Green Tea EGCG and Antioxidants
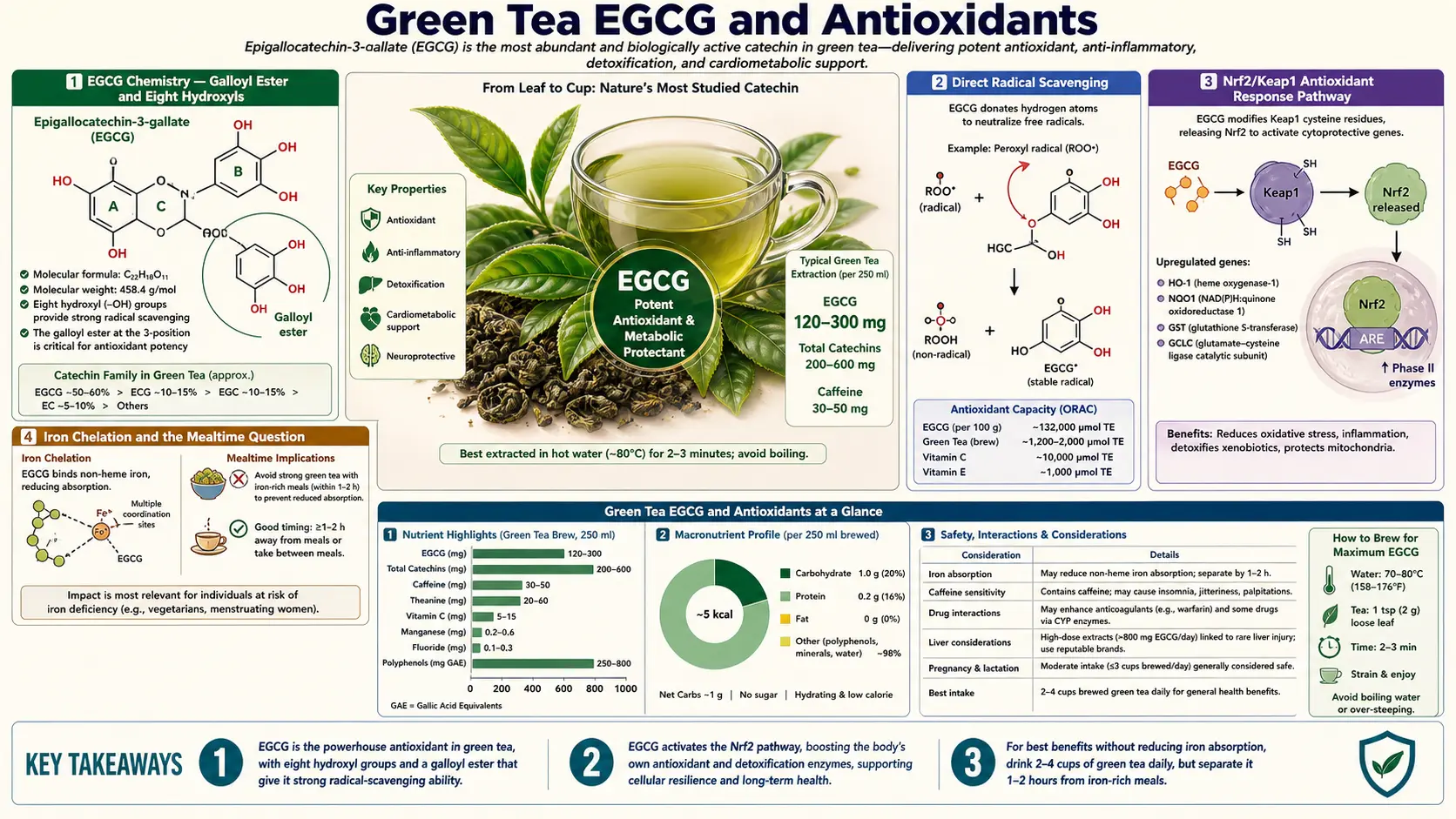
Epigallocatechin-3-gallate (EGCG) is the most extensively studied single polyphenol in nutritional science. It comprises roughly 50-80% of the catechin fraction in green tea, accounts for the majority of the bitter astringent mouthfeel, and is the molecule responsible for nearly every laboratory and clinical antioxidant endpoint that distinguishes green tea from other beverages. Yet "antioxidant" is the easy half of the story. EGCG's real biology is more interesting: it is a relatively weak direct radical scavenger compared to vitamin C or glutathione, but a potent inducer of the body's endogenous antioxidant enzyme machinery through the Nrf2/Keap1 pathway. And at high purified-extract doses, it inverts to a pro-oxidant capable of hepatocyte injury. This page walks through the chemistry, the mechanism, the human evidence, and the dose-toxicity inversion that explains why the brewed beverage is exceptionally safe while the concentrated capsule is not.
