Uterine Prolapse
Uterine prolapse is the descent of the uterus and cervix into or beyond the vaginal canal due to failure of the pelvic floor support structures. It belongs to the broader spectrum of pelvic organ prolapse (POP), which encompasses herniation of the bladder (cystocele), rectum (rectocele), small bowel (enterocele), and vaginal vault into or through the vaginal walls. Approximately 50% of women who have had at least one vaginal delivery have some measurable degree of anatomical prolapse on examination, though most remain asymptomatic. Between 10 and 20% will seek treatment for bothersome symptoms, and the lifetime risk of undergoing at least one surgical correction is estimated at 12–19%. POP is significantly underreported because many women are embarrassed or assume symptoms are an inevitable part of aging. It affects sexual function, urinary and bowel habits, body image, and overall quality of life — yet responds well to both conservative and surgical treatment when addressed.
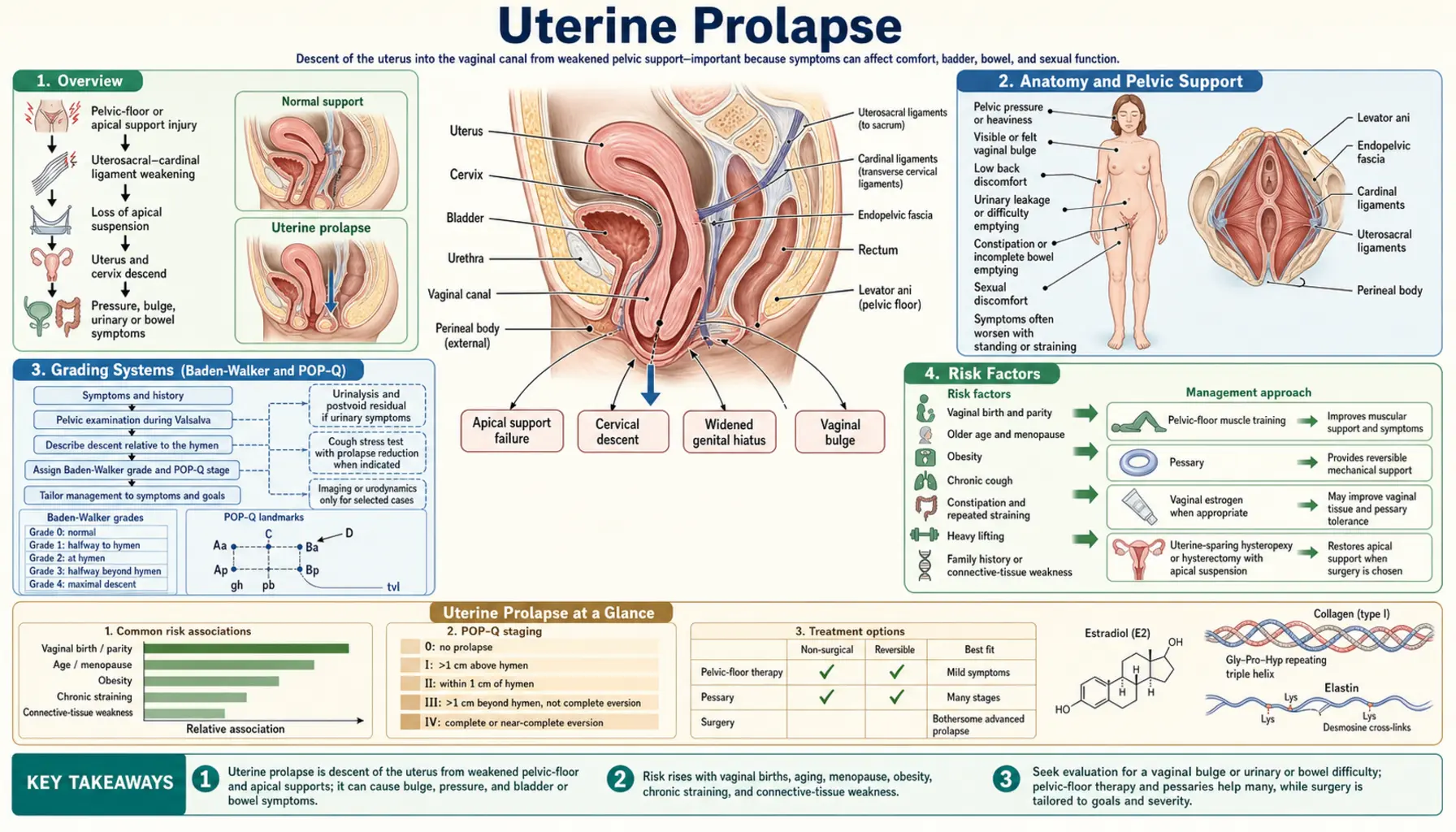
Table of Contents
- Overview
- Anatomy and Pelvic Support
- Grading Systems (Baden-Walker and POP-Q)
- Risk Factors
- Clinical Presentation and Three Compartments
- Diagnosis
- Pelvic Floor Physical Therapy
- Pessaries
- Surgical Options
- Sacrocolpopexy and Apical Repair
- References
- Featured Videos
1. Overview
Pelvic organ prolapse (POP) is a form of hernia in which one or more pelvic organs — the bladder, uterus, rectum, or small bowel — descend into or protrude through the vaginal canal because the supporting pelvic floor muscles, fascia, and ligaments have been weakened or damaged. Uterine prolapse specifically refers to the downward displacement of the uterus and cervix along the vaginal axis.
