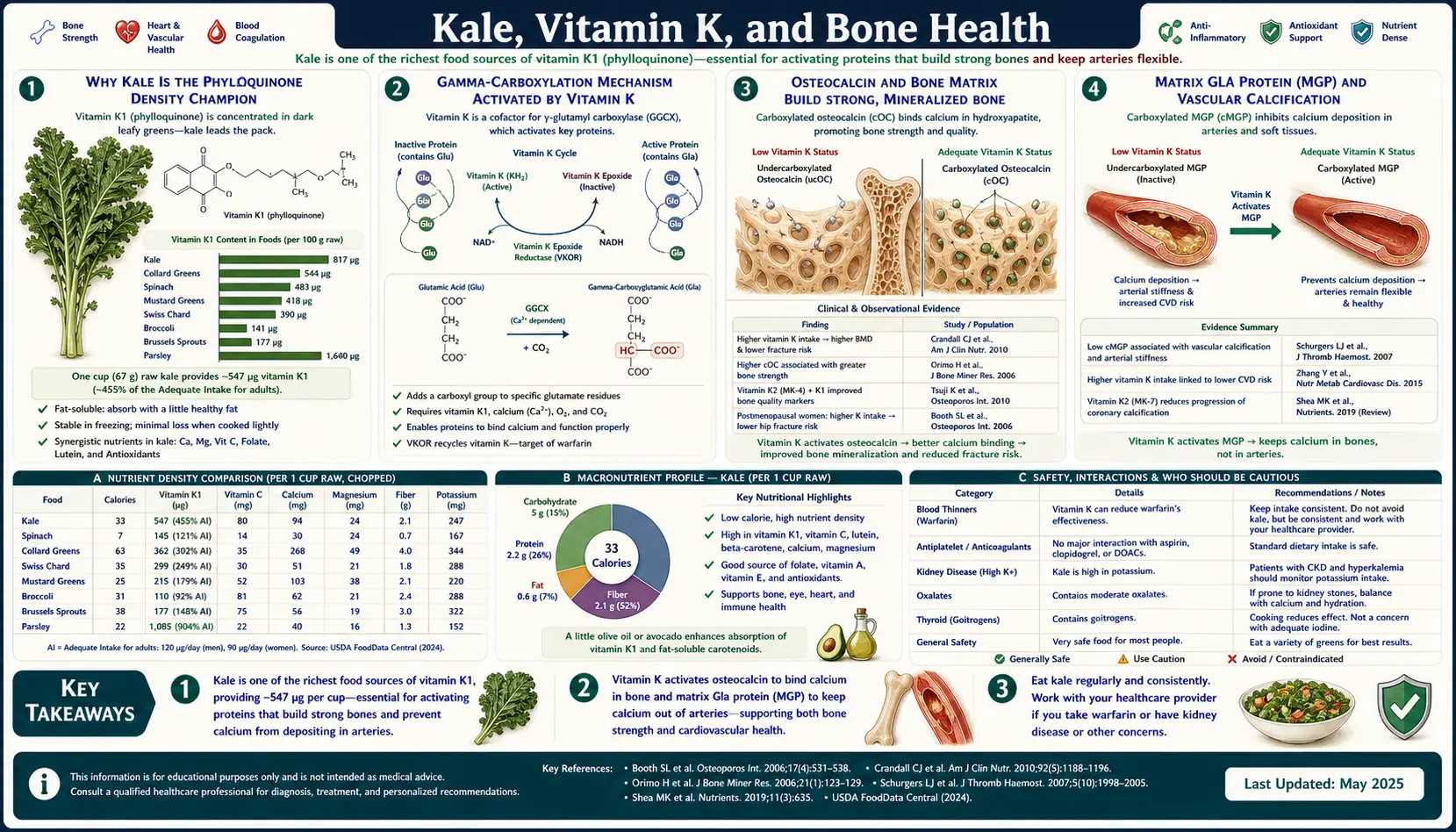
Kale is the densest commonly consumed food source of phylloquinone (Vitamin K1), delivering roughly 547 micrograms in a single 67-gram cup of raw chopped leaves — more than five times the adult Adequate Intake. Vitamin K1 functions as the obligate cofactor for the gamma-glutamyl carboxylase enzyme, which converts glutamate residues to gamma-carboxyglutamate (Gla) residues on a dozen target proteins. Two of those proteins are central to skeletal health: osteocalcin (the most abundant non-collagen protein in bone matrix) and matrix Gla protein (the master inhibitor of vascular calcification). Adequately carboxylated osteocalcin binds calcium and directs it into hydroxyapatite crystal formation in bone; under-carboxylated osteocalcin (ucOC) does neither, and ucOC concentration is one of the strongest individual biomarkers of hip-fracture risk in older women. This deep-dive walks through the biochemistry, the pivotal observational and interventional trials, the K1-to-MK-4 tissue conversion question, and the practical clinical issues for warfarin patients, bisphosphonate combination therapy, and the everyday consumer trying to reach the 90-120 mcg adequate intake from food alone.
