Coffee for Cognitive Performance
Caffeine is the most widely consumed psychoactive substance on earth and the cognitive-performance effect is its main reason for being. The molecular mechanism is well mapped — competitive antagonism at the adenosine A1 and A2A receptors prevents the buildup of adenosine that drives sleep pressure across waking hours. Within roughly 30-60 minutes of intake, reaction time shortens, vigilance improves, sustained attention extends, and subjective alertness rises. Above 400-600 mg in a single dose the dose-response inverts — reaction time degrades from over-arousal, and anxiety, tremor, and palpitations dominate the experience. Across the population, CYP1A2 polymorphisms split coffee drinkers into fast metabolizers (caffeine half-life ~2-3 hours) and slow metabolizers (~6-10 hours), explaining why the same evening cup that lets one person sleep keeps another awake until 3 AM. This page maps the acute alertness pharmacology, the chronic tolerance and withdrawal cycle, and the longer-arc evidence for protection against Parkinson's and Alzheimer's disease.
Interactive Visualization Caffeine, Adenosine & Why Coffee Stops Working Caffeine doesn’t give you energy — it blocks the tiredness signal while adenosine keeps piling up behind the blockade. Move your coffee to 2 p.m. and watch your deep sleep vanish. Launch →
Table of Contents
- The Adenosine Receptor Mechanism
- Dose-Response and the Inverted U
- Pharmacokinetics: Absorption, Half-Life, Metabolism
- CYP1A2 Polymorphisms — Fast vs Slow Metabolizers
- Specific Cognitive Domains Affected
- Tolerance Development Over Days to Weeks
- Withdrawal Headache and Rebound
- Long-Term Effect: Parkinson's Disease Risk Reduction
- Long-Term Effect: Alzheimer's and Dementia
- CGA-Mediated Cognitive Effects (Independent of Caffeine)
- Caffeine in Exercise and Ergogenic Performance
- Sleep Considerations and Caffeine Half-Life Math
- Key Research Papers
- Connections
- Featured Videos
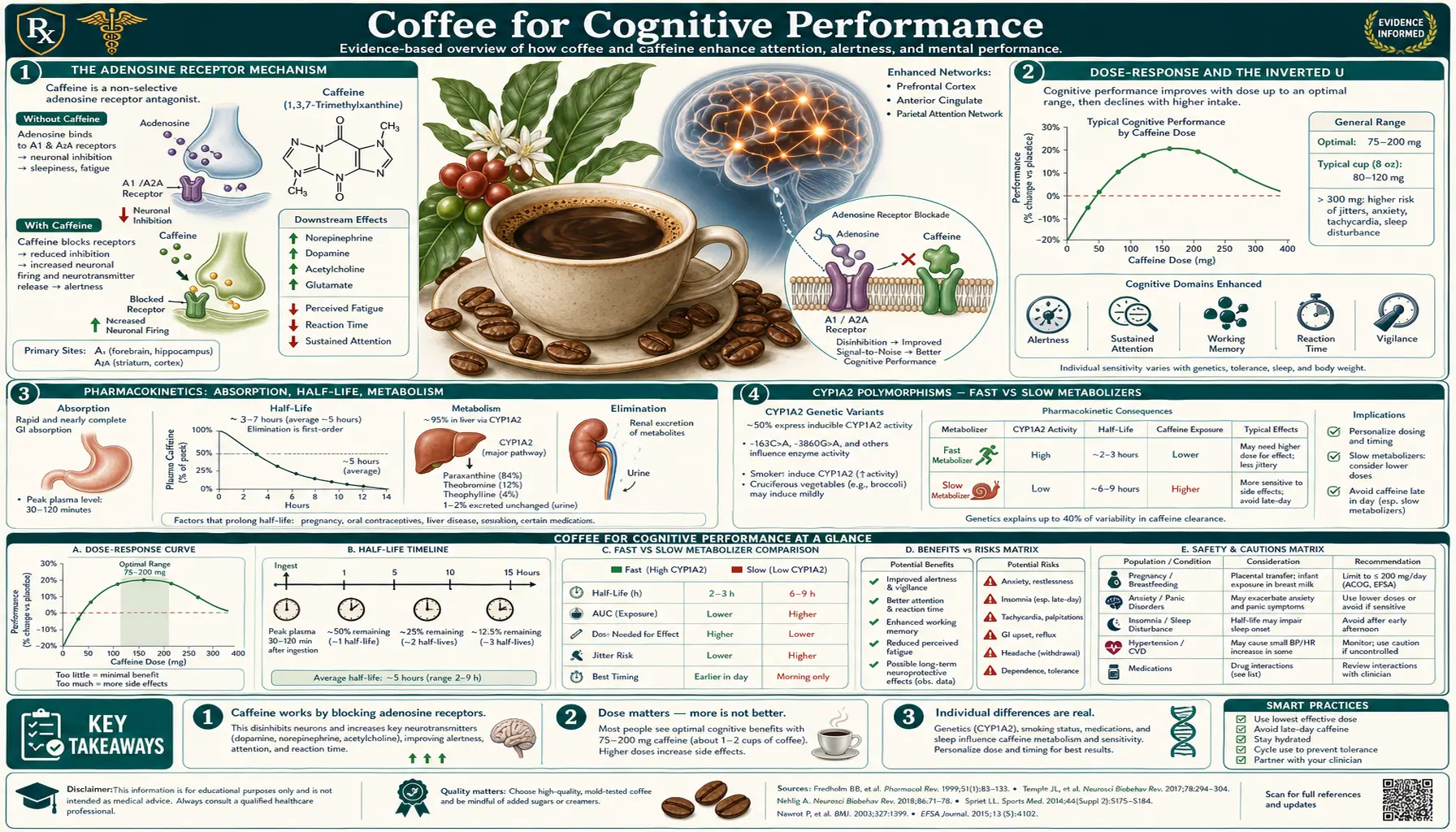
The Adenosine Receptor Mechanism
Adenosine is a small purine nucleoside that accumulates extracellularly during waking hours as a byproduct of ATP turnover in the brain — effectively a chemical record of how long the neurons have been working. Adenosine binds to four G-protein-coupled receptor subtypes (A1, A2A, A2B, A3); the A1 and A2A subtypes are the relevant ones for sleep-wake regulation. A1 receptors are widely distributed and generally inhibitory (Gi-coupled, reduce neuronal firing); A2A receptors concentrate in basal ganglia and the basal forebrain and are excitatory (Gs-coupled) but their net effect via downstream circuits is to promote sleep and reduce arousal.
