Diagnosing Tapeworm — Imaging, Serology, and Stool Microscopy
- Diagnostic Challenge
- Stool Microscopy for Intestinal Tapeworm
- ELISA Serology
- MRI
- CT Scan
- EITB Western Blot
- CSF Analysis in Meningeal NCC
- Echinococcus (Hydatid) Diagnosis
- Revised Diagnostic Criteria for NCC
- Key Research Papers
- PubMed Searches
- Connections
Diagnostic Challenge
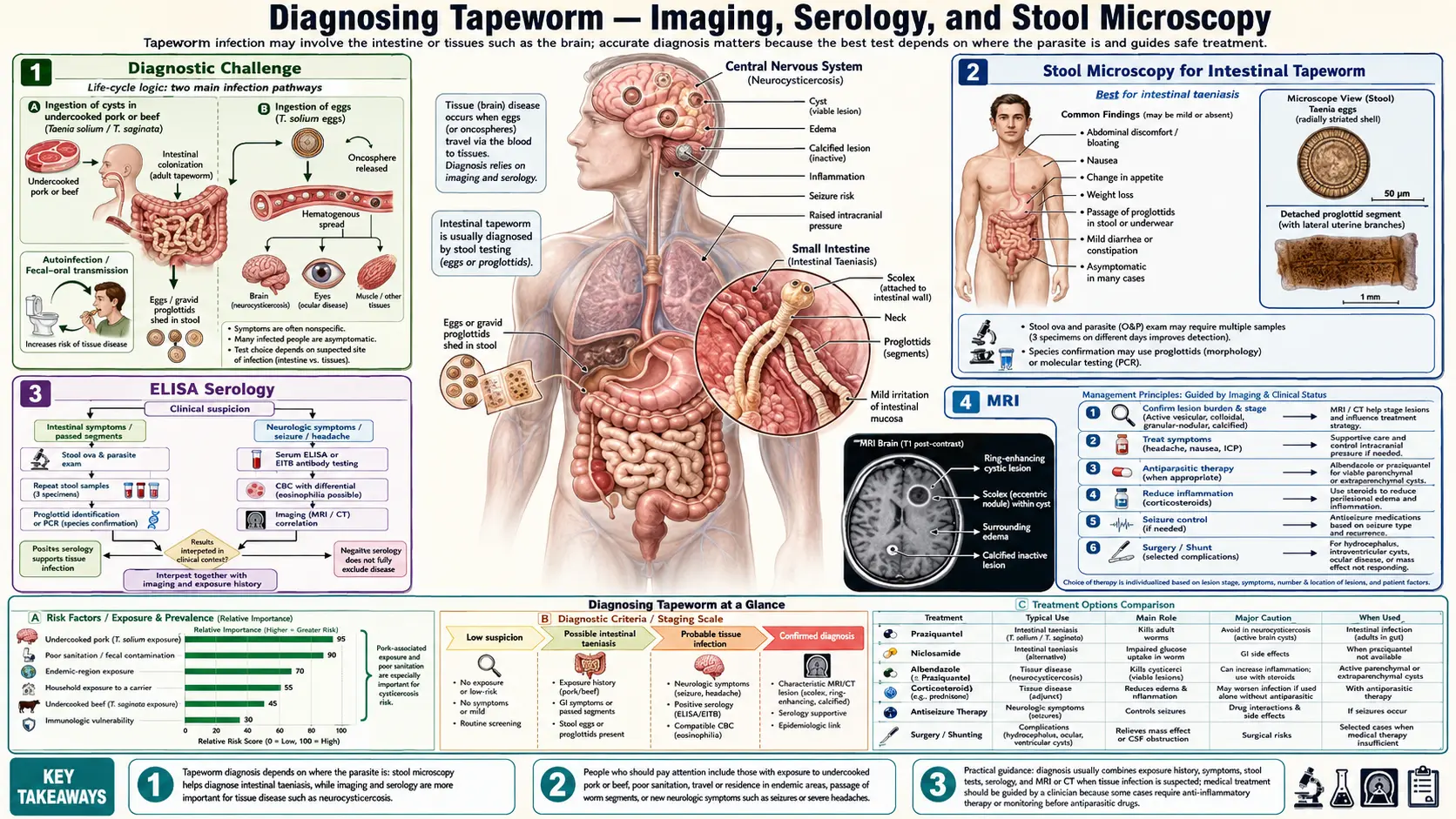
Diagnosing tapeworm infections is deceptively difficult because the clinical picture varies enormously depending on which species is involved and whether the infection is limited to the intestine or has invaded tissues. A person with an intestinal tapeworm (Taenia saginata, T. solium, or Diphyllobothrium latum) may have only vague abdominal symptoms — or no symptoms at all — and simply notice segments passing in stool. By contrast, T. solium infection carries additional public health significance: an intestinal carrier sheds eggs that can cause neurocysticercosis (NCC) in household contacts and in themselves through autoinfection.