Table of Contents
- Why Kale Is the Phylloquinone Density Champion
- The Gamma-Carboxylation Mechanism
- Osteocalcin and Bone Matrix
- Matrix Gla Protein and Vascular Calcification
- K1 vs K2 (MK-4 / MK-7): Conversion in Tissues
- Hip-Fracture Epidemiology and Intervention Data
- The Warfarin Interaction (Consistency, Not Avoidance)
- Practical Applications for Adults
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
Why Kale Is the Phylloquinone Density Champion
Phylloquinone (the IUPAC name for Vitamin K1, 2-methyl-3-phytyl-1,4-naphthoquinone) is synthesized exclusively in plant chloroplasts, where it functions as an electron carrier in photosystem I. The highest concentrations occur in the photosynthetic green leaves of plants with the densest chloroplast packing, and within that category kale sits at the top. The USDA FoodData Central database lists raw curly kale at 817 micrograms of phylloquinone per 100 grams of fresh weight, with cooked kale slightly higher per gram (after water loss) at 817-1,062 micrograms.
For reference, the adult Adequate Intake (AI) for Vitamin K set by the Institute of Medicine is 120 micrograms per day for adult men and 90 micrograms per day for adult women. A single 67-gram cup of raw chopped kale delivers approximately 547 micrograms — roughly five times the AI for women and four-and-a-half times the AI for men. Compare to spinach (483 mcg/100 g raw), collard greens (407 mcg), Swiss chard (830 mcg cooked), or romaine (102 mcg). Kale's combination of phylloquinone density, year-round availability, palatability across cooking methods, and the ease of consuming 60+ grams in a single sitting makes it the practical winner.
It is worth noting that the AI for Vitamin K was set in 2001 based primarily on the prothrombin time requirement for normal coagulation. There is widespread scientific consensus that this AI is set too low to optimally support the extra-hepatic Vitamin K-dependent proteins (osteocalcin in bone, matrix Gla protein in vasculature). The European Food Safety Authority adequate intake is similarly set to support coagulation, not bone or vascular endpoints. Researchers including Cees Vermeer (Maastricht University) have argued that the optimal intake for bone and vascular health is closer to 200-300 micrograms per day for K1 plus 100-200 micrograms per day for MK-7 — intakes most easily achieved through one cup of cooked kale (or two cups of raw) plus modest fermented-food consumption.
The Gamma-Carboxylation Mechanism
Vitamin K functions as the obligate cofactor for a single enzymatic reaction: the gamma-carboxylation of specific glutamate (Glu) residues to gamma-carboxyglutamate (Gla) residues on target proteins. The enzyme is gamma-glutamyl carboxylase (GGCX), located on the endoplasmic reticulum membrane. The reaction adds a second carboxyl group to the gamma carbon of glutamate, converting it from a singly-charged amino acid to a doubly-charged dicarboxylic acid that can chelate two calcium ions with high affinity.
The mechanism is a coupled cycle. Reduced Vitamin K (hydroquinone form, KH2) is oxidized to Vitamin K epoxide (KO) during the carboxylation reaction; KO is then recycled back to the active hydroquinone by the vitamin K epoxide reductase complex (VKORC1). This recycling is efficient — one Vitamin K molecule can carboxylate many target proteins before being lost — which is why daily Vitamin K requirements are modest despite the dozen target proteins involved.