Table of Contents
- EGCG Chemistry — The Galloyl Ester and Eight Hydroxyls
- Direct Radical Scavenging
- The Nrf2 / Keap1 Antioxidant Response Pathway
- Iron Chelation and the Mealtime Question
- EGCG Bioavailability — The Real-World Plasma Curve
- Dose-Response and the Effective Cup Count
- The Dose-Toxicity Inversion (Pro-Oxidant Behavior)
- Hepatotoxicity and the EFSA 800 mg Limit
- Concentrated Supplement Versus Brewed Beverage
- Drug Interactions and Cautions
- Key Research Papers
- Connections
- Featured Videos
EGCG Chemistry — The Galloyl Ester and Eight Hydroxyls
Catechins are a subclass of flavonoids called flavan-3-ols. Their two-ring core (A-ring fused to a pyranose, joined to a B-ring) carries hydroxyl groups whose count and arrangement determine the molecule's antioxidant chemistry. Four major catechins are present in green tea: epicatechin (EC), epigallocatechin (EGC), epicatechin gallate (ECG), and epigallocatechin-3-gallate (EGCG). Of these, EGCG is by far the most abundant (50-80% of catechin mass in typical Japanese sencha) and the most pharmacologically active.
The "epigallo" prefix means the B-ring carries three adjacent hydroxyls (3', 4', 5' positions) in a vicinal triol arrangement. The "gallate" suffix means a galloyl ester — another three-hydroxyl gallic acid moiety — is attached to the 3-position of the C-ring. The net result is a single molecule carrying eight phenolic hydroxyl groups, all of which can donate a hydrogen atom or an electron to neutralize a radical species. This is unusually dense reducing power for a small molecule of just under 460 Daltons.
The vicinal triol arrangement on the B-ring also gives EGCG its characteristic ability to chelate divalent metal cations — iron, copper, zinc, calcium — through coordination at the two adjacent hydroxyls. The galloyl ester at the 3-position contributes additional chelation sites. This polyphenol-metal binding is the chemistry behind both the iron-absorption interaction (a real and clinically meaningful effect on non-heme iron uptake) and a substantial portion of the indirect antioxidant effect: chelating iron prevents it from catalyzing Fenton-reaction hydroxyl radical generation in the first place.
Direct Radical Scavenging
The simplest mechanism by which EGCG behaves as an antioxidant is direct radical scavenging: a hydroxyl, peroxyl, superoxide, or other reactive species encounters an EGCG molecule, abstracts a hydrogen atom from one of the eight phenolic hydroxyls, and is thereby quenched. EGCG itself becomes a relatively stable phenoxyl radical, stabilized by resonance across the aromatic ring, and can either be regenerated by ascorbate or further oxidized to a quinone.
In standard test-tube assays (DPPH, ABTS, ORAC), EGCG scores extremely high — often higher than ascorbic acid on a molar basis and orders of magnitude higher than alpha-tocopherol. This is why early enthusiasm cast green tea as the "highest antioxidant beverage." The problem with extrapolating from test-tube assays to humans is that plasma EGCG concentrations after drinking tea are quite low — peak concentrations rarely exceed 1 micromolar, compared to ascorbate at 50-80 micromolar and urate at 200-300 micromolar. On a population basis, ascorbate, urate, and reduced glutathione vastly outweigh EGCG as direct radical scavengers in human plasma.
The implication is that direct radical scavenging by EGCG, while real, is probably not the dominant mechanism by which green tea consumption translates into measurable antioxidant benefit in humans. The more important mechanism is indirect: EGCG induces the body's own endogenous antioxidant enzyme machinery to produce more glutathione, more superoxide dismutase, more catalase, and more glutathione peroxidase. That mechanism — the Nrf2/Keap1 pathway — is the topic of the next section.
