Urinary Incontinence
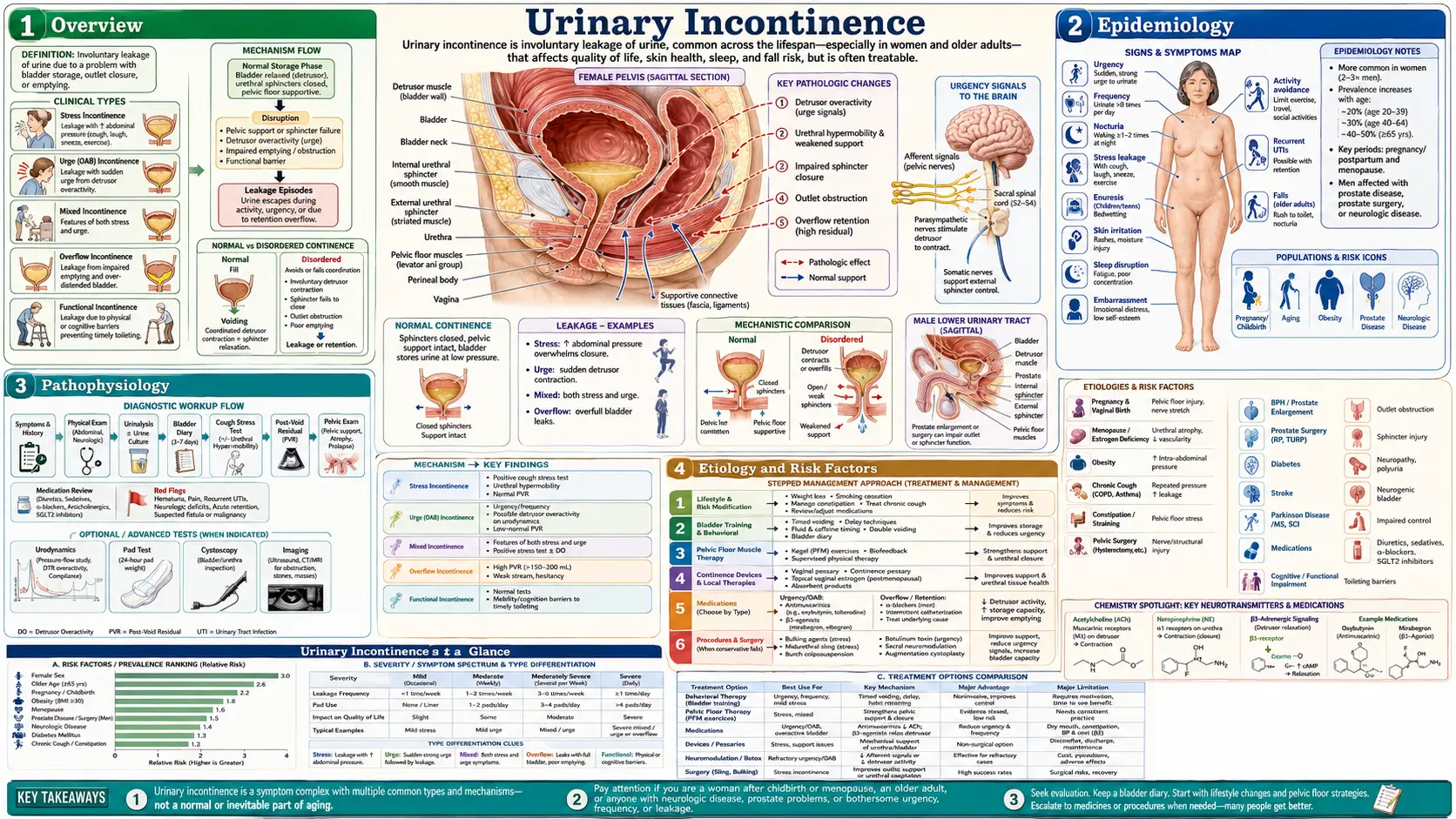
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Etiology and Risk Factors
- Clinical Presentation
- Diagnosis
- Treatment
- Complications
- Prognosis
- Prevention
- Recent Research and Advances
- References & Research
- Research Papers
- Connections
- Featured Videos
1. Overview
Urinary incontinence is the involuntary leakage of urine — anything from a few drops when you cough or laugh to a sudden, overwhelming need to go that you can't hold back. It is one of the most common health problems in the world, and also one of the most under-reported. Tens of millions of adults in the United States live with it, yet the great majority never mention it to a doctor. People assume it's just part of getting older, feel too embarrassed to bring it up, or quietly reorganize their lives around the nearest bathroom. The single most important message of this page is this: urinary incontinence is not a normal or inevitable part of aging, and in most people it can be significantly improved — often without surgery and sometimes without any medication at all. Leaking is a symptom, not a life sentence, and it is highly treatable once you know what type you have.
