Tapeworm Symptoms — Intestinal Disease, Neurocysticercosis, and Diagnosis
Tapeworms are a group of parasitic flatworms that range from nearly harmless intestinal passengers to the cause of one of the world's leading preventable neurological emergencies. Understanding which species causes which kind of illness — and why the pork tapeworm is uniquely dangerous — is the key to making sense of tapeworm symptoms. This page covers all five clinically important human tapeworm species, the full spectrum of disease from mild intestinal colonization to brain cysts and hydatid rupture, and how each is recognized. The information here reflects the medical literature and is educational; it is not a substitute for care by a clinician.
Table of Contents
- Tapeworm Species Overview
- The Two Faces of Taenia solium
- Species-Specific Presentations
- Intestinal Tapeworm Symptoms
- Fish Tapeworm and Vitamin B12 Deficiency
- Neurocysticercosis
- Echinococcus and Hydatid Disease
- Who Is Most at Risk
- Key Research Papers
- Connections
- Featured Videos
1. Tapeworm Species Overview
Five tapeworm species account for nearly all human tapeworm disease. They differ in size, route of transmission, intermediate host, and crucially in the severity of illness they cause.
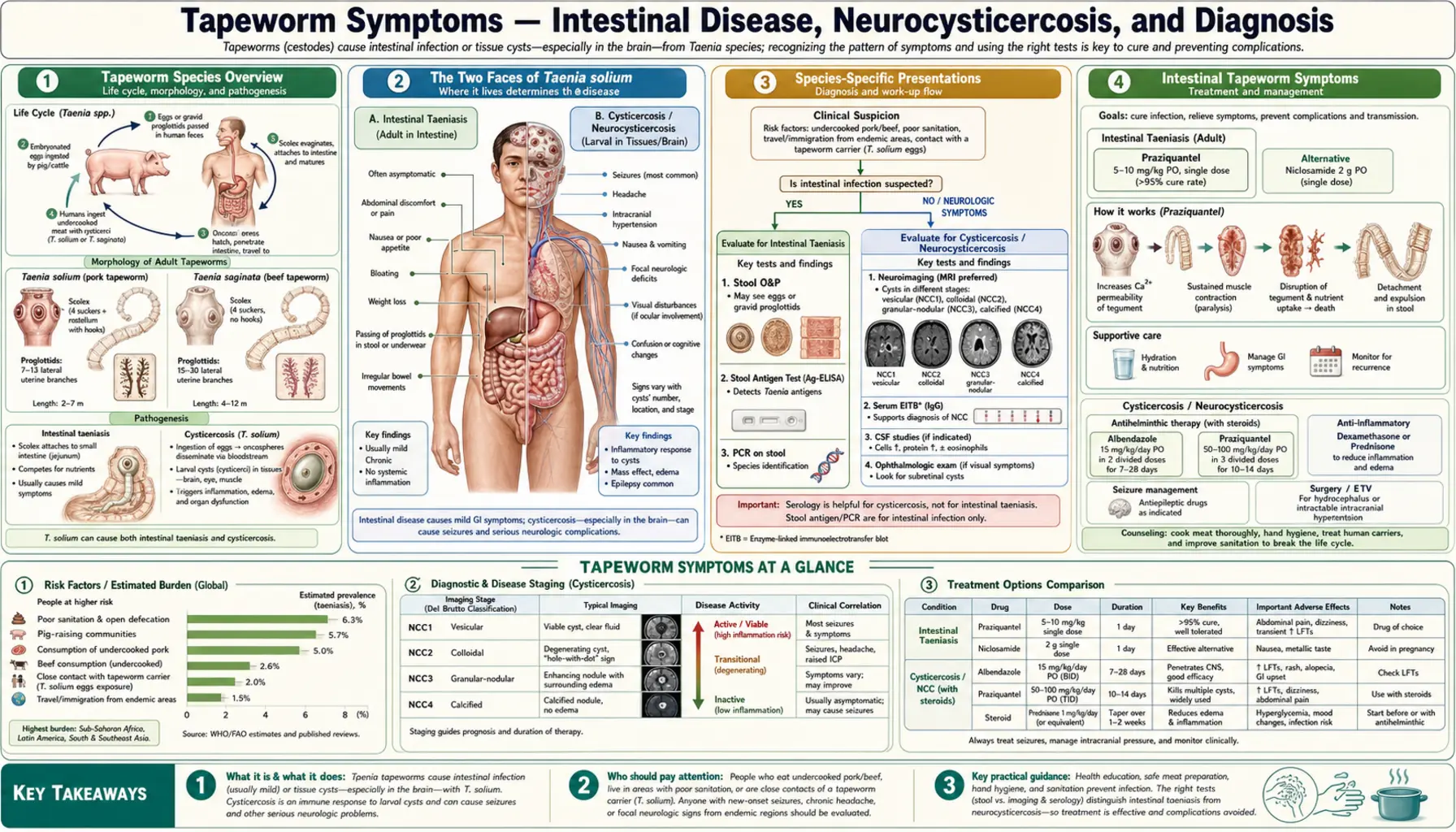
Taenia solium (pork tapeworm) is the most medically important tapeworm on earth. Adults reach 2–4 meters in the human small intestine. Infection with the adult worm (taeniasis) comes from eating undercooked pork containing larval cysts. Infection with the larvae themselves (cysticercosis) comes from swallowing microscopic eggs in contaminated food, water, or on unwashed hands — a completely separate route. T. solium is endemic in Latin America, sub-Saharan Africa, South and Southeast Asia, and parts of Eastern Europe. It is the only tapeworm that routinely causes serious brain disease in people.
Taenia saginata (beef tapeworm) is the most common tapeworm in regions that eat raw or lightly cooked beef. Adults grow to 4–10 meters. It causes only intestinal infection; because its eggs cannot develop into tissue-invading larvae in humans, there is no risk of cysticercosis. Proglottid segments passing spontaneously from the anus — sometimes while the person is walking — are its most recognizable feature.