Caffeine is a competitive antagonist at both A1 and A2A receptors, with binding affinity in the high-nanomolar to low-micromolar range — well within the plasma concentration achieved by a single normal cup of coffee (5-10 mg/L caffeine = 25-50 micromolar). At realistic intake the A2A occupancy at peak plasma concentration is approximately 50%.
The functional consequence: caffeine does not produce alertness by adding a positive stimulant signal. It produces apparent alertness by removing an inhibitory signal — the adenosine-driven brake on neuronal firing. This is a clinically important distinction. Caffeine's effect is largest in subjects with high adenosine pressure (sleep-deprived, late in the day, post-meal) and smallest in well-rested subjects in the morning. The classic finding that "caffeine restores performance to baseline in sleep-deprived subjects but barely improves it in rested ones" falls out directly from this mechanism.
Two secondary mechanisms contribute modestly. Caffeine inhibits phosphodiesterase weakly at supraphysiologic concentrations (the basis of caffeine's bronchodilator action, but irrelevant at coffee-drinking doses). Caffeine triggers modest catecholamine release (epinephrine and norepinephrine), contributing to the cardiovascular and tremor effects but not centrally to the cognitive effect.
Dose-Response and the Inverted U
The cognitive effect of caffeine follows an inverted-U dose-response. Reasonably tight numbers from the controlled-trial literature in caffeine-tolerant adults:
- 50-100 mg (half cup of drip): subjective alertness improvement, modest reaction-time improvement, no consistent vigilance change in laboratory tasks
- 100-200 mg (one normal cup): reliable reaction-time improvement of 4-7% on simple visual tasks, vigilance improvement during sustained-attention tasks of 30-90 minutes, modest working-memory improvement
- 200-400 mg (2-3 cups within an hour, or a Starbucks grande): larger reaction-time and vigilance effects, peak subjective alertness, mood improvement in moderate sleep deprivation
- 400-600 mg: vigilance still elevated but reaction-time benefit begins to plateau and reverse for complex tasks; anxiety begins to emerge in sensitive individuals
- 600-1000 mg: tremor, palpitations, anxiety dominate; cognitive performance on tasks requiring fine motor control degrades; subjective experience often becomes unpleasant
- Above 1000 mg in a single dose: clinically significant caffeine intoxication (DSM-5 criterion); arrhythmia, severe anxiety, gastrointestinal distress
- Above 5000 mg (rare, requires concentrated caffeine powder): potentially fatal due to seizure and ventricular arrhythmia
The FDA, EFSA, and Health Canada converge on roughly 400 mg/day for healthy adults as the upper bound of routinely safe daily intake, with 200 mg/day for pregnant women per ACOG. These limits reflect chronic safety rather than acute optimal performance — the optimum acute cognitive dose for most adults is in the 100-300 mg range, well below the chronic ceiling.