The reason so many people suffer needlessly is a quiet conspiracy of silence. Surveys consistently find that fewer than half of people with bothersome leakage ever raise it with a clinician, and that on average they wait years — sometimes more than a decade — before doing so. In the meantime they spend money on absorbent pads, avoid exercise, decline social invitations, sleep poorly because they're up all night, and feel ashamed of something that is enormously common and not their fault. If you take only one action from reading this, let it be the simplest and most powerful one: tell your doctor. The conversation is routine for them, the evaluation is usually straightforward, and the first-line treatments are safe, free or cheap, and genuinely effective.
Understanding incontinence starts with understanding that it is not a single condition. There are several distinct types, each driven by a different mechanism and each responding to a different treatment. Getting the type right is the key that unlocks the right plan — which is exactly why this page spends so much time distinguishing them.
2. Epidemiology
Urinary incontinence affects a strikingly large share of the adult population. Prevalence estimates vary with how the question is asked, but large population surveys consistently find that roughly a quarter to a third of community-dwelling adult women report some degree of leakage, with the figure rising further among older women and those in long-term care. In men the overall prevalence is lower — in the range of 10–15% — but it climbs sharply with age and after prostate surgery. Overactive bladder, the syndrome behind most urge incontinence, affects on the order of 16% of US adults of both sexes (Stewart 2003).
Two patterns stand out. First, incontinence is roughly twice as common in women as in men for most of adult life, reflecting the anatomy of the female pelvic floor and the lasting effects of pregnancy, childbirth, and menopause. Second, prevalence rises steadily with age — but, crucially, rising with age is not the same as being caused by age. Older bodies accumulate more of the contributing factors (weaker pelvic muscles, prostate enlargement, more medications, more constipation, less mobility), and those factors are what can be treated. A landmark European survey (Irwin 2006) documented just how widespread lower-urinary-tract symptoms are across both sexes, underscoring that this is a mainstream health issue, not a niche one.
3. Pathophysiology
Normal continence depends on a quiet, coordinated truce between two systems: a storage system (the bladder relaxing to fill while its outlet stays closed) and an emptying system (the bladder muscle contracting while the outlet opens). The bladder wall muscle is called the detrusor. The outlet is guarded by the urethral sphincters and supported from below by the pelvic floor muscles, a hammock of muscle slung between the pubic bone and the tailbone. The brain, spinal cord, and pelvic nerves keep the whole thing politely in check so you stay dry until you decide otherwise.
Incontinence happens when that balance breaks down, and it breaks down in a handful of recognizable ways:
- Stress incontinence — the outlet is too weak to stay shut when pressure in the abdomen suddenly rises. A cough, sneeze, laugh, jump, or heavy lift drives urine past a sphincter or pelvic-floor hammock that can no longer hold the line. This is fundamentally a problem of support, not of the bladder muscle itself.