Diphyllobothrium latum (fish tapeworm, broad tapeworm) is the largest tapeworm parasite of humans, reaching up to 10 meters. It is acquired by eating raw or undercooked freshwater fish, particularly in Scandinavia, Russia, Japan, and North America near the Great Lakes and Pacific Northwest. Its defining medical consequence is competitive sequestration of vitamin B12 in the ileum, leading to megaloblastic anemia in a minority of heavily infected patients.
Hymenolepis nana (dwarf tapeworm) is the most common tapeworm worldwide despite its small size (2–4 cm). Unlike the other species listed here, it completes its entire life cycle within a single human host — eggs hatched in the gut produce larvae that develop to adults in the same intestine without requiring an intermediate animal host. It spreads by the fecal-oral route, is especially prevalent in children in institutional settings, and can autoinfect its host repeatedly.
Echinococcus granulosus and E. multilocularis are small tapeworms of dogs and foxes. Humans are accidental dead-end hosts who swallow eggs. Instead of an adult worm in the gut, the infection takes the form of slowly enlarging, fluid-filled cysts in the liver (most commonly), lungs, and other organs. This is called hydatid disease or cystic echinococcosis. Rupture of a cyst can cause fatal anaphylactic shock.
2. The Two Faces of Taenia solium
Taenia solium is the only common tapeworm with two entirely different clinical faces, both produced by the same species but by completely different mechanisms. Grasping this distinction is the most important thing to understand about tapeworm disease.
Face 1: Taeniasis — the adult worm in the gut. A person eats undercooked pork containing larval cysts (cysticerci) embedded in muscle. Stomach acid dissolves the cyst wall, the larva attaches to the small intestinal wall, and over 2–3 months it grows into an adult tapeworm. The adult lives in the intestine, absorbs nutrients passively through its surface, and steadily produces egg-filled proglottid segments that pass in the stool. Most carriers have no or minimal symptoms. This form is called taeniasis and is usually mild.