The inverted-U has clinical implications. Heavy coffee drinkers who push past 400 mg/day in pursuit of more alertness often find they get less — the marginal cup makes them jittery rather than sharper. The optimal-dose problem is also state-dependent: a sleep-deprived shift worker may need 200-300 mg to reach the same plateau that 100 mg achieves in a rested subject.
Pharmacokinetics: Absorption, Half-Life, Metabolism
Caffeine's pharmacokinetics are clean and well characterized:
- Absorption — rapid and essentially complete from the gastrointestinal tract. Peak plasma concentration at 30-90 minutes after oral intake, with substantial inter-individual variation in time-to-peak driven by gastric emptying and meal effects. Concurrent food slows absorption modestly but does not change total absorbed dose.
- Distribution — freely crosses the blood-brain barrier and the placenta. Volume of distribution roughly 0.5 L/kg (similar to total body water). No tissue accumulation with chronic intake.
- Half-life — population mean approximately 5 hours in healthy adults, range 2-10 hours driven primarily by CYP1A2 activity (next section). Half-life is shortened by smoking (~2 hours, smokers metabolize caffeine roughly 2x faster than non-smokers) and lengthened by pregnancy (third trimester 10-12 hours), liver disease, oral contraceptives, and several CYP1A2-inhibitor medications including ciprofloxacin, fluvoxamine, and cimetidine.
- Metabolism — 95% hepatic via CYP1A2, with the remainder via CYP2A6 and CYP3A4. The three primary metabolites are paraxanthine (84% of metabolism, the dominant metabolite and carrier of most chronic effects), theobromine (12%), and theophylline (4%). Paraxanthine has its own bioactivity profile — somewhat less psychoactive than caffeine but with adenosine antagonism preserved.
- Excretion — primarily urinary as paraxanthine and its further metabolites. Less than 3% appears in urine as unchanged caffeine.
The practical half-life numbers translate to: a 200 mg dose at 8 AM leaves roughly 100 mg circulating at 1 PM, 50 mg at 6 PM, and 25 mg at 11 PM in an average-metabolism adult. The sleep-relevant question is what blood concentration of caffeine at bedtime degrades sleep architecture — the answer from polysomnography studies is that even 100-200 mg of residual caffeine at bedtime measurably reduces deep slow-wave sleep and prolongs sleep onset latency, even when the subjects report feeling unaffected.
CYP1A2 Polymorphisms — Fast vs Slow Metabolizers
CYP1A2 activity in adults varies roughly 40-fold across the population — the largest known variation for any drug-metabolizing enzyme in routine human use. The variation is driven by a single common polymorphism in the CYP1A2 gene, rs762551 (also called CYP1A2*1F when the variant allele is in the *1F haplotype):
- AA genotype (~40-45% of European-ancestry population) — fast metabolizer. CYP1A2 is highly inducible. With habitual coffee or tobacco exposure, enzyme activity rises further and caffeine half-life shortens to 2-3 hours. The same dose "works" for a shorter time. Fast metabolizers can typically tolerate an evening cup without sleep disturbance because the caffeine has cleared by bedtime.
- AC and CC genotypes (~55-60%) — slow metabolizer. CYP1A2 has low baseline activity and limited inducibility. Caffeine half-life can reach 6-10 hours. The morning cup is still circulating at clinically meaningful concentration in the evening. Slow metabolizers often report "coffee makes me too wired" or "keeps me up all night even from a morning cup," and they have measurably more anxiety, jitteriness, and sleep disruption per dose.