- Urge incontinence (overactive bladder) — the detrusor muscle contracts on its own, before you're ready, producing a sudden, hard-to-defer urge followed by leakage. Here the problem is an overactive or poorly controlled bladder muscle, often with no clear cause.
- Overflow incontinence — the bladder never fully empties, fills past capacity, and then dribbles. The cause is either an obstruction at the outlet (most commonly an enlarged prostate — see benign prostatic hyperplasia) or a weak/underactive detrusor that can't generate a proper contraction (often from nerve damage).
Because the broken mechanism is different in each case, the fix is different in each case. A sphincter problem is not solved by a bladder-muscle drug, and an overactive bladder is not solved by a sling. Sorting out which mechanism is at work is the heart of the evaluation.
4. Etiology and Risk Factors
The major types of incontinence each have a typical backstory:
- Stress incontinence is most often the legacy of pregnancy and vaginal childbirth, which stretch and sometimes injure the pelvic floor and its nerves. It is also driven by menopause (loss of estrogen thins and weakens urethral tissue), by chronic strain (obesity, chronic cough, heavy lifting), and in men by prostate surgery, which can damage the sphincter. Leakage with coughing, laughing, exercise, or lifting is its signature.
- Urge incontinence / overactive bladder produces a sudden powerful urge, urinary frequency (going often), and nocturia (waking at night to urinate). It frequently has no identifiable cause, but can be provoked or worsened by bladder irritants, neurological disease (see multiple sclerosis, Parkinson's disease, stroke), and bladder inflammation.
- Mixed incontinence — both stress and urge features together — is extremely common, especially in older women. Treatment usually targets whichever component bothers the person most.
- Overflow incontinence — constant or post-void dribbling from incomplete emptying. In men the classic cause is BPH obstructing the outlet; in both sexes nerve problems (diabetic nerve damage, spinal issues) can leave the bladder unable to squeeze.
- Functional incontinence — the urinary tract works, but a mobility or cognitive problem (arthritis, a walker, dementia) stops the person reaching and using the toilet in time.
Before settling on a type, it is essential to look for reversible, transient causes — things that can make anyone leak temporarily and that often resolve completely once corrected. Geriatricians remember these with the memory aid "DIAPPERS", but the idea is simple: check first for a urinary tract infection (see UTIs), medications (especially diuretics — "water pills" — and sedatives), constipation and stool impaction pressing on the bladder, excess intake of caffeine and alcohol, and uncontrolled diabetes producing high urine volumes (see diabetes). Fixing a treatable trigger can sometimes make the leakage disappear without any further treatment at all.
5. Clinical Presentation
The way leakage shows up usually points straight to its type. Leaking with effort — the moment you cough, sneeze, laugh, run, or pick up a grandchild — is the hallmark of stress incontinence. A sudden urge that you can't put off, often with frequent daytime trips and waking at night, points to urge incontinence. A combination of both is mixed. A constant dribble, a feeling that the bladder never empties, or a weak stream (especially in older men) suggests overflow.
Whatever the type, the impact on daily life is real and deserves to be taken seriously — you are not making a fuss over nothing. Constant moisture can cause skin breakdown and rashes. The urgent dash to the bathroom is a major cause of falls and fractures in older adults, especially at night. Many people withdraw from exercise, travel, intimacy, and social life, and rates of anxiety, isolation, and depression are meaningfully higher among those with incontinence. None of this is vanity or weakness. It is the predictable toll of a treatable medical problem that too often goes unspoken — which is exactly why naming it out loud to a clinician is the turning point.
6. Diagnosis
The good news is that most incontinence can be diagnosed with simple, low-tech tools — no scary tests required for the typical case. The core evaluation is:
- History — when do you leak, how much, what triggers it, how many pads, how often you go, whether you wake at night. This alone usually identifies the type.