Face 2: Cysticercosis — larvae in the body's tissues. Now consider a different route. A person swallows the microscopic eggs of T. solium — not larval cysts in pork, but eggs shed in human stool and spread by the fecal-oral route. The human body responds to these eggs the way a pig's body does: the eggs hatch in the small intestine, the released oncospheres (embryos) penetrate the intestinal wall, enter the bloodstream, and disseminate throughout the body. They preferentially settle in the brain, muscle, eye, and subcutaneous tissue, where each develops into a fluid-filled cyst called a cysticercus. This condition is cysticercosis, and when it involves the brain it is called neurocysticercosis (NCC).
The critical implication: you do not need to eat pork to develop cysticercosis. You need only to ingest T. solium eggs from contaminated food, water, or the unwashed hands of a tapeworm carrier — often a household member or food preparer. A person can even auto-infect themselves by transferring eggs from their own stool to their mouth if they carry an adult tapeworm. Cysticercosis is therefore a disease of fecal contamination, not of meat eating. Vegetarians and people who have never touched pork can and do develop neurocysticercosis if they are exposed to T. solium eggs.
3. Species-Specific Presentations
Each tapeworm species has a characteristic clinical fingerprint shaped by where it lives, how large it grows, and what tissues (if any) it invades.
Taenia saginata causes almost no systemic illness. The worm is large — occasionally exceeding 10 meters — but its symptoms are limited to the intestine. The most distinctive feature is the spontaneous, often surprising passage of motile proglottid segments through the anus, which may occur between bowel movements and can be felt as movement in the underwear or on the skin. Vague abdominal discomfort, mild nausea, and a slight increase in appetite are reported by some carriers, but many are completely asymptomatic until they see a segment in the toilet.
Taenia solium (intestinal form) produces intestinal symptoms indistinguishable from T. saginata. What sets it apart is the risk it creates: a person carrying an adult T. solium sheds thousands of eggs per day in their stool, creating a persistent source of cysticercosis risk for themselves and the people around them.
Diphyllobothrium latum typically causes no or minor intestinal symptoms. The clinically important feature is its ability to compete with the host for vitamin B12 absorption in the terminal ileum. The worm binds the intrinsic factor–B12 complex and takes up cobalamin at the expense of the host. In heavy or long-standing infection, this produces megaloblastic (macrocytic) anemia with the neurological complications of severe B12 deficiency including subacute combined degeneration of the spinal cord.
Hymenolepis nana most often causes mild or no symptoms in light infections. Heavier worm burdens (common in immunocompromised individuals and malnourished children) cause abdominal pain, diarrhea, and irritability. Because autoinfection is possible without leaving the host, untreated infections in people with impaired immunity can amplify dramatically.
Echinococcus remains clinically silent for years to decades while the cyst slowly enlarges. Presenting symptoms depend on cyst location: right upper quadrant pain or a palpable mass for liver cysts; cough, chest pain, or hemoptysis for pulmonary cysts. Cyst rupture — spontaneous or traumatic — releases hydatid fluid and can trigger severe anaphylaxis. Secondary seeding of daughter cysts at the rupture site can cause recurrent disease.
4. Intestinal Tapeworm Symptoms
When a tapeworm lives only in the intestine, the body's immune response to a large worm is surprisingly limited. The intestinal forms of tapeworm disease are frequently asymptomatic, discovered incidentally when a patient notices segments in the stool or on imaging for another reason.