Warfarin works by inhibiting VKORC1, blocking the recycling step. Without VKORC1 activity, oxidized Vitamin K epoxide accumulates and the active reduced form is depleted, halting gamma-carboxylation across all Vitamin K-dependent proteins. The clinical effect on coagulation appears first (factors II, VII, IX, X have short half-lives), but the effect on osteocalcin and matrix Gla protein is part of the long-term picture in chronic warfarin users.
The dozen Vitamin K-dependent (VKD) proteins fall into three functional groups: hepatic coagulation factors (II/prothrombin, VII, IX, X, plus regulatory proteins C, S, Z), extra-hepatic structural Gla proteins (osteocalcin in bone, matrix Gla protein in vasculature, periostin in bone-tendon interfaces, Gas6 in cell signaling), and the newly recognized GRP (Gla-rich protein) involved in soft-tissue calcification regulation. Kale supports all of them through dietary phylloquinone supply.
Osteocalcin and Bone Matrix
Osteocalcin (also called bone Gla protein, BGP) is the most abundant non-collagen protein in the bone matrix, synthesized exclusively by osteoblasts. It is a small 49-amino-acid protein with three glutamate residues at positions 17, 21, and 24 that are gamma-carboxylated by GGCX in the presence of Vitamin K. The fully carboxylated form (cOC) binds calcium with high affinity and helps direct calcium and phosphate into the hydroxyapatite crystal lattice that gives bone its compressive strength.
Under-carboxylated osteocalcin (ucOC) is osteocalcin synthesized when Vitamin K supply is inadequate — the protein backbone is normal but the Gla residues are missing. UcOC cannot bind calcium effectively, cannot incorporate properly into bone matrix, and is released into circulation. The ratio of serum ucOC to total osteocalcin is a sensitive, validated biomarker of Vitamin K status, more responsive than coagulation parameters (which require severe deficiency) and predictive of fracture risk in prospective cohort studies.
The Framingham Heart Study cohort showed an inverse association between dietary Vitamin K intake and hip fracture risk that has been replicated in the Nurses' Health Study, the Health Professionals Follow-up Study, and multiple European cohorts. Pooled relative risk for hip fracture among individuals in the highest dietary K quintile vs the lowest is approximately 0.65-0.75 across studies. The effect is independent of calcium intake and Vitamin D status, supporting a direct mechanistic role rather than a confounding general-healthy-diet signal.
For the broader bone-health picture — calcium, Vitamin D3, magnesium, and the K2 / D3 interaction — see our Osteoporosis page and our Vitamin D3 page.
Matrix Gla Protein and Vascular Calcification
The second major extra-hepatic Vitamin K-dependent protein is matrix Gla protein (MGP), synthesized by vascular smooth muscle cells in the arterial wall. MGP is the master inhibitor of vascular calcification — the pathological deposition of calcium hydroxyapatite in the intima and media of arteries that drives arterial stiffness, isolated systolic hypertension, and the cardiovascular risk associated with chronic kidney disease.
The clinical relevance to kale and dietary K: low Vitamin K status produces under-carboxylated MGP (ucMGP, measured as dephospho-uncarboxylated MGP, dp-ucMGP), which loses its calcification-inhibitor function. Elevated dp-ucMGP predicts cardiovascular mortality independently of traditional risk factors in multiple prospective cohorts (Rotterdam Study, EPIC-Norfolk, dialysis populations). This is the mechanism behind the seemingly paradoxical finding that warfarin-treated patients accumulate vascular calcification faster than comparable patients on direct oral anticoagulants (DOACs) like apixaban or rivaroxaban — warfarin inhibits MGP carboxylation along with the intended coagulation-factor carboxylation, while DOACs only block downstream factor Xa or thrombin.
For the kale eater specifically, the implication is favorable: adequate dietary K1 (plus K1-derived MK-4 in tissues) supports MGP carboxylation and may slow the progression of vascular calcification. For more on the cardiovascular role of micronutrients, see our Atherosclerosis page.