The Nrf2 / Keap1 Antioxidant Response Pathway
Nrf2 (nuclear factor erythroid 2-related factor 2) is the master transcription factor controlling the cell's antioxidant response. Under basal conditions, Nrf2 is held in the cytoplasm by Keap1 (Kelch-like ECH-associated protein 1), which targets Nrf2 for proteasomal degradation. Keap1 carries a set of reactive cysteine residues. When those cysteines are modified by an electrophilic or oxidative stimulus, Keap1 releases Nrf2, which translocates to the nucleus, dimerizes with small Maf proteins, and binds antioxidant response elements (AREs) in the promoter regions of more than 200 cytoprotective genes.
The Nrf2 target gene set includes:
- Glutathione synthesis enzymes — gamma-glutamyl-cysteine ligase (GCLC, GCLM), the rate-limiting enzymes for glutathione production
- Glutathione utilization enzymes — glutathione S-transferases (GSTs), glutathione peroxidases (GPxs)
- NADPH-regenerating enzymes — glucose-6-phosphate dehydrogenase, 6-phosphogluconate dehydrogenase
- Direct antioxidant enzymes — superoxide dismutase (SOD), catalase, thioredoxin reductase, peroxiredoxins
- Phase II detoxification enzymes — NAD(P)H quinone dehydrogenase 1 (NQO1), heme oxygenase-1 (HO-1), UDP-glucuronosyltransferases (UGTs)
EGCG activates Nrf2 indirectly: at modest concentrations it produces a low-grade oxidative or electrophilic signal in the cell that modifies Keap1's reactive cysteines, releasing Nrf2 to translocate to the nucleus and induce the cytoprotective response. The cell, in effect, perceives EGCG as a mild stressor and ramps up its endogenous antioxidant defenses in response. This is the hormesis principle that underlies much of the polyphenol-and-health story.
The implication is that the meaningful antioxidant benefit of green tea is not the direct quenching done by the EGCG molecules circulating in plasma. It is the elevated steady-state glutathione, SOD, and catalase activity in tissues that results from chronic mild Nrf2 stimulation. This is why habitual tea consumption produces measurable reductions in oxidative DNA damage markers (urinary 8-hydroxy-2'-deoxyguanosine), F2-isoprostanes, and lipid peroxidation products — while acute single-dose tea consumption typically does not.
Iron Chelation and the Mealtime Question
The vicinal triol on the EGCG B-ring is an excellent chelator of ferric (Fe3+) iron. When tea is consumed with a meal, EGCG and the other catechins bind dietary non-heme iron in the lumen of the small intestine, forming insoluble polyphenol-iron complexes that are not absorbed. The classic Hallberg and Rossander work in the 1980s documented a 60-90% reduction in non-heme iron absorption when tea was consumed concurrently with a meal — far larger than the inhibition produced by coffee, milk, or calcium supplements.
This is clinically meaningful in two opposite directions:
- Iron-deficient population (premenopausal women, vegetarians, gastric bypass patients, chronic blood loss) — tea consumption with meals contributes to iron-deficiency risk and should be separated from iron-rich meals by at least 1-2 hours. This is the single most important practical caution for habitual green tea drinkers who are female of reproductive age or have any other risk factor for iron deficiency.
- Iron-overload population (hereditary hemochromatosis, thalassemia, repeat-transfusion recipients) — tea consumption with meals can be a useful adjunct to phlebotomy or chelation therapy by reducing dietary iron absorption. Small clinical series have explored green tea extract as adjunctive therapy in thalassemia major.
The chelation also has an indirect antioxidant benefit: chelating intestinal iron prevents iron-catalyzed lipid peroxidation in the gut lumen, which has been hypothesized as one mechanism by which polyphenol-rich diets reduce colorectal cancer risk. The same chelation chemistry contributes to systemic antioxidant effect by reducing free-iron-driven Fenton chemistry in tissues, although the magnitude of the systemic effect is modest because absorbed EGCG plasma concentrations are low.