When symptoms do occur they are typically mild and non-specific:
- Vague abdominal discomfort — mild cramping or a sense of fullness, most often in the epigastrium or periumbilical region
- Nausea — intermittent, rarely severe enough to cause vomiting
- Altered appetite — increased or decreased hunger; some carriers report persistent hunger despite adequate food intake
- Mild weight loss — modest, rarely exceeding a few kilograms, from nutrient competition with a large worm
- Bloating and flatulence — nonspecific, may reflect altered gut motility
- Diarrhea or constipation — inconsistent; most carriers have normal bowel habits
- Proglottid segments in stool or underwear — the pathognomonic finding; flat, whitish, seed-like pieces, actively motile for T. saginata
- Perianal pruritus — from migrating proglottids, especially with T. saginata
The absence of severe symptoms should not be taken as evidence that these infections are trivial. Beyond the nutritional competition and the discomfort, the intestinal tapeworm — specifically T. solium — is the source of the eggs that can cause cysticercosis in the carrier and in close contacts.
5. Fish Tapeworm and Vitamin B12 Deficiency
The fish tapeworm (Diphyllobothrium latum) occupies a special niche in the history of medicine: it was one of the first parasitic causes of a specific nutritional deficiency to be identified. In the early twentieth century, before the nature of vitamin B12 was understood, the megaloblastic anemia seen in Finnish and Scandinavian fish-tapeworm carriers was recognized as a distinct clinical entity called "bothriocephalus anemia."
The mechanism is competitive uptake. In the distal ileum, dietary vitamin B12 bound to intrinsic factor is normally absorbed by receptors in the ileal mucosa. The fish tapeworm, residing in the upper jejunum, produces binding proteins that compete with the intrinsic factor–B12 complex, sequestering cobalamin before it reaches its absorption site. The worm accumulates B12 at concentrations up to 10–20 times higher than the host's serum levels.
Not all carriers develop deficiency; worm burden and host diet matter. When deficiency does develop, the consequences include:
- Megaloblastic anemia — large, poorly functioning red blood cells; fatigue, pallor, shortness of breath on exertion
- Macrocytosis — elevated mean corpuscular volume (MCV) on a CBC
- Glossitis — a smooth, red, painful tongue (Hunter's glossitis)
- Subacute combined degeneration of the spinal cord — in severe deficiency: posterior column (vibration and proprioception loss) and lateral column (upper motor neuron signs) dysfunction; can be irreversible
- Cognitive changes — memory impairment, irritability, depression, in severe or prolonged cases
Diagnosis of this complication requires both parasite identification (eggs in stool) and B12 level measurement. Treatment is antiparasitic therapy plus B12 supplementation or injections to replenish stores; neurological recovery depends on how long the deficiency went unrecognized.
6. Neurocysticercosis
Neurocysticercosis is not a rare exotic disease. The World Health Organization estimates that 50 million people worldwide are currently infected, making it the most common preventable cause of epilepsy in the developing world. In regions where T. solium is endemic, up to 30% of all epilepsy cases in adults are attributable to NCC. In the United States, it is the most common parasitic disease of the central nervous system and a significant cause of new-onset seizures in immigrants from endemic regions.
Why the brain? When T. solium oncospheres disseminate through the bloodstream, they are filtered out in capillary beds. The brain, with its rich blood supply and immunologically privileged environment, accumulates cysts readily. Cysts may also develop in the spinal cord, the eye, or the subarachnoid space surrounding the brain stem.
Seizures are the presenting symptom in 50–70% of NCC patients and result from cortical irritation by cysts or by the inflammatory reaction when a cyst dies and the immune system attacks it. Seizures may be focal or generalized. A first seizure in an adult with no prior history, in the context of residence in or travel to an endemic region, should prompt consideration of NCC.