K1 vs K2 (MK-4 / MK-7): Conversion in Tissues
Vitamin K2 (menaquinones) refers to a family of naphthoquinones with isoprenyl side chains of varying lengths, named by the number of isoprenyl units — MK-4 (4 units, found in animal tissues), MK-7 (7 units, produced by Bacillus subtilis in natto fermentation), and longer chains (MK-9, MK-10) produced by other bacteria. K2 forms have markedly longer plasma half-lives than K1 (K1: ~1-2 hours; MK-7: ~72 hours) and partition preferentially into extra-hepatic tissues like bone and vasculature.
For decades it was assumed that dietary K1 supported only hepatic coagulation factor synthesis, while extra-hepatic proteins (osteocalcin, MGP) required dietary K2. This is now known to be incomplete. The UBIAD1 enzyme (also called TBC) in extra-hepatic tissues cleaves the phytyl side chain from K1 and replaces it with a geranylgeranyl chain, converting K1 to MK-4 within the tissue where it is needed. So dietary K1 from kale is, in effect, converted into MK-4 in bone, vasculature, brain, pancreas, and other tissues that express UBIAD1.
The conversion efficiency is not 1:1, and there is genetic variability in UBIAD1 expression. So while dietary K1 alone can support extra-hepatic Vitamin K-dependent protein carboxylation in most healthy adults with adequate intake, supplementing with MK-7 may provide additional benefit for individuals with documented elevated dp-ucMGP, post-menopausal bone loss, or chronic kidney disease. The Vermeer group's clinical trials have used 180 mcg/day MK-7 with measurable reductions in dp-ucMGP over 12 weeks. See our Vitamin K page for the broader K1 / K2 strategy.
The practical implication for the kale eater: a daily cup of cooked kale (or its equivalent in other dark leafy greens) supplies abundant K1, and most healthy adults can support normal Gla-protein carboxylation from food alone. Adding MK-7 supplementation makes sense in specific clinical contexts (osteoporosis, CKD, post-menopausal women with elevated dp-ucMGP) but is not necessary as a baseline.
Hip-Fracture Epidemiology and Intervention Data
The strongest clinical evidence connecting dietary Vitamin K to skeletal endpoints comes from large prospective cohorts measuring hip-fracture incidence as a function of dietary K intake quintile. Three studies stand out:
- Nurses' Health Study (Feskanich 1999) — 72,327 women followed for 10 years. Women in the highest quintile of Vitamin K intake (median ~110 mcg/day) had a 30% lower hip-fracture risk than women in the lowest quintile (median ~13 mcg/day). The strongest dietary contributor to the high-quintile intake was lettuce, kale, and broccoli.
- Framingham Heart Study (Booth 2000) &mdashj; 888 men and women followed for 7 years. The highest dietary K quartile had a 65% lower hip-fracture risk than the lowest quartile, after adjustment for age, sex, BMI, calcium, and Vitamin D.
- Japanese MK-4 trials — pharmacological-dose MK-4 (45 mg/day, far above dietary intake) has been used in Japan as treatment for osteoporosis since 1995, with prospective trials showing reduced fracture incidence. This is a pharmacological intervention, not a dietary one, but it confirms the mechanistic link.
Direct intervention trials of dietary kale (vs supplementation) on fracture endpoints are not available — sample sizes and follow-up duration required make such trials impractical. The case for kale as a fracture-prevention strategy is therefore based on the convergent evidence from the K1 epidemiology, the MK-4 intervention trials, and the mechanistic data on osteocalcin carboxylation. The case is strong but circumstantial.
The Warfarin Interaction (Consistency, Not Avoidance)
The most common clinical conversation about kale concerns its interaction with warfarin (Coumadin). The mechanism is direct: warfarin inhibits VKORC1, blocking Vitamin K recycling and producing anticoagulation. A sudden large increase in dietary Vitamin K (e.g., starting a daily kale-smoothie habit) provides more substrate for the residual gamma-carboxylation activity, reducing the anticoagulant effect and dropping the INR — potentially below therapeutic range and increasing thromboembolic risk. Conversely, a sudden cessation of dietary K (e.g., a hospitalization with limited diet) reduces the substrate, increasing the anticoagulant effect and raising the INR — potentially producing bleeding.