Population-based studies estimate that roughly 50% of women who have had at least one vaginal delivery have some degree of anatomical prolapse detectable on standardized pelvic examination, though many never develop significant symptoms. Symptomatic prolapse that prompts a clinical visit affects 10–20% of women over their lifetime, and an estimated 12–19% of women will ultimately require surgical repair. POP is the leading indication for hysterectomy in women over age 55 in the United States.
Despite its high prevalence, POP is chronically undertreated. Studies show that fewer than half of affected women bring symptoms to their physician, commonly citing embarrassment or a belief that nothing can be done. This silence leads to delayed diagnosis and prolonged impairment of quality of life — including sexual dysfunction, urinary and bowel symptoms, reduced physical activity, and negative body image. Early identification and a stepped-care approach, beginning with conservative pelvic floor rehabilitation, can dramatically improve outcomes with relatively low risk. Surgical repair, when indicated, offers durable relief for the majority of women.
2. Anatomy and Pelvic Support
The pelvic organs are held in position by an integrated system of muscular and connective-tissue support that DeLancey organized into three anatomical levels, each responsible for a distinct segment of the vagina and its adjacent organs.
- Level I (apical support): The uterosacral ligaments and cardinal (Mackenrodt's) ligaments suspend the vaginal apex and uterine cervix from the sacrum and lateral pelvic sidewalls. Failure at this level produces uterine prolapse or, after hysterectomy, vaginal vault prolapse.
- Level II (lateral/mid-vaginal support): Paravaginal attachments connect the lateral walls of the anterior vagina to the arcus tendineus fasciae pelvis (ATFP), a fibrous band running from the pubic symphysis to the ischial spine. Defects here allow the anterior vaginal wall and the overlying bladder to herniate inward, producing a cystocele.
- Level III (distal support): The distal vagina fuses directly with the perineal body and urogenital diaphragm. Damage at this level leads to perineal descent and distal rectocele.
The levator ani muscle group — comprising the pubococcygeus, iliococcygeus, and puborectalis — forms the muscular floor of the pelvis and provides active, dynamic support. Under normal resting conditions the levator plate is nearly horizontal, which allows intra-abdominal pressure increases (coughing, lifting) to compress the vagina against this muscular shelf rather than force organs downward through the genital hiatus. When the levator ani is damaged or denervated, the genital hiatus widens and the vaginal axis shifts toward vertical, placing the full force of intra-abdominal pressure directly on the connective tissue supports.
Estrogen plays a critical role in maintaining connective tissue elasticity and collagen synthesis within the pelvic ligaments and fasciae. Loss of estrogen at menopause accelerates collagen degradation and reduces the tensile strength of the uterosacral and cardinal ligaments, which is why symptomatic prolapse is most common in the postmenopausal decade.
3. Grading Systems (Baden-Walker and POP-Q)
Two staging systems are in common clinical use. The Baden-Walker halfway system is older and widely used in everyday clinical practice for its simplicity. The Pelvic Organ Prolapse Quantification (POP-Q) system, introduced in 1996 and subsequently adopted by the International Continence Society, provides standardized, reproducible measurements suitable for research and surgical outcome reporting.