Other neurological manifestations depend on cyst location and number:
- Headache — most common non-seizure complaint; from inflammation or raised intracranial pressure
- Hydrocephalus — cysts in the ventricles or at the foramen of Monro block CSF flow; this is the most dangerous complication and requires urgent intervention
- Focal neurological deficits — motor weakness, sensory loss, or speech difficulty from cysts in eloquent cortex
- Meningitis — subarachnoid NCC triggers a basilar meningitis with neck stiffness, cranial nerve palsies, and risk of stroke from arteritis
- Cognitive impairment and behavioral changes — from multiple or strategically located cysts
- Spinal NCC — rare but severe; cysts in the spinal subarachnoid space or cord can cause progressive paraparesis, radiculopathy, or cauda equina syndrome
- Ocular cysticercosis — cysts in the vitreous, subretinal space, or anterior chamber cause floaters, visual field loss, and, if untreated, blindness; this form requires ophthalmological evaluation before any antiparasitic treatment is started because killing a cyst in the eye causes a destructive inflammatory reaction
The clinical course of NCC is shaped by the number of cysts, their stage (viable, degenerating, calcified), and their location. Viable cysts are often surprisingly well tolerated; the illness typically worsens when cysts begin to degenerate because the dying cyst provokes intense perilesional inflammation that irritates surrounding brain tissue. Calcified cysts can continue to provoke seizures years after the parasite itself is dead.
7. Echinococcus and Hydatid Disease
Echinococcus is biologically distinct from Taenia and Diphyllobothrium — adult worms live only in the intestines of dogs and related canids, not in humans. Humans are accidental dead-end intermediate hosts who swallow eggs passed in canid feces. Two species cause almost all human disease:
Echinococcus granulosus causes cystic echinococcosis (CE), also called hydatid disease. The larvae develop into large, fluid-filled unilocular cysts that grow slowly — typically 1–5 cm per year — in the liver (70% of cases), lungs (20%), and rarely other organs. Patients may be asymptomatic for years or decades. Symptoms arise when the cyst is large enough to compress adjacent structures (biliary obstruction, portal hypertension, pulmonary atelectasis) or when the cyst ruptures. Rupture is a medical emergency: the hydatid fluid is intensely antigenic and can cause severe anaphylactic shock, and seeding of daughter cysts at the rupture site can establish recurrent disease throughout the abdomen or pleural cavity.
Echinococcus multilocularis causes alveolar echinococcosis (AE), a far more aggressive disease. The larval mass grows by continuous budding in an infiltrative, tumor-like pattern, predominantly in the liver. It erodes into bile ducts and blood vessels, and untreated it is nearly uniformly fatal. AE is endemic in parts of central Europe, central Asia, China, and the subarctic regions of North America and Russia.
Key clinical pointers for hydatid disease:
- Slow-growing hepatic cysts in a patient from a pastoral region (sheep-herding communities, contact with dogs) warrant serological testing and imaging
- Eosinophilia may be present but is neither sensitive nor specific
- Cyst rupture can be triggered by trauma, including biopsy — aspiration or biopsy of a suspected hydatid cyst without antiparasitic coverage and surgical backup is dangerous
- Diagnosis is made by imaging (ultrasound, CT) plus serology (ELISA for echinococcal antibodies)
8. Who Is Most at Risk
Tapeworm infections are strongly patterned by geography, sanitation, food practices, and animal husbandry, making epidemiological history one of the most useful diagnostic tools.
Geographic distribution:
- Taenia solium: Latin America (especially Mexico, Peru, Bolivia), sub-Saharan Africa, South and Southeast Asia, parts of Eastern Europe. Rare but not absent in US domestic cases; immigrant populations from endemic regions represent the largest burden in high-income countries.
- Taenia saginata: worldwide wherever beef is eaten raw or undercooked; highest prevalence in Ethiopia, the Middle East, Latin America, and Eastern Europe.
- Diphyllobothrium: Scandinavia, Finland, Russia, Japan, Chile, and North America where raw freshwater fish is consumed (sushi, ceviche, gravlax from freshwater species, lightly smoked fish).
- Hymenolepis nana: global, highest in children in tropical and subtropical regions, institutional settings, and areas with poor sanitation.
- Echinococcus granulosus: pastoral communities with close dog-sheep contact worldwide; Mediterranean, Middle East, Central Asia, South America, sub-Saharan Africa, Australia.