- A bladder diary — arguably the single most useful tool in the whole evaluation. For just 2–3 days you jot down what and when you drink, when you urinate and roughly how much, and when leaks happen and what you were doing. The pattern that emerges (urge versus effort, the role of caffeine, overnight volumes) frequently makes the diagnosis and guides the treatment more clearly than any machine.
- Physical exam — a focused pelvic exam in women (looking for prolapse and pelvic-floor strength) or a prostate exam in men.
- Urinalysis — a quick urine test to rule out infection, blood, or high sugar.
- Post-void residual — a painless bladder ultrasound after you urinate to confirm you're emptying properly. A high residual points to overflow.
Most people never need anything beyond this. Referral to a urologist or urogynecologist, and specialized urodynamic testing (which measures bladder pressures during filling), is reserved for specific situations: leakage that doesn't fit a clear pattern, failure of first-line treatment, before incontinence surgery, prior pelvic surgery or radiation, suspected neurological cause, or warning signs such as blood in the urine or pain.
7. Treatment
Here is the most empowering fact of all: the first-line treatments for incontinence are behavioral and lifestyle measures — they cost little or nothing, carry essentially no risk, and have strong evidence behind them. National guidelines (Qaseem 2014) recommend trying these before any drug. The right combination depends on your type.
Lifestyle and behavioral measures (try these first, for every type)
- Pelvic floor muscle training (Kegels) — the cornerstone of treatment, first-line for stress incontinence and genuinely helpful for urge as well. A large Cochrane review (Dumoulin 2018) found that women who do pelvic-floor training are far more likely to report cure or improvement than those who don't. The catch is that Kegels are very commonly done wrong — squeezing the wrong muscles, holding the breath, or bearing down. If self-directed exercises aren't working within a few weeks, ask for a referral to a pelvic-floor physical therapist, who can confirm you're using the right muscles and add biofeedback. This is not a minor footnote: proper technique is often the difference between failure and success.
- Bladder training / timed voiding — the mainstay behavioral therapy for urge incontinence. You urinate on a fixed schedule and gradually stretch the interval, retraining the bladder to hold more and the urge to settle. A Cochrane review (Funada 2023) supports its benefit.
- Weight loss — one of the strongest evidence-based interventions there is. A randomized trial (Subak 2009) showed that even a modest weight loss of about 8% in overweight and obese women cut weekly leakage episodes substantially. If you carry extra weight, losing some of it is one of the most reliable things you can do (see obesity).
- Fluid and caffeine management — cutting back on caffeine and alcohol (both bladder irritants and diuretics) and spreading fluids out across the day, with less in the evening, reduces urgency and nighttime trips.
- Treat constipation — a full rectum presses on the bladder and worsens both urge and stress symptoms; regular bowel habits genuinely help.
An important myth to debunk: many people try to control leaks by drinking as little as possible. This usually backfires. Concentrated urine is more irritating to the bladder lining and can actually increase urgency and frequency — and chronic under-drinking raises the risk of UTIs and constipation, which worsen incontinence further. The goal is sensible, evenly-spaced fluids, not dehydration.
Medications and procedures for urge incontinence / overactive bladder
- Antimuscarinic (anticholinergic) drugs — oxybutynin, tolterodine, solifenacin and others calm the overactive detrusor. They work, but they carry a real and honestly stated concern: this drug class has been linked in large observational studies (Gray 2015; Coupland 2019) to a higher risk of dementia with cumulative use, and they commonly cause dry mouth, constipation, and confusion in older adults. Because of this "anticholinergic burden," they should be used cautiously — and often avoided — in elderly or cognitively vulnerable patients.
- Beta-3 agonists (mirabegron, vibegron) — a newer class that relaxes the bladder by a different mechanism without the anticholinergic brain risk, making them the generally preferred option in older adults. Both have solid trial evidence (Khullar 2013 for mirabegron; Staskin 2020, the EMPOWUR trial, for vibegron). Their main caution is a modest rise in blood pressure, which should be monitored.