The clinical implications go beyond personal coffee preference. A landmark series of studies (Cornelis et al., Palatini et al., Caldeira et al.) found that the CYP1A2 genotype interacts with coffee intake to modify cardiovascular risk:
- In fast metabolizers (AA), increasing coffee intake is associated with progressively lower risk of myocardial infarction and lower blood pressure
- In slow metabolizers (AC/CC), increasing coffee intake above ~2 cups/day is associated with higher risk of myocardial infarction and higher blood pressure
The proposed mechanism is that slow metabolizers experience prolonged elevated caffeine levels with each cup, producing sustained sympathetic activation that fast metabolizers escape. This is the same finding as our cardiovascular page covers in more detail. The CYP1A2 test is commercially available through 23andMe and most direct-to-consumer SNP services; the rs762551 result can be requested explicitly from any clinical genotyping service. For people whose coffee experience strongly resembles the slow-metabolizer phenotype (jittery, prolonged effect, sleep disruption from morning intake), the genetic confirmation is rarely needed — the phenotype is unambiguous.
Specific Cognitive Domains Affected
The McLellan, Caldwell, and Lieberman 2016 review and the Smith and Lieberman 2002 review converge on a fairly consistent map of which cognitive functions caffeine improves and which it does not:
- Vigilance / sustained attention — the most robust caffeine effect. Caffeine measurably improves performance on tasks lasting 30+ minutes requiring continuous monitoring (radar operators, air traffic control simulators, the Mackworth Clock Test). Effect size is large in sleep-deprived subjects and modest but reliable in rested ones.
- Simple reaction time — consistent 4-8% improvement at typical doses, larger in fatigued states.
- Choice reaction time — smaller benefit than simple reaction time; the additional decision step is less caffeine-responsive than the motor-response speed.
- Working memory — modest improvement on the n-back task and digit span at low-to-moderate doses; declines at high doses due to over-arousal interfering with the cognitive control needed for working memory.
- Executive function / cognitive flexibility — mixed results; some tasks improve, others (notably set-shifting under high cognitive load) can degrade.
- Long-term memory consolidation — emerging evidence (notably Borota et al. 2014) suggests caffeine taken after learning may enhance memory consolidation. The effect is small but reproducible in a few labs.
- Mood — consistent acute mood improvement in regular users (driven partly by reversal of overnight withdrawal); modest mood improvement in non-users. Decreases anger and depression scores on standardized scales acutely.
- Anxiety — dose-dependent. Mild reduction in some at low doses; clinically meaningful increase in some sensitive individuals at moderate doses. Caffeine challenge in panic-disorder patients reliably triggers panic attacks at doses (300-450 mg) that do not affect controls — this is a recognized provocation test.
- Creativity / divergent thinking — little evidence for enhancement and some evidence (Zabelina & Silvia 2020) of small impairment on tasks requiring flexible idea generation, possibly because the increased focus narrows attention.
The summary picture: caffeine reliably improves vigilance, reaction time, and convergent task performance, particularly in fatigued or sleep-deprived states. It is less reliable for executive function and creativity, and counter-productive at high doses for tasks requiring fine motor control or flexible thinking.
Tolerance Development Over Days to Weeks
Daily caffeine intake produces partial tolerance to its cognitive effects over 7-14 days. The mechanism is upregulation of adenosine receptors (more receptors per cell, requiring a higher caffeine dose to occupy the same fraction) plus modest sensitization of A2A signaling.
The tolerance is partial and selective:
- Subjective alertness — substantial tolerance. After two weeks of regular daily intake, the "feeling" of the morning cup is largely a feeling of returning to baseline rather than rising above it.
- Vigilance / reaction time — partial tolerance, but laboratory studies still show measurable improvement vs the same subject in caffeine-withdrawn state.
- Cardiovascular pressor effect — substantial tolerance. The 5-10 mmHg blood pressure rise after caffeine in naive subjects shrinks to 1-2 mmHg in chronic daily users.
- Diuresis — substantial tolerance. Caffeine's mild diuretic effect is largely abolished in regular daily drinkers.
- Sleep disruption — incomplete tolerance. Even chronic daily drinkers show measurable sleep architecture disturbance from evening caffeine, although they often subjectively report no problem. This is one of the few caffeine effects that does not fully habituate.
The tolerance has interesting strategic implications. Athletes and shift workers who want maximum acute performance benefit from caffeine sometimes withdraw for 5-7 days before a competition or critical shift, then dose acutely on the target day. This recovers a substantial fraction of the "naive responder" effect at the cost of a withdrawal period.
Conversely, daily coffee drinkers who try to use coffee acutely for the alertness benefit during normal daily life are mostly running on the partial-tolerance plateau. They feel mostly normal with their morning cup and lousy without it — which is consistent with the picture that for chronic users, daily caffeine is mostly preventing withdrawal symptoms and providing a modest residual alerting effect on top.