Baden-Walker Halfway System
- Grade 0: No prolapse; normal support.
- Grade 1: The most distal portion of the prolapse descends halfway to the hymen.
- Grade 2: The prolapse reaches the hymenal ring.
- Grade 3: The prolapse extends halfway past the hymen.
- Grade 4: Maximum prolapse; complete eversion of the vaginal wall or procidentia.
POP-Q System
The POP-Q measures nine anatomical reference points relative to the hymen (negative values = above the hymen; positive values = beyond it). The six primary measurement points are: Aa and Ba (anterior compartment), C and D (apical compartment), and Ap and Bp (posterior compartment). Three additional measurements capture the genital hiatus (gh), perineal body (pb), and total vaginal length (tvl).
- Stage 0: No prolapse; all points above hymen by more than 1 cm.
- Stage I: Most distal point is more than 1 cm above the hymen.
- Stage II: Most distal point is within 1 cm proximal or distal to the hymenal plane.
- Stage III: Most distal point is more than 1 cm past the hymen but less than (tvl − 2) cm beyond it.
- Stage IV: Complete vaginal eversion; most distal point is at least (tvl − 2) cm beyond the hymen.
The POP-Q system also describes three anatomical compartments that are assessed separately: the anterior compartment (bladder/cystocele, measured at points Aa and Ba), the apical compartment (uterus or post-hysterectomy vaginal vault, measured at C and D), and the posterior compartment (rectum/rectocele or small bowel/enterocele, measured at Ap and Bp). A patient may have prolapse in one, two, or all three compartments simultaneously.
4. Risk Factors
POP is multifactorial. The major categories of risk include obstetric trauma, hormonal changes, chronically elevated intra-abdominal pressure, anatomical and genetic susceptibility, and age.
Obstetric Factors
- Vaginal delivery: The single strongest modifiable risk factor. Levator ani muscle avulsion injury — visible on pelvic MRI as a detachment of the pubococcygeus from its insertion on the pubic bone — occurs in 20–30% of vaginal deliveries and is strongly associated with subsequent prolapse.
- Operative vaginal delivery: Forceps delivery carries a 3–4 fold higher risk of levator avulsion than spontaneous vaginal delivery; vacuum extraction carries intermediate risk.
- Prolonged second stage of labor: Each additional hour in the second stage increases levator damage and pudendal nerve stretch injury.
- Fetal macrosomia: Birth weight above 4 kg is an independent risk factor.
- Parity: Risk increases cumulatively with each vaginal delivery.
Hormonal Factors
- Menopause: Estrogen deficiency reduces collagen synthesis and accelerates ligament degradation, making symptomatic prolapse far more common in the postmenopausal years even when the initial anatomical damage occurred decades earlier during childbirth.
- Surgical menopause: Bilateral oophorectomy before natural menopause leads to earlier onset of connective tissue changes.
Chronic Increased Intra-Abdominal Pressure
- Obesity: BMI above 30 approximately doubles the risk of POP by applying persistent downward load on pelvic floor structures.
- Chronic constipation and straining: Repeated Valsalva during defecation stretches pudendal nerve and perineal tissues over time.
- COPD and chronic cough: Forceful repeated coughing transmits intra-abdominal pressure spikes to the pelvic floor.
- Heavy repetitive lifting: Occupational lifting (nursing, farming, construction) is an independent risk factor in several cohort studies.
Anatomical and Genetic Factors
- Race and ethnicity: Caucasian and Hispanic women have significantly higher rates of symptomatic POP than African-American women, likely reflecting differences in levator ani muscle bulk and pelvic architecture. Asian women have intermediate risk.
- Family history: First-degree relatives of women with prolapse have a substantially elevated lifetime risk, suggesting heritable collagen and connective tissue traits.
- Connective tissue disorders: Marfan syndrome, Ehlers-Danlos syndrome (especially hypermobile type), and other heritable connective tissue disorders markedly increase prolapse risk and recurrence rates after repair.
- Prior hysterectomy: Removal of the uterus eliminates the apical anchoring provided by the uterosacral and cardinal ligaments, increasing long-term risk of vaginal vault prolapse by approximately 5-fold if apical suspension is not specifically addressed at the time of hysterectomy.