- Bladder Botox (onabotulinumtoxinA) — injected into the bladder wall, it is highly effective for refractory urge incontinence; a head-to-head trial (Visco 2012) found it at least as good as anticholinergic pills, with a tradeoff of occasional incomplete emptying requiring temporary catheterization.
- Percutaneous tibial nerve stimulation (PTNS) — a low-risk office therapy using a fine needle near the ankle to modulate the bladder nerves, shown effective versus sham (Peters 2010).
- Sacral neuromodulation — an implanted "bladder pacemaker" for severe, treatment-resistant cases, with durable long-term benefit (van Kerrebroeck 2007).
Procedures for stress incontinence
- Pessary — a removable silicone device worn in the vagina to support the urethra; a simple, non-surgical option, especially useful with prolapse.
- Urethral bulking agents — injections that plump the urethral lining to improve closure; less invasive than surgery but generally less durable (Kirchin 2017).
- Midurethral sling — the most effective surgical treatment for stress incontinence, supporting the urethra with a small strip of mesh; long-term trials (Richter 2010) and guidelines (Kobashi 2017) confirm high cure rates. Honest context on mesh: the well-publicized safety problems and lawsuits centered largely on transvaginal mesh kits used for pelvic-organ prolapse, which were withdrawn. The midurethral sling for incontinence is a different, much-studied device that major urology and gynecology bodies continue to endorse as safe and effective — though, as with any surgery, the small risks (pain, mesh exposure, voiding difficulty) deserve a frank discussion.
Special situations
- Postmenopausal urogenital symptoms — low-dose vaginal estrogen can relieve the dryness, urgency, and recurrent-UTI cycle of genitourinary syndrome of menopause; a Cochrane review (Cody 2012) found local (vaginal) estrogen helpful for incontinence symptoms (while systemic estrogen pills were not). See menopause & HRT.
- Men after prostate surgery — formal pelvic-floor rehabilitation is the starting point; persistent leakage can be treated with a male sling or an artificial urinary sphincter, the latter being the gold standard for severe post-prostatectomy incontinence. Early one-to-one pelvic-floor therapy has been studied directly in this group (Glazener 2011).
8. Complications
Left unaddressed, incontinence carries real downstream harms — another reason the silence is so costly. Persistent skin moisture leads to incontinence-associated dermatitis, rashes, and pressure injuries. The urgent rush to the toilet, particularly overnight, is a well-documented driver of falls and hip fractures in older people. Recurrent or untreated urinary tract infections can result from incomplete emptying (overflow) or from chronic under-drinking. Overflow from severe outlet obstruction can, rarely, back pressure up to the kidneys. And the psychological burden — social withdrawal, loss of independence, anxiety, and depression — can be as disabling as the physical symptoms, and is itself a strong reason to seek help rather than cope alone.
9. Prognosis
The outlook is genuinely encouraging, which is the note worth ending on. For stress incontinence, pelvic-floor training improves or cures a large fraction of women, and the midurethral sling cures the great majority of those who choose surgery. For urge incontinence, behavioral therapy plus a beta-3 agonist (or, when appropriate, an antimuscarinic) controls symptoms in most people, and Botox or neuromodulation rescues most of the rest. Even overflow from BPH often resolves once the obstruction is treated. Few people achieve "perfect" dryness in every circumstance, but the realistic and common outcome is a substantial reduction in leakage and a large gain in quality of life. The main thing standing between a person and that outcome is usually not the limits of medicine — it's the decision to bring it up.
10. Prevention
Much of incontinence is preventable, or at least postponable, with habits that also happen to be good for general health:
- Keep the pelvic floor fit. Regular pelvic-floor exercises — including during and after pregnancy — build the support that prevents stress leakage later. It's worth learning the correct technique once from a professional.
- Maintain a healthy weight. Excess abdominal weight pushes constantly on the bladder; staying lean is one of the most effective preventive measures (see obesity).