Withdrawal Headache and Rebound
Caffeine withdrawal is a recognized DSM-5 diagnosis. Symptoms begin 12-24 hours after the last dose, peak at 24-48 hours, and resolve over 2-9 days. The cardinal symptom is headache — a bilateral throbbing or pulsing headache, often unilateral or worse on one side, typically beginning at the temples or in the frontal region.
The mechanism is rebound adenosine sensitivity. During chronic caffeine intake, adenosine receptors are upregulated; when caffeine is removed, the endogenous adenosine occupies the now-abundant receptors with no antagonist to compete, producing cerebral vasodilation (adenosine is a cerebral vasodilator), reduced neuronal firing, and the headache experience. Caffeine restores antagonism and the headache resolves within 30-60 minutes — the well-known "coffee cures my headache" experience.
Other withdrawal symptoms: fatigue, reduced alertness, difficulty concentrating, depressed mood, irritability, flu-like sensations, mild nausea, and (rarely) muscle aches. The full constellation is reported by roughly 50% of people withdrawing from 200+ mg/day after 5+ days of regular intake. Withdrawal from very low doses (one cup of weak tea daily) typically produces no clinically significant symptoms.
Clinical relevance:
- Pre-operative fasting — patients undergoing surgery who normally drink several cups of coffee daily are at risk for postoperative caffeine-withdrawal headache. Many anesthesia services now permit a single small caffeinated drink with the preoperative sip of water, or use caffeine sodium benzoate IV to prevent withdrawal.
- Hospitalization — admitted patients often have their coffee abruptly stopped, contributing to apparent "hospital headache." This is now widely recognized and is usually managed by allowing coffee or providing caffeine in the medication list.
- Migraine — chronic caffeine use complicates migraine management. Caffeine can abort an acute migraine (the basis of caffeine-containing analgesics like Excedrin) but daily caffeine use can also drive medication-overuse headache that resembles chronic migraine. Migraineurs with daily coffee intake should taper rather than abruptly stop.
- Tapering strategy — if discontinuation is the goal, a roughly 25-50% reduction every 2-3 days over 1-2 weeks largely avoids the headache. Cold-turkey discontinuation produces the full syndrome.
Long-Term Effect: Parkinson's Disease Risk Reduction
One of the strongest and most consistent epidemiologic associations between any dietary factor and any neurodegenerative disease is the inverse relationship between coffee consumption and Parkinson's disease incidence. The Honolulu Heart Program (Ross et al. 2000) was the first large prospective cohort to demonstrate this clearly, finding that men in the highest coffee-consumption quartile had approximately one-third the Parkinson's disease incidence of non-drinkers over 30 years of follow-up.
Subsequent meta-analyses (Hernan et al. 2002, Liu et al. 2012, Costa et al. 2010) consistently show a 20-30% relative risk reduction per 3-cup daily intake, with the dose-response curve flattening above 3-4 cups. The effect is present in both men and women in most studies, though some show a sex difference modulated by hormonal status (women on hormone replacement therapy show attenuated protection, suggesting an estrogen-caffeine interaction).
The proposed mechanism is A2A receptor antagonism in the striatum. The striatum contains dense A2A receptor expression on the indirect-pathway medium spiny neurons. Adenosine A2A signaling promotes activity in this indirect pathway, which is overactive in Parkinson's disease (the indirect pathway lesion contributes to bradykinesia and rigidity). Caffeine's A2A antagonism dampens this overactivity. Istradefylline, a selective A2A antagonist approved by the FDA in 2019 as adjunct therapy for Parkinson's disease, validates the pharmacologic concept at therapeutic doses.
A few important caveats:
- The protective effect is largely caffeine-specific. Decaffeinated coffee shows much weaker or absent protection in most studies (although a few find some residual effect, possibly mediated by EHT, an organic compound also found in coffee).
- Reverse causation is a concern — pre-clinical Parkinson's disease can produce loss of pleasure in coffee, so people who develop Parkinson's may reduce coffee intake years before diagnosis. Studies with very long lead-time follow-up (15-30 years pre-diagnosis exposure assessment) largely control for this and still show the protective effect.
- The effect is on incidence, not on disease progression. Coffee consumption does not appear to slow Parkinson's disease progression in established disease.