Age
Prevalence rises steeply with age. While anatomical prolapse is common in younger parous women, symptomatic prolapse requiring treatment is most prevalent in women in their 70s and 80s. The combination of cumulative connective tissue aging, post-menopausal estrogen loss, and years of gravitational loading converges to produce clinically significant descent in older women.
5. Clinical Presentation and Three Compartments
Symptoms of POP are closely tied to which compartment is affected and the degree of descent. The most sensitive indicator of clinically significant prolapse is the prolapse extending to or beyond the hymen (POP-Q Stage II or higher).
General Pelvic Symptoms
- Pelvic pressure or heaviness: The most common presenting symptom — a sensation of "something falling out" of the vagina, typically worsening with prolonged standing, walking, or physical activity and relieved by lying down.
- Vaginal bulge: A visible or palpable protrusion at the vaginal opening; pathognomonic of significant prolapse when the patient herself can see or feel it.
- Pelvic pain or low backache: Less specific; often attributed to the mechanical load on supporting ligaments.
Anterior Compartment (Cystocele)
Descent of the anterior vaginal wall carries the bladder base downward, distorting urethral and bladder geometry. Symptoms include:
- Stress urinary incontinence (leakage with coughing, sneezing, exercise)
- Urinary urgency and frequency (overactive bladder symptoms)
- Voiding difficulty — incomplete bladder emptying, hesitancy, need to change position or manually reduce the prolapse to initiate urination ("splinting" or "digitation")
- Recurrent urinary tract infections from chronic incomplete emptying
Apical and Uterine Prolapse
- Cervix visible at or protruding beyond the vaginal introitus
- Ulceration and keratinization of the exposed cervical epithelium from chronic friction and desiccation
- Dragging lower abdominal discomfort
Posterior Compartment (Rectocele and Enterocele)
Descent of the posterior vaginal wall allows the rectum (rectocele) or small bowel (enterocele) to herniate into the vaginal lumen. Symptoms include:
- Difficulty with defecation — straining, sense of incomplete evacuation
- Need to apply digital pressure to the posterior vaginal wall to empty the rectum ("posterior splinting" or manual digitation)
- Constipation, fecal urgency, or fecal incontinence in severe cases
Sexual Dysfunction
POP impairs sexual function through dyspareunia (pain with intercourse from mechanical distortion), reduced lubrication and arousal (from associated atrophic changes and psychosocial distress), and avoidance behaviors. Partners may perceive the vaginal bulge during intercourse.
Occult Stress Urinary Incontinence
Some women with large anterior prolapse paradoxically report no urine leakage because the prolapsed bladder kinks the urethra, creating a functional obstruction. When the prolapse is surgically corrected, this kinking is relieved and stress incontinence becomes apparent. A preoperative pessary reduction test — asking the patient to cough or strain with the prolapse manually reduced — unmasks occult incontinence in approximately 30–40% of women with Stage III or IV anterior prolapse, informing the decision to add a concurrent continence procedure.
6. Diagnosis
The diagnosis of POP is clinical, based on history and pelvic examination. No imaging is required for routine cases.
- Pelvic examination: Performed in the dorsal lithotomy position, first at rest and then with maximum Valsalva (bearing down). Each compartment is assessed separately using a Sims (half) speculum to retract the opposing wall. The posterior blade retracts the posterior wall to isolate the anterior compartment and vice versa. Standing examination is often superior for detecting posterior compartment prolapse.
- POP-Q staging: Recommended for documentation, surgical planning, and outcome comparison. Requires a ruler and the ability to identify the anatomical reference points reliably.
- Urodynamic studies: Indicated when significant urinary symptoms coexist with prolapse, particularly before surgical intervention, to differentiate stress incontinence from urgency incontinence and to detect occult incontinence after prolapse reduction.
- Defecography or dynamic MRI of the pelvic floor: Reserved for complex posterior compartment prolapse, suspected enterocele, obstructed defecation, or evaluation of failed prior posterior repair. MRI provides multicompartment visualization in a single study and can detect levator avulsion injuries.
- Renal ultrasound: Indicated in women with Stage III or IV anterior prolapse to screen for hydronephrosis from ureteral kinking by the prolapsed bladder base.
- Cystoscopy: Performed when concurrent bladder pathology is suspected or before mesh-augmented repair of the anterior compartment.