- Look after your bowels. Avoiding chronic constipation through fiber, fluids, and activity protects the bladder from pressure.
- Moderate caffeine and alcohol and stay sensibly hydrated — not under-hydrated.
- Don't smoke. A chronic smoker's cough hammers the pelvic floor and raises bladder-cancer risk.
And the most important preventive act of all is behavioral: don't ignore early leakage, and don't suffer in silence. Ask for help. Incontinence almost always responds better when addressed early, and the conversation that unlocks treatment is one short, ordinary appointment away.
11. Recent Research and Advances
The field has shifted decisively toward safer, less invasive options. The biggest practical change in the last decade is the rise of the beta-3 agonists (mirabegron and, more recently, vibegron via the EMPOWUR trial), which give clinicians an effective overactive-bladder drug that sidesteps the dementia and cognitive concerns of the older anticholinergics — a concern that itself was sharpened by large pharmacoepidemiology studies linking cumulative anticholinergic exposure to dementia risk. That work has driven a broad effort to de-prescribe high anticholinergic-burden drugs in older adults.
On the device side, rechargeable, MRI-compatible sacral neuromodulation systems and refined PTNS protocols (including implantable tibial-nerve stimulators) have expanded the menu for refractory urge incontinence. For stress incontinence, long-term follow-up of midurethral slings continues to support their durability and safety, helping clinicians separate the genuine, well-studied incontinence sling from the discontinued prolapse-mesh products at the center of past controversy. Active research areas include regenerative approaches (stem-cell and tissue-engineering strategies to restore sphincter function) and better tools — including app-based bladder diaries and biofeedback — to make first-line behavioral therapy easier to do correctly at home.
12. References & Research
Historical Background
Modern incontinence treatment begins with gynecologist Arnold Kegel, who in 1948 described and popularized the pelvic-floor muscle exercises that still bear his name — the first effective non-surgical therapy for stress incontinence. Surgical management was transformed in the late 1990s and 2000s by the midurethral synthetic sling, a minimally invasive operation that became the most common continence procedure worldwide; large randomized trials and long-term follow-up established its effectiveness, even as a separate generation of transvaginal prolapse-mesh kits drew safety warnings and litigation that were frequently — and inaccurately — conflated with the incontinence sling. Pharmacologic and device therapy advanced in parallel: the beta-3 agonist mirabegron (approved in the early 2010s) and vibegron offered overactive-bladder relief without anticholinergic cognitive risk, while sacral neuromodulation, bladder Botox, and percutaneous tibial nerve stimulation gave clinicians effective options for refractory urge incontinence.
Key Research Papers
- Dumoulin C, Cacciari LP, Hay-Smith EJC. Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. Cochrane Database of Systematic Reviews 2018; vol 2018, issue 10. doi:10.1002/14651858.CD005654.pub4
- Subak LL, Wing R, West DS, et al. Weight loss to treat urinary incontinence in overweight and obese women. New England Journal of Medicine 2009; 360(5):481–490. doi:10.1056/NEJMoa0806375
- Qaseem A, Dallas P, Forciea MA, et al. Nonsurgical management of urinary incontinence in women: a clinical practice guideline from the American College of Physicians. Annals of Internal Medicine 2014; 161(6):429–440. doi:10.7326/M13-2410
- Funada S, Yoshioka T, Luo Y, et al. Bladder training for treating overactive bladder in adults. Cochrane Database of Systematic Reviews 2023; vol 2023, issue 10. doi:10.1002/14651858.CD013571.pub2
- Nygaard I. Idiopathic urgency urinary incontinence. New England Journal of Medicine 2010; 363(12):1156–1162. doi:10.1056/NEJMcp1003849