For more on iron physiology, see our Iron page. For tea drinkers who are iron-deficient, the simple rule is: tea between meals, not with meals. Coffee has the same interaction (though smaller) due to its chlorogenic acid content.
EGCG Bioavailability — The Real-World Plasma Curve
EGCG bioavailability from brewed green tea is poor by pharmaceutical standards. Peak plasma EGCG concentrations after a typical cup of tea (containing 50-100 mg EGCG) are in the 0.1-0.5 micromolar range, with peak time around 90-150 minutes and an elimination half-life of approximately 3-5 hours. After a higher dose (200-400 mg EGCG from concentrated extract), peak concentrations reach 1-3 micromolar.
Several factors limit oral bioavailability:
- Intestinal stability — EGCG degrades in the alkaline pH of the small intestine, with substantial losses to oxidation and epimerization to gallocatechin gallate (GCG)
- Efflux transport — absorbed EGCG is partly pumped back into the gut lumen by intestinal P-glycoprotein and MRP2 efflux pumps
- First-pass conjugation — absorbed EGCG is extensively conjugated to methylated, sulfated, and glucuronidated metabolites in the intestinal wall and liver, reducing the fraction of free EGCG that reaches systemic circulation
- Microbial metabolism — unabsorbed EGCG reaching the colon is degraded by gut bacteria to lower-molecular-weight phenolic acids (3-(3',4',5'-trihydroxyphenyl)propionic acid and related metabolites), some of which may have their own biological activity
One practical implication: taking EGCG on an empty stomach roughly doubles peak plasma concentrations compared to taking it with food. This is one reason high-dose concentrated green tea extract supplements taken on an empty stomach have been associated with idiosyncratic hepatotoxicity at much lower nominal doses than equivalent EGCG intake from food.
A second practical implication: EGCG plasma concentrations from realistic tea consumption never reach the high-micromolar concentrations used in most in vitro studies of EGCG anticancer or anti-inflammatory activity. Translation from cell culture to whole organism for EGCG is more strained than for most nutraceuticals. The meaningful in vivo effects of habitual tea consumption are mediated more by Nrf2 induction, gut-microbiome metabolite formation, and chronic low-grade signaling than by acute high-concentration direct effects.
Dose-Response and the Effective Cup Count
Epidemiologic and clinical-trial data converge on a roughly 3-5 cup per day intake as the range where measurable benefits on cardiovascular, metabolic, and cancer-related endpoints emerge. The Ohsaki cohort (Kuriyama 2006, 40,530 Japanese adults) found that consumers of five or more cups per day had a 16% lower all-cause mortality and a 31% lower cardiovascular mortality in women compared to consumers of less than one cup per day, with a dose-response gradient through the intermediate categories.
Typical EGCG content per cup varies considerably by leaf grade, brewing technique, and steep time. A standard 8-ounce cup of typical Japanese sencha brewed at 80°C for 2 minutes delivers roughly 50-100 mg EGCG. Matcha delivers substantially more because the whole leaf is consumed — a typical 2-gram serving of ceremonial-grade matcha delivers approximately 130-180 mg EGCG. Loose-leaf gyokuro is intermediate. Tea-bag green tea is typically lower per serving.
For practical guidance:
- 1 cup/day — pleasant beverage, hydration, modest antioxidant signal, well below any safety concern
- 3-5 cups/day — the documented "effect zone" in epidemiologic cohorts. Reproducible improvements in oxidative stress markers, LDL oxidation resistance, blood pressure, and HDL/LDL ratio. Caffeine load of 90-250 mg per day, which is well-tolerated by most caffeine-naive adults.
- 6-10 cups/day — the upper Japanese consumption range. Larger antioxidant signal, but caffeine load may approach 300-500 mg/day. Fluoride load also begins to deserve attention (tea is one of the highest fluoride foods in the typical diet).
- Concentrated EGCG capsules >800 mg/day — exceeds EFSA safety limit, real idiosyncratic hepatotoxicity risk, not recommended.
The Dose-Toxicity Inversion (Pro-Oxidant Behavior)
At physiologic concentrations (the low micromolar range achieved by brewed tea), EGCG behaves as an antioxidant through the mechanisms described above. At supraphysiologic concentrations (high micromolar to millimolar, achievable only through concentrated extract supplementation), EGCG inverts to a pro-oxidant.