The historical clinical advice was to avoid leafy greens entirely on warfarin. This is now considered outdated and potentially harmful, because it deprives the patient of the cardiovascular, bone-protective, and general nutritional benefits of leafy greens. The modern guidance is consistency, not avoidance:
- Determine a typical daily intake of green leafy vegetables, set a target (often expressed as cups per week), and stick to that pattern week to week
- The warfarin dose is then titrated to maintain INR in therapeutic range (typically 2.0-3.0) at the stable dietary K intake
- Avoid large episodic variations — not the steady consumption itself
- If a major dietary change is planned (starting or stopping a smoothie habit, changing to a vegetarian diet, etc.), inform the prescribing clinician so the warfarin dose can be re-titrated
Patients on direct oral anticoagulants (DOACs — apixaban, rivaroxaban, edoxaban, dabigatran) do not have a dietary Vitamin K interaction because DOACs do not work through VKORC1. The DOAC patient can eat kale freely. This is one of the practical advantages that has driven the displacement of warfarin by DOACs over the past 15 years for the atrial fibrillation indication.
Practical Applications for Adults
The realistic kale-for-bones strategy for an average adult:
- Target intake — one cup of cooked kale (or roughly two cups of raw, massaged with olive oil and lemon juice) provides 800-1000 mcg of phylloquinone, well above the AI and at the level researchers identify as optimal for bone and vascular endpoints. Daily consumption is not required — 3-4 times per week is sufficient to maintain elevated tissue K1 stores
- Cook with fat — Vitamin K is fat-soluble; cooked kale dressed with olive oil or sauteed with butter or ghee delivers 3-5x the bioavailability of raw or fat-free preparations
- Combine with K2 strategy — for post-menopausal women, individuals over 65, or anyone with osteopenia or osteoporosis, adding 90-180 mcg MK-7 daily provides additive benefit beyond dietary K1 alone
- Pair with adequate Vitamin D3 and calcium — the Vitamin K-dependent gamma-carboxylation of osteocalcin only matters if there is calcium to incorporate and Vitamin D3 to support intestinal calcium absorption. Target 25(OH)D3 of 40-60 ng/mL and dietary calcium of 800-1200 mg/day
- Watch the iron interaction — non-heme iron in kale is poorly absorbed compared to heme iron from animal sources, but Vitamin C in the same meal enhances it significantly. Vitamin K does not impair iron absorption
- If on warfarin — eat kale on a consistent weekly schedule, inform the anticoagulation clinic of any major dietary changes, and target stable INR rather than dietary K avoidance
Cautions and Drug Interactions
- Warfarin (Coumadin) — the cornerstone interaction, discussed above. Consistency matters more than avoidance; INR monitoring is the safety net
- Antibiotics that suppress gut flora — long-term broad-spectrum antibiotics can reduce gut bacterial menaquinone production, increasing dietary K1 requirements. Kale supports this requirement effectively
- Cholestyramine and bile-acid sequestrants — reduce fat-soluble vitamin absorption including Vitamin K. Take kale at meals separated from the medication by 4+ hours
- Orlistat (Xenical, Alli) — the lipase inhibitor reduces absorption of all fat-soluble vitamins including K. Consider supplementation if on chronic therapy
- Antiepileptics (phenytoin, phenobarbital, carbamazepine) — accelerate hepatic Vitamin K catabolism and may produce subclinical K deficiency with chronic use, particularly in pregnancy
- Chronic kidney disease (advanced) — the elevated dp-ucMGP is a marker of inadequate functional K status. Both dietary K1 (kale) and supplemental MK-7 are appropriate; however, very high potassium content in kale may require portion limits if hyperkalemia is a concern. Discuss with the nephrology team