- The therapeutic implication is not "drink more coffee to prevent Parkinson's." The risk reduction is modest in absolute terms (Parkinson's lifetime risk is ~1.5%, so even a 30% relative risk reduction is a 0.5% absolute reduction) and not large enough on its own to motivate intake.
See our Parkinson's Disease page for the full clinical picture.
Long-Term Effect: Alzheimer's and Dementia
The coffee-Alzheimer's association is real but weaker and noisier than the Parkinson's association. Eskelinen and Kivipelto's 2009 CAIDE cohort study in Finland found that midlife (mean age 50) coffee consumption of 3-5 cups/day was associated with approximately 65% reduced dementia risk and 64% reduced Alzheimer's risk at 21-year follow-up, compared to less than 2 cups/day. The effect was U-shaped — very heavy drinkers (more than 5 cups) had less protection than the 3-5 cup group.
Other large cohorts (CARDIA, Rotterdam, Three-City) have produced mixed results, with some showing protection and others showing no significant association. The meta-analyses pool to a small protective effect (roughly 15-20% relative risk reduction) that is statistically significant but modest in magnitude.
Proposed mechanisms (none individually proven):
- A2A receptor antagonism in hippocampus and cortex, reducing tau pathology in mouse models
- Chlorogenic acid and ferulic acid metabolites crossing the blood-brain barrier and reducing oxidative stress in vulnerable neurons
- Insulin sensitivity improvement reducing the metabolic-syndrome contribution to dementia risk (type 3 diabetes hypothesis)
- Cerebrovascular effects — coffee's modest blood pressure effects may protect against vascular cognitive impairment
- EHT (eicosanoyl-5-hydroxytryptamide) — a coffee constituent shown in mouse models to reduce alpha-synuclein and tau pathology synergistically with caffeine
Practical conclusion: the dementia-protective evidence is suggestive but not as compelling as the Parkinson's evidence. As with Parkinson's, the absolute risk reduction is modest and not on its own a sufficient reason to start drinking coffee. Established daily coffee drinkers may take some reassurance that their habit is not harming and is probably mildly helpful for long-term cognitive health.
CGA-Mediated Cognitive Effects (Independent of Caffeine)
The acute cognitive effects of coffee that survive decaffeination are smaller than the caffeine-driven effects but real. Studies of decaffeinated coffee and green-coffee-extract supplements show:
- Modest improvement in vigilance and reaction time at high CGA doses (300-1000 mg), roughly 30-50% of the caffeine-driven effect
- Improvement in cerebral blood flow measured by transcranial Doppler — CGAs and their metabolites are mild cerebral vasodilators
- Some evidence for improvement on mental fatigue measures during prolonged cognitive tasks, possibly via cerebral blood flow and antioxidant mechanisms
- The chronic cognitive-decline-protective effects of coffee on Parkinson's and Alzheimer's are partially preserved in decaf studies (especially for Alzheimer's; less so for Parkinson's), suggesting CGAs contribute to the long-term protective effect
The CGA-mediated cognitive effects are explored further in the Polyphenols and Chlorogenic Acid deep-dive and in the Decaf vs Caffeinated page.
Caffeine in Exercise and Ergogenic Performance
Caffeine is one of the most thoroughly validated ergogenic aids in sports science. The 2021 International Society of Sports Nutrition position stand on caffeine and exercise performance summarizes the evidence:
- Endurance performance (events 5-60+ minutes): 2-6% improvement at 3-6 mg/kg body weight, taken 60 minutes before competition
- Short-duration high-intensity performance: modest 2-5% improvement, more variable than endurance benefit
- Muscular strength and power: small but reproducible 2-7% improvement in resistance-exercise studies
- Reaction time and accuracy in team sports: improvement in vigilance and decision-making translates to sport-specific performance gains in football, basketball, and tennis trials
The standard dose for performance is 3-6 mg/kg of caffeine 60 minutes pre-exercise. For a 70 kg adult that is 210-420 mg, comparable to 2-4 cups of strong coffee or one large pre-workout supplement. Higher doses (8-9 mg/kg) do not provide additional benefit and increase side effects.
The CGA contribution to ergogenic performance is small. Most of the exercise-related coffee benefit is caffeine-driven. Decaffeinated coffee in placebo-controlled trials does not produce the same performance gains.
Caffeine's ergogenic effect has been formally removed from the WADA prohibited list (since 2004), although it remains on the monitoring program. In NCAA athletes, urinary concentrations above 15 mcg/mL constitute a positive test — a threshold typically requiring 800+ mg of caffeine in 2-3 hours pre-competition.