The chemistry behind the inversion involves EGCG autoxidation. In aqueous solution at neutral pH, EGCG slowly oxidizes by losing hydrogens to molecular oxygen, generating hydrogen peroxide and EGCG quinone intermediates as byproducts. At low EGCG concentrations the hydrogen peroxide is rapidly neutralized by cellular catalase and glutathione peroxidase. At high concentrations, hydrogen peroxide generation outpaces the cell's ability to neutralize it, and the result is oxidative stress driven by the supposed antioxidant.
EGCG quinones are also electrophilic and can covalently modify protein thiols, including critical cellular machinery like glutathione, glutathione S-transferase, and various mitochondrial proteins. The net effect of high-dose EGCG exposure in cell culture and in animal models is mitochondrial dysfunction, glutathione depletion, hepatocyte apoptosis, and acute hepatocellular injury — the opposite of the antioxidant effect at low dose.
This inversion is the underlying mechanism behind the green tea extract hepatotoxicity case series. Concentrated EGCG capsules taken on an empty stomach push plasma EGCG concentrations into the pro-oxidant range, particularly when the individual carries genetic variants that reduce hepatic EGCG conjugation or clearance. The brewed beverage essentially never reaches these concentrations.
Hepatotoxicity and the EFSA 800 mg Limit
The published literature on green tea extract hepatotoxicity now includes more than 100 case reports of acute hepatocellular injury attributed to concentrated EGCG supplements, with onset typically 2-12 weeks after starting the product. Liver injury patterns are typically hepatocellular (elevated ALT and AST) rather than cholestatic, with R-ratios >5. Histology when biopsy is performed shows hepatocyte necrosis with variable inflammatory infiltrate.
The Mazzanti case series (2009 and 2015 updates) catalogued the European pharmacovigilance data and identified key risk factors:
- Concentrated EGCG extracts (typically 300+ mg EGCG per capsule)
- Taking the supplement on an empty stomach (which substantially increases peak plasma EGCG)
- Multiple-times-daily dosing pushing total EGCG above 800 mg/day
- Concurrent use of other potentially hepatotoxic drugs or supplements
- Possible genetic susceptibility (HLA-B*35:01 has been associated with green tea extract DILI in one cohort)
The European Food Safety Authority issued a scientific opinion in 2018 recommending an upper limit of 800 mg EGCG per day for food supplements, with mandatory hepatic safety labeling. The opinion explicitly distinguished concentrated extracts from the brewed beverage and from green-tea-flavored foods (which carry vastly lower EGCG doses per serving and have an unbroken human safety record).
The practical guidance is clear: drink the tea, do not take the high-dose extract capsule unless under specific medical supervision (for example, certain oncology adjunct protocols use concentrated EGCG, but those are monitored settings).
Concentrated Supplement Versus Brewed Beverage
The difference between brewed green tea and concentrated EGCG capsules is not just a matter of dose, but of pharmacokinetics, matrix protection, and risk-benefit profile. A summary comparison:
- Total EGCG per serving — brewed cup: 50-100 mg. Concentrated capsule: 300-700 mg.
- Time to peak plasma EGCG — brewed cup with food: slow, modest peak. Capsule on empty stomach: rapid, high peak.
- Co-delivered compounds — brewed cup delivers EGCG with caffeine, L-theanine, EC, EGC, ECG, and minor compounds in natural ratios. Capsule delivers isolated EGCG with no protective matrix.
- Caffeine dose — brewed cup: 30-50 mg. Capsule: usually decaffeinated for higher EGCG concentration, removing the protective methylxanthine context.
- Documented hepatotoxicity risk — brewed beverage: essentially zero, no causally implicated case in the published literature over decades of high-volume consumption. Capsule: real but rare idiosyncratic risk.
- Pleasure / adherence — brewed beverage: high, sustainable for decades. Capsule: low, often discontinued.
The site-wide position is that green tea is a beverage, not a supplement. The benefits documented in epidemiologic cohorts came from drinking tea, not from taking pills. The dose-toxicity inversion at high EGCG concentrations is a real concern that does not apply to the brewed beverage at any reasonable consumption level.