Behaviors and exposures that increase risk:
- Eating raw or undercooked pork, beef, or freshwater fish
- Poor hand hygiene, particularly in households with a known tapeworm carrier
- Living in or traveling to areas with inadequate sanitation and open defecation
- Using human feces as agricultural fertilizer (night soil) on crops eaten raw
- Close contact with dogs in areas endemic for Echinococcus
- Immunosuppression (HIV, corticosteroids, chemotherapy) — increases risk of H. nana hyperinfection and may unmask or accelerate Echinococcus progression
Immigration and travel medicine: New-onset seizures in a person from Latin America, sub-Saharan Africa, or South Asia should prompt consideration of NCC. The incubation period for neurocysticercosis (time from egg ingestion to symptomatic cyst) is typically 1–5 years, so symptoms may develop long after the exposure occurred.
Key Research Papers
Peer-reviewed studies, systematic reviews, and clinical guidelines on tapeworm disease in humans. The year/volume/pages link opens the PubMed record.
- Garcia HH, Gonzalez AE, Evans CAW, Gilman RH. Taenia solium Cysticercosis. The Lancet. Search PubMed [PubMed PMID 17269187]
- Nash TE, Garcia HH. Diagnosis and Treatment of Neurocysticercosis. Nature Reviews Neurology. Search PubMed [PubMed PMID 21572778]
- White AC Jr, Coyle CM, Rajshekhar V, et al. Diagnosis and Treatment of Neurocysticercosis: 2017 Clinical Practice Guidelines. Clinical Infectious Diseases. Search PubMed [PubMed PMID 28260308]
- Del Brutto OH, Nash TE, White AC Jr, et al. Revised Diagnostic Criteria for Neurocysticercosis. Journal of the Neurological Sciences. Search PubMed [PubMed PMID 22900875]
- Ndimubanzi PC, Carabin H, Budke CM, et al. A Systematic Review of the Frequency of Neurocysticercosis with a Focus on People with Epilepsy. PLoS Neglected Tropical Diseases. Search PubMed [PubMed PMID 23079626]
- Scholz T, Garcia HH, Kuchta R, Wicht B. Update on the Human Broad Tapeworm (Diphyllobothrium), Including Clinical Relevance. Clinical Microbiology Reviews. Search PubMed [PubMed PMID 24528876]
- Gripper LB, Welburn SC. Neurocysticercosis Infection and Disease — A Review. Acta Tropica. Search PubMed [PubMed PMID 26272177]
- Brunetti E, Kern P, Vuitton DA. Expert Consensus for the Diagnosis and Treatment of Cystic and Alveolar Echinococcosis in Humans. Acta Tropica. Search PubMed [PubMed PMID 15929899]
- Coyle CM, Mahanty S, Zunt JR, et al. Neurocysticercosis: Neglected but Not Forgotten. PLoS Neglected Tropical Diseases. Search PubMed [PubMed PMID 22030207]
- Carabin H, Ndimubanzi PC, Budke CM, et al. Clinical Manifestations Associated with Neurocysticercosis: A Systematic Review. PLoS Neglected Tropical Diseases. Search PubMed [PubMed PMID 25023047]
Live PubMed Searches
Each link opens a live PubMed query so results stay current as new papers are indexed.
- Taenia solium taeniasis symptoms
- Neurocysticercosis seizures
- Diphyllobothrium vitamin B12 deficiency
- Cysticercosis brain cysts MRI
- Echinococcus hydatid disease
- Hymenolepis nana in children
- Tapeworm proglottid diagnosis
- Taeniasis cysticercosis epidemiology
- Neurocysticercosis in immigrants
Connections
- Tapeworm Hub
- Intestinal Tapeworm Symptoms
- Neurocysticercosis — Brain Cysts
- Diagnosis — Imaging & Serology
- Tapeworm Treatments
- Praziquantel & Albendazole
- Neurocysticercosis Treatment
- Prevention & Food Safety
- Parasites
- Acanthamoeba
- Giardia
- Malaria
- Toxoplasma
- Neurology
- Infectious Disease
- Lab Tests