- Khullar V, Amarenco G, Angulo JC, et al. Efficacy and tolerability of mirabegron, a beta-3-adrenoceptor agonist, in patients with overactive bladder. European Urology 2013; 63(2):283–295. doi:10.1016/j.eururo.2012.10.016
- Staskin D, Frankel J, Varano S, et al. International phase III, randomized, double-blind, placebo and active controlled study to evaluate the safety and efficacy of vibegron in patients with symptoms of overactive bladder: EMPOWUR. Journal of Urology 2020; 204(2):316–324. doi:10.1097/JU.0000000000000807
- Gray SL, Anderson ML, Dublin S, et al. Cumulative use of strong anticholinergics and incident dementia. JAMA Internal Medicine 2015; 175(3):401–407. doi:10.1001/jamainternmed.2014.7663
- Coupland CAC, Hill T, Dening T, et al. Anticholinergic drug exposure and the risk of dementia: a nested case-control study. JAMA Internal Medicine 2019; 179(8):1084–1093. doi:10.1001/jamainternmed.2019.0677
- Visco AG, Brubaker L, Richter HE, et al. Anticholinergic therapy vs. onabotulinumtoxinA for urgency urinary incontinence. New England Journal of Medicine 2012; 367(19):1803–1813. doi:10.1056/NEJMoa1208872
- Richter HE, Albo ME, Zyczynski HM, et al. Retropubic versus transobturator midurethral slings for stress incontinence. New England Journal of Medicine 2010; 362(22):2066–2076. doi:10.1056/NEJMoa0912658
- Kobashi KC, Albo ME, Dmochowski RR, et al. Surgical treatment of female stress urinary incontinence: AUA/SUFU guideline. Journal of Urology 2017; 198(4):875–883. doi:10.1016/j.juro.2017.06.061
- Cody JD, Jacobs ML, Richardson K, et al. Oestrogen therapy for urinary incontinence in post-menopausal women. Cochrane Database of Systematic Reviews 2012; vol 2012, issue 10. doi:10.1002/14651858.CD001405.pub3
- Stewart WF, Van Rooyen JB, Cundiff GW, et al. Prevalence and burden of overactive bladder in the United States. World Journal of Urology 2003; 20(6):327–336. doi:10.1007/s00345-002-0301-4
Research Papers
The links below run live searches on PubMed, the U.S. National Library of Medicine's database of biomedical literature. Use them to explore the latest peer-reviewed research on urinary incontinence and its treatments.
- Urinary incontinence management
- Stress urinary incontinence treatment
- Overactive bladder and urge incontinence
- Pelvic floor muscle training for incontinence
- Bladder training for overactive bladder
- Midurethral sling for stress incontinence
- Beta-3 agonists (mirabegron, vibegron)
- Anticholinergic burden and dementia risk
- Sacral neuromodulation for incontinence
- Bladder Botox for urge incontinence
- Post-prostatectomy urinary incontinence
- Vaginal estrogen for genitourinary syndrome of menopause
Connections
- Benign Prostatic Hyperplasia — enlarged prostate, the classic cause of overflow incontinence in men.
- Urinary Tract Infections — a reversible, transient cause of leakage to rule out first.
- Interstitial Cystitis — painful bladder syndrome that overlaps with urgency and frequency.
- Prostate Conditions — prostate disease and surgery as drivers of male incontinence.
- Kidney Stones — another common lower-urinary-tract problem causing urgency and pain.
- Menopause & HRT — estrogen loss and vaginal-estrogen treatment for urogenital symptoms.
- Perimenopause — the transition when bladder and pelvic-floor changes often begin.
- Diabetes — uncontrolled high blood sugar raises urine volume and damages bladder nerves.
- Obesity — extra weight worsens leakage; modest weight loss is strongly evidence-based.
- Multiple Sclerosis — a neurological cause of overactive bladder and incontinence.
- Parkinson's Disease — commonly causes urgency, frequency, and nocturia.
- Dementia — a driver of functional incontinence and the reason to limit anticholinergic drugs.
- Urology — the full collection of urinary-tract and male-reproductive conditions.
- All Conditions — browse every disease and condition on the site.