Sleep Considerations and Caffeine Half-Life Math
Caffeine measurably disrupts sleep at lower doses and later cutoff times than most users appreciate. The Drake et al. 2013 study found that 400 mg caffeine taken 6 hours before bedtime reduced total sleep time by 1 hour and significantly disrupted sleep architecture, even though subjects reported no awareness of the effect. The effect on objectively measured sleep was nearly as large at the 6-hour pre-sleep timing as at the 0-hour (bedtime) timing.
The practical math: for an average-metabolism adult with a 10 PM bedtime and a desired residual caffeine load under 50 mg at bedtime, the last cup of regular coffee should be no later than ~2 PM. For slow CYP1A2 metabolizers, the cutoff is closer to noon. Fast metabolizers tolerate later intake.
Practical adjustments:
- If you suspect coffee is degrading your sleep but cannot tell — try a 5-day caffeine washout and compare your morning energy. If you feel meaningfully better after washout, your evening caffeine is reaching the brain at sleep time even if subjective experience does not register it.
- For slow metabolizers: switch to decaf or yerba mate by 11 AM, drink only morning coffee, or simply cap daily intake at one early cup.
- For fast metabolizers: more flexibility but still avoid the last cup closer than 6 hours before bedtime if sleep quality matters.
- If you wake unrefreshed despite adequate hours in bed — deep slow-wave sleep is often the missing element, and residual caffeine selectively reduces deep sleep more than total sleep. Earlier cutoff is the cheapest intervention.
Caffeine and shift work has its own optimization literature; see Roach et al. for evidence-based caffeine strategies for night-shift workers.
Key Research Papers
- Fredholm BB et al. (1999). Actions of caffeine in the brain with special reference to factors that contribute to its widespread use. Pharmacological Reviews. — PubMed
- McLellan TM, Caldwell JA, Lieberman HR (2016). A review of caffeine's effects on cognitive, physical and occupational performance. Neuroscience & Biobehavioral Reviews. — PubMed
- Cornelis MC, El-Sohemy A et al. (2006). Coffee, CYP1A2 genotype, and risk of myocardial infarction. JAMA. — PubMed
- Ross GW et al. (2000). Association of coffee and caffeine intake with the risk of Parkinson disease. JAMA. — PubMed
- Eskelinen MH, Kivipelto M (2010). Caffeine as a protective factor in dementia and Alzheimer's disease. Journal of Alzheimer's Disease. — PubMed
- Drake C et al. (2013). Caffeine effects on sleep taken 0, 3, or 6 hours before going to bed. Journal of Clinical Sleep Medicine. — PubMed
- Juliano LM, Griffiths RR (2004). A critical review of caffeine withdrawal: empirical validation of symptoms and signs. Psychopharmacology. — PubMed
- Hernan MA et al. (2002). A meta-analysis of coffee drinking, cigarette smoking, and the risk of Parkinson's disease. Annals of Neurology. — PubMed
- Borota D et al. (2014). Post-study caffeine administration enhances memory consolidation in humans. Nature Neuroscience. — PubMed
- Guest NS et al. (2021). International Society of Sports Nutrition position stand: caffeine and exercise performance. JISSN. — PubMed
- Smith A (2002). Effects of caffeine on human behavior. Food and Chemical Toxicology. — PubMed
- Palatini P et al. (2009). CYP1A2 genotype modifies the association between coffee intake and the risk of hypertension. Journal of Hypertension. — PubMed
PubMed Topic Searches
- PubMed: Caffeine adenosine A2A cognition
- PubMed: CYP1A2 caffeine metabolism
- PubMed: Coffee Parkinson's cohorts
- PubMed: Caffeine working memory vigilance
- PubMed: Caffeine withdrawal headache
Connections
- Caffeine, Adenosine & Why Coffee Stops Working — interactive animation
- Coffee Benefits Hub (Food Science)
- Polyphenols and Chlorogenic Acid
- Bean Variety and Roast
- Decaf vs Caffeinated
- Coffee (Food Hub)
- Coffee Cardiovascular & Mortality (CYP1A2 Interaction)
- Parkinson's Disease
- Alzheimer's Disease
- Anxiety
- Insomnia
- Hypertension
- Green Tea (L-Theanine + Caffeine)
- L-Theanine
- Lab Tests
- All Foods