7. Pelvic Floor Physical Therapy
Pelvic floor physical therapy (PFPT) is the recommended first-line treatment for symptomatic POP Stage I through III. It is also used after surgical repair to optimize long-term support and prevent recurrence.
Core Technique: Pelvic Floor Muscle Training (PFMT / Kegel Exercises)
PFMT involves systematic strengthening of the levator ani and other pelvic floor muscles. Supervised PFMT by a trained pelvic floor physiotherapist is substantially more effective than unsupervised home exercise because many women cannot correctly identify their pelvic floor muscles without instruction, and up to 30% contract the wrong muscles (Valsalva or gluteal co-contraction) when given written instructions alone.
- A typical supervised protocol includes 3 sets of 10–15 contractions daily, progressing in duration (from 3-second holds to 10-second holds), intensity, and functional integration over 12–16 weeks.
- Endurance training (sustained contractions) and coordination training (quick-flicks for reflex closure during cough/sneeze) complement strength training.
- For women with hypertonicity or high-tone pelvic floor dysfunction, relaxation and down-training techniques are essential before strengthening.
- Functional integration includes pelvic floor co-contraction during squats, lifting, and transitions from sitting to standing.
Outcomes
The POPPY trial (Hagen et al., 2014) — the largest randomized controlled trial of PFMT for POP — demonstrated that individualized PFMT reduced prolapse symptom severity significantly compared to a control group, with benefit sustained at one year. Meta-analyses show PFMT reduces prolapse stage by at least one grade in 20–30% of women and meaningfully improves symptom severity scores and quality of life in 40–60% of participants.
Adjunct Modalities
- Biofeedback: Real-time visual or auditory feedback of pelvic floor EMG activity helps patients correctly isolate target muscles.
- Intravaginal electrical stimulation: Passive contraction stimulus useful for women with poor voluntary control or levator denervation.
- Manual therapy: Soft-tissue mobilization and myofascial release for scar tissue after obstetric trauma or prior surgery.
- Lifestyle modification: Weight loss, stool softeners/fiber to eliminate straining, timed voiding, and activity modification all reduce mechanical load on the pelvic floor and complement muscle training.
Postpartum pelvic floor rehabilitation — initiated as early as 6 weeks after vaginal delivery — is the most effective time to prevent progression from asymptomatic anatomical prolapse to symptomatic disease.
8. Pessaries
A pessary is a removable mechanical support device placed intravaginally to reduce prolapse, restore normal vaginal anatomy, and relieve symptoms. Pessaries are appropriate for women with symptomatic Stage II–IV prolapse who prefer non-surgical management, are medically unfit for surgery, or wish to preserve fertility and defer definitive repair.
Types and Fitting
- Ring pessary: The most commonly prescribed device; suitable for Stage II–III prolapse with adequate perineal support. Available in multiple sizes; can usually be self-managed by the patient (removed, cleaned, and reinserted at home).
- Gellhorn pessary: A rigid convex disc with a central stem; preferred for Stage III–IV prolapse and complete uterine procidentia. Requires office fitting and removal due to the stem design; most women cannot self-manage Gellhorn pessaries.
- Cube, donut, inflatable, and Shaatz pessaries: Alternative designs for specific anatomical situations (wide vaginal caliber, inadequate perineal body, failed ring/Gellhorn).
Fitting requires a trial of different sizes and types with assessment of comfort, ambulation, and voiding after placement. Approximately 20–30% of women cannot retain a pessary satisfactorily due to insufficient perineal support or vaginal anatomy not compatible with available devices.
Maintenance
- Self-removable pessaries (most ring types): Patient cleans device weekly with mild soap and water; re-examination every 3–6 months initially, then annually if stable.
- Non-removable pessaries (Gellhorn): Office visits every 3 months for removal, inspection, cleaning, and re-insertion.
Complications and Long-Term Use
- Vaginal discharge: Mucoid secretion is normal and expected; offensive odor suggests overgrowth of vaginal flora, managed by more frequent cleaning or periodic metronidazole gel.
- Vaginal erosion: Especially common with atrophic postmenopausal mucosa; local vaginal estrogen cream used prophylactically reduces erosion risk and improves tissue integrity.
- Expulsion: Particularly during Valsalva; managed by upsizing or switching pessary type.
- Urinary symptoms: Ring pessaries may correct or worsen urinary incontinence depending on urethral geometry.