Drug Interactions and Cautions
- Iron supplements and iron-rich meals — separate tea from iron intake by at least 1-2 hours to avoid catechin-iron chelation reducing iron absorption
- Anticoagulants (warfarin) — green tea contains vitamin K (modest amount), and very high-volume consumption has been reported to reduce INR in patients on warfarin. Habitual consumption is fine; large abrupt changes in tea intake should prompt INR monitoring.
- Bortezomib — EGCG directly binds and inactivates bortezomib (a proteasome inhibitor used in multiple myeloma), and patients on bortezomib should avoid green tea extract entirely. Brewed tea consumption is uncertain but typically avoided during active bortezomib treatment.
- Beta-blockers, atorvastatin, simvastatin — green tea may modestly reduce absorption via P-glycoprotein modulation. Separation by 1-2 hours is prudent.
- Caffeine-sensitive individuals — the caffeine load of 5-10 cups per day is real (250-500 mg) and can produce insomnia, tachyarrhythmia, anxiety, GERD, or pregnancy concerns at the high end
- Pregnancy — 1-3 cups per day appears safe. The folate-antagonist concern for EGCG raised by some animal data has not been confirmed in human pregnancy cohorts. Concentrated EGCG extract should be avoided in pregnancy.
- Fluoride exposure — tea leaves accumulate fluoride from soil, and brewed tea contributes meaningful fluoride to total daily intake. Heavy users (more than 6-8 cups daily of mature-leaf cheaper grades) have rare case reports of skeletal fluorosis. Higher-grade young-leaf teas (sencha, gyokuro, matcha) generally have lower fluoride than mature-leaf cheaper grades and brick tea.
Key Research Papers
- Higdon JV, Frei B (2003). Tea catechins and polyphenols: health effects, metabolism, and antioxidant functions. Critical Reviews in Food Science and Nutrition. — PubMed
- Yang CS et al. (2009). Cancer prevention by tea: animal studies, molecular mechanisms and human relevance. Nature Reviews Cancer. — PubMed
- Mazzanti G et al. (2009, 2015). Hepatotoxicity from green tea: a review of the literature and two unpublished cases. European Journal of Clinical Pharmacology. — PubMed
- EFSA Panel on Food Additives and Nutrient Sources (2018). Scientific opinion on the safety of green tea catechins. EFSA Journal. — PubMed
- Na HK, Surh YJ (2008). Modulation of Nrf2-mediated antioxidant and detoxifying enzyme induction by the green tea polyphenol EGCG. Food and Chemical Toxicology. — PubMed
- Lambert JD, Elias RJ (2010). The antioxidant and pro-oxidant activities of green tea polyphenols: a role in cancer prevention. Archives of Biochemistry and Biophysics. — PubMed
- Hallberg L, Rossander L (1982). Effect of different drinks on the absorption of non-heme iron from composite meals. Human Nutrition: Applied Nutrition. — PubMed
- Lee MJ et al. (2002). Pharmacokinetics of tea catechins after ingestion of green tea and (-)-epigallocatechin-3-gallate by humans. Cancer Epidemiology, Biomarkers and Prevention. — PubMed
- Sang S et al. (2011). The chemistry and biotransformation of tea constituents. Pharmacological Research. — PubMed
- Shen CL et al. (2009). Green tea and bone metabolism. Nutrition Research. — PubMed
- Hodgson AB et al. (2013). The metabolic and performance effects of caffeine compared to coffee during endurance exercise. PLoS One. — PubMed
- Hsu CH et al. (2008). Effect of green tea extract on obese women: a randomized, double-blind, placebo-controlled clinical trial. Clinical Nutrition. — PubMed
PubMed Topic Searches
- PubMed: EGCG and Nrf2 antioxidant response
- PubMed: EGCG pharmacokinetics
- PubMed: Green tea extract hepatotoxicity
- PubMed: Catechin iron chelation
- PubMed: EGCG pro-oxidant behavior
Connections
- Green Tea Overview
- Green Tea Benefits Hub
- Metabolism & Fat Oxidation
- L-Theanine & Calm Focus
- Brewing Time & Temperature
- L-Theanine
- Vitamin C
- Vitamin E
- Iron (Catechin Interaction)
- Selenium (Glutathione Peroxidase Cofactor)
- All Remedies
- Cardiology
- Hepatology
- All Food