- Kidney-stone-forming history — kale's modest oxalate content (~20 mg per 100 g raw) is usually safe in moderation, but multi-cup daily green-smoothie intake can push oxalate load high enough to matter. See our oxalate page
- Hypothyroidism on levothyroxine — mature kale has modest goitrogenic potential in iodine-deficient individuals. Iodine-replete adults (most Americans, given iodized salt) can consume kale without thyroid concern. See the cooking page
Key Research Papers
- Feskanich D, Weber P, Willett WC, Rockett H, Booth SL, Colditz GA (1999). Vitamin K intake and hip fractures in women: a prospective study. American Journal of Clinical Nutrition. PMID: 9925137 — Search PubMed
- Booth SL, Tucker KL, Chen H, Hannan MT, Gagnon DR, Cupples LA, Wilson PW, Ordovas J, Schaefer EJ, Dawson-Hughes B, Kiel DP (2000). Dietary vitamin K intakes are associated with hip fracture but not with bone mineral density in elderly men and women. American Journal of Clinical Nutrition. PMID: 10799384 — Search PubMed
- Cockayne S, Adamson J, Lanham-New S, Shearer MJ, Gilbody S, Torgerson DJ (2006). Vitamin K and the prevention of fractures: systematic review and meta-analysis of randomized controlled trials. Archives of Internal Medicine. PMID: 16801507 — PubMed 16801507
- Schurgers LJ, Vermeer C (2002). Differential lipoprotein transport pathways of K-vitamins in healthy subjects. Biochimica et Biophysica Acta. PMID: 11900868 — Search PubMed
- Nakagawa K, Hirota Y, Sawada N, Yuge N, Watanabe M, Uchino Y, Okuda N, Shimomura Y, Suhara Y, Okano T (2010). Identification of UBIAD1 as a novel human menaquinone-4 biosynthetic enzyme. Nature. PMID: 21102434 — Search PubMed
- Schurgers LJ, Cranenburg EC, Vermeer C (2008). Matrix Gla-protein: the calcification inhibitor in need of vitamin K. Thrombosis and Haemostasis. PMID: 18841273 — PubMed 18841273
- Knapen MH, Drummen NE, Smit E, Vermeer C, Theuwissen E (2013). Three-year low-dose menaquinone-7 supplementation helps decrease bone loss in healthy postmenopausal women. Osteoporosis International. PMID: 23525894 — PubMed 23525894
- Booth SL, Centi A, Smith SR, Gundberg C (2013). The role of osteocalcin in human glucose metabolism: marker or mediator? Nature Reviews Endocrinology. PMID: 23149970 — Search PubMed
- Geleijnse JM, Vermeer C, Grobbee DE, Schurgers LJ, Knapen MH, van der Meer IM, Hofman A, Witteman JC (2004). Dietary intake of menaquinone is associated with a reduced risk of coronary heart disease: the Rotterdam Study. Journal of Nutrition. PMID: 15514282 — PubMed 15514282
- Shea MK, Booth SL (2016). Concepts and Controversies in Evaluating Vitamin K Status in Population-Based Studies. Nutrients. PMID: 26901221 — Search PubMed
- Booth SL, Pennington JA, Sadowski JA (1996). Food sources and dietary intakes of vitamin K-1 (phylloquinone) in the American diet: data from the FDA Total Diet Study. Journal of the American Dietetic Association. PMID: 8568090 — Search PubMed
- Vermeer C, Joyce I, Theuwissen E (2017). Vitamin K, an underestimated vitamin. Network Health Digest (review) PubMed: Vermeer reviews
PubMed Topic Searches
- PubMed: Phylloquinone hip fracture
- PubMed: Osteocalcin K status
- PubMed: MGP and vascular calcification
- PubMed: Warfarin and dietary K
- PubMed: MK-7 postmenopausal bone
Connections
- Kale (Main Page)
- Kale Benefits Hub
- Kale for Lutein/Eye Health
- Kale Glucosinolates and Cancer
- Kale Oxalates and Cooking
- Vitamin K (K1 and K2)
- Vitamin D3 (Calcium Partner)
- Calcium
- Magnesium
- Osteoporosis
- Atherosclerosis
- Spinach
- Broccoli
- Natto (MK-7 Source)
- Lab: Vitamin K Status (ucOC)