Long-term success rates for pessary use are 50–75% at one year. Pessary use does not worsen prolapse or preclude later surgery, and many women successfully manage symptoms with pessaries indefinitely without progression to surgical repair.
9. Surgical Options
Surgery is indicated for symptomatic POP Stage III–IV that has not responded adequately to conservative measures, or for Stage II prolapse with significant quality-of-life impact. The three main surgical categories are native tissue repair, mesh-augmented repair, and obliterative procedures.
Native Tissue Repair
Native tissue procedures use the patient's own fascial and connective tissue to reconstruct pelvic support.
- Anterior colporrhaphy: Plication of the pubocervical fascia to reduce cystocele.
- Posterior colporrhaphy and perineorrhaphy: Plication of the rectovaginal fascia and perineal body to reduce rectocele and restore perineal support.
- Uterosacral ligament suspension (USLS): Apical repair attaching the vaginal vault to the remnants of the uterosacral ligaments bilaterally; performed vaginally or laparoscopically.
- Sacrospinous ligament fixation (SSLF): Unilateral or bilateral attachment of the vaginal apex to the sacrospinous ligament; vaginal approach; well-validated with long-term data.
Native tissue repair avoids mesh-related complications but carries anatomical recurrence rates of 10–30% over 5–10 years, particularly for the anterior compartment. The OPTIMAL trial demonstrated equivalent outcomes between vaginal USLS and SSLF at 2 years.
Synthetic Mesh
The FDA issued safety communications in 2008 and 2011 regarding transvaginal mesh for POP repair, citing higher complication rates (mesh erosion, dyspareunia, chronic pelvic pain, need for reoperation) compared to native tissue repair without a clear efficacy benefit. In 2019 the FDA ordered manufacturers to stop selling transvaginal mesh products for anterior and posterior compartment POP repair. Transvaginal mesh for POP is therefore largely abandoned in current practice.
By contrast, abdominal and laparoscopic/robotic mesh approaches (sacrocolpopexy) remain the gold standard for apical prolapse, with a proven safety and efficacy profile distinct from transvaginal mesh complications.
Obliterative Procedures
- LeFort colpocleisis: The anterior and posterior vaginal walls are sutured together, obliterating the vaginal canal and preventing organ descent. Suitable for elderly or medically frail women who no longer wish to have penetrative intercourse. Success rates approach 95%; operative time and blood loss are minimal; anesthesia can often be regional. The procedure is not reversible.
- Complete colpocleisis: Variant for post-hysterectomy vaginal vault prolapse in women who decline or cannot tolerate more extensive surgery.
10. Sacrocolpopexy and Apical Repair
Sacrocolpopexy is considered the gold standard surgical procedure for apical compartment prolapse (uterine prolapse or post-hysterectomy vaginal vault prolapse). It provides durable, anatomically correct apical support by bridging the vaginal apex to the anterior longitudinal ligament of the sacrum at S1–S2 using a Y-shaped synthetic mesh graft.
Technique and Approach
- Open abdominal sacrocolpopexy: The original approach; well-validated with the longest follow-up data (10+ years).
- Laparoscopic sacrocolpopexy: Equivalent anatomical outcomes with shorter hospital stay and faster recovery than open surgery.
- Robotic-assisted sacrocolpopexy: The most widely adopted minimally invasive approach in the United States; ergonomically superior for surgeons during complex intrapelvic suturing; outcomes equivalent to laparoscopic with further reduction in blood loss and hospital stay; higher device cost.
The mesh is sutured to the anterior and posterior vaginal walls (over the bladder and rectum, respectively) and to the anterior longitudinal ligament of the sacrum, restoring the normal horizontal vaginal axis. When the uterus is present, the surgeon may perform a concurrent hysterectomy followed by vault suspension, or — increasingly — a hysteropexy (sacrohysteropexy) leaving the uterus in place.
Uterus-Preserving Hysteropexy
Women who wish to retain their uterus — whether for fertility, personal preference, or cultural reasons — are increasingly offered hysteropexy rather than hysterectomy-plus-vault suspension. Sacrohysteropexy (abdominal attachment of the uterus to the sacrum via mesh) and uterosacral ligament hysteropexy (vaginal approach) have demonstrated comparable success rates to hysterectomy-based repair in RCTs, with equivalent mesh erosion rates and shorter operating times. Uterine preservation is now considered a valid and preferred option when appropriate for the individual patient.
Outcomes
- Anatomical success (apical compartment) at 5 years: 78–90%.
- Mesh erosion rate: 3–5% (substantially lower than transvaginal mesh, attributed to the abdominal rather than vaginal placement).
- The CARE trial (Brubaker et al., 2006) demonstrated that adding a Burch colposuspension at the time of sacrocolpopexy significantly reduced postoperative stress incontinence in women without preoperative leakage, establishing concurrent incontinence prevention as standard practice for women at high risk.
- The OPTIMAL trial compared vaginal USLS to vaginal SSLF for apical prolapse; both achieved similar 2-year anatomical and functional outcomes.
Postoperative Recovery
Women are typically advised to avoid lifting objects heavier than 5–10 pounds for 6–8 weeks after sacrocolpopexy and to defer sexual intercourse for 6 weeks to allow mesh integration and vaginal healing. Pelvic floor physical therapy after surgery is strongly recommended to rebuild neuromuscular coordination, prevent constipation-related straining, and reduce recurrence risk. Most women return to full activity within 8–12 weeks of robotic or laparoscopic repair.
11. References
- Barber MD, Maher C. Epidemiology and outcome assessment of pelvic organ prolapse. Int Urogynecol J. 2013;24(11):1783–1790. — PMID: 24142054
- Bump RC, Mattiasson A, Bo K, et al. The standardization of terminology of female pelvic organ prolapse and pelvic floor dysfunction. Am J Obstet Gynecol. 1996;175(1):10–17. — PMID: 8694033
- Maher C, Feiner B, Baessler K, et al. Surgical management of pelvic organ prolapse in women. Cochrane Database Syst Rev. 2013;(4):CD004014. — PMID: 23633316
- DeLancey JO. Anatomic aspects of vaginal eversion after hysterectomy. Am J Obstet Gynecol. 1992;166(6 Pt 1):1717–1724. — Search PubMed
- Hagen S, Stark D, Glazener C, et al. Individualised pelvic floor muscle training in women with pelvic organ prolapse (POPPY): a multicentre randomised controlled trial. Lancet. 2014;383(9919):796–806. — Search PubMed
- Barber MD, Brubaker L, Nygaard I, et al. Defining success after surgery for pelvic organ prolapse. Obstet Gynecol. 2009;114(3):600–609. — PMID: 19701041
- Nygaard I, Barber MD, Burgio KL, et al. Prevalence of symptomatic pelvic floor disorders in US women. JAMA. 2008;300(11):1311–1316. — PMID: 18799443
- Subak LL, Waetjen LE, van den Eeden S, et al. Cost of pelvic organ prolapse surgery in the United States. Obstet Gynecol. 2001;98(4):646–651. — Search PubMed
- Richter HE, Albo ME, Zyczynski HM, et al. Retropubic versus transobturator midurethral slings for stress incontinence. N Engl J Med. 2010;362(22):2066–2076. — PMID: 20479459
- Culligan PJ, Salamo L, Murphy M, et al. Long-term success of abdominal sacrocolpopexy using synthetic mesh. Am J Obstet Gynecol. 2002;187(6):1473–1480. — Search PubMed
- Brubaker L, Cundiff GW, Fine P, et al. Abdominal sacrocolpopexy with Burch colposuspension to reduce urinary stress incontinence. N Engl J Med. 2006;354(15):1557–1566. — PMID: 16611949
- Swift SE. The distribution of pelvic organ support in a population of female subjects seen for routine gynecologic health care. Am J Obstet Gynecol. 2000;183(2):277–285. — PMID: 10942459
Research Papers
- Pelvic organ prolapse treatment (PubMed)
- Uterine prolapse surgery outcomes (PubMed)
- Pelvic floor muscle training for prolapse (PubMed)
- Pessary use in pelvic organ prolapse (PubMed)
- Sacrocolpopexy robotic outcomes (PubMed)
- Levator ani avulsion and prolapse (PubMed)
- Hysteropexy uterine preservation (PubMed)
- POP-Q staging system (PubMed)
Connections
- Reproductive Medicine
- Premature Ovarian Insufficiency
- Menopause
- Urinary Incontinence
- Osteoporosis
- Constipation
- Obesity
- Postpartum Recovery
- Overactive Bladder
- Vitamin D
- Calcium
- Magnesium
- Hypertension