In the brain, NCC mimics a long list of other conditions: epilepsy of unknown cause, brain tumor (the ring-enhancing lesion of a degenerating cyst is often mistaken for a primary or metastatic malignancy), brain abscess, tuberculoma, and toxoplasma encephalitis. Distinguishing NCC from these other diagnoses — or from other parasitic infections like cerebral toxocariasis or cerebral echinococcosis — has major treatment implications. Getting the species right also matters: identifying intestinal T. solium (not T. saginata) triggers contact screening, because household contacts of T. solium carriers are at risk for NCC.
Diagnosis of tapeworm infection therefore requires combining clinical history (travel history, dietary habits, symptoms), stool examination (microscopy, antigen tests), serology (antibody and antigen detection), and neuroimaging (CT, MRI) in a systematic approach tailored to the suspected species and disease stage.
Stool Microscopy for Intestinal Tapeworm
Stool examination remains the foundation of diagnosing intestinal tapeworm infections, though it has significant limitations in sensitivity and specificity.
Ova and parasite (O&P) examination: A standard O&P exam involves concentration of stool (formalin-ethyl acetate sedimentation or flotation) and examination under light microscopy. Taenia eggs are 30–40 μm, round, with a thick striated outer shell, and contain an oncosphere with six hooks. Critically, T. solium and T. saginata eggs are morphologically identical under microscopy — species identification requires proglottid examination.
Proglottid examination: Gravid proglottids (segments containing eggs) are passed in stool or noticed by patients in their underwear. They are flat, white or yellowish, and motile when fresh. Species identification: T. saginata proglottids have 15–20 main uterine branches on each side; T. solium proglottids have 7–12 uterine branches. This distinction is critical because T. solium requires immediate treatment and household contact screening for NCC risk.
Sensitivity limitations: Tapeworm eggs may not be present in every stool sample — adult tapeworms shed proglottids intermittently, and eggs within intact proglottids may not be released into free stool. Multiple stool samples collected on different days increase sensitivity. Perianal tape test (pressing sticky tape to the anal region, then examining under microscopy) improves egg detection for T. saginata, analogous to the method used for pinworm.
Modified acid-fast staining: Not used for Taenia but important for Echinococcus in stool when protoscoleces are shed (rare, only in patients with ruptured or communicating hydatid cysts). Also used to differentiate Cryptosporidium and Cyclospora oocysts from tapeworm eggs in mixed helminth-protozoa co-infections.
ELISA Serology
Enzyme-linked immunosorbent assay (ELISA) for tapeworm diagnosis detects either antibodies in patient serum (indicating exposure) or parasite antigens in serum or stool (indicating active infection). Each has distinct clinical utility.
Antibody ELISA: Measures IgG antibodies against Taenia or Echinococcus antigens. For NCC, antibody tests suffer from cross-reactivity between T. solium and other Taenia species, and between Taenia and Echinococcus. Additionally, antibodies persist long after the infection has resolved, limiting utility for distinguishing active from past infection. Antibody ELISA is best used as an initial screen in suspected NCC, with confirmation by EITB Western blot.
Coproantigen ELISA: Detects Taenia antigens in stool. More sensitive than microscopy for detecting intestinal tapeworm carriers (particularly T. solium carriers who may pass few or no intact proglottids). Sensitivity approximately 95% for active tapeworm infection; specificity near 99%. Species-level identification is possible with monoclonal antibody-based assays. An excellent test for the tapeworm carrier identification programs that protect household contacts from NCC.
Serum antigen ELISA (HP10 and B158/B60 assays): Detects circulating Taenia larval antigens shed by live cysts. Particularly useful for monitoring treatment response in NCC — antigen levels drop after successful antiparasitic therapy and cyst resolution. Also useful in extraparenchymal NCC where serology may be more sensitive than in single-lesion parenchymal NCC. Antigen assays are more sensitive in patients with viable cysts than in those with calcified (dead) cysts.
MRI
Magnetic resonance imaging is the gold standard diagnostic modality for active NCC, providing unmatched detail on cyst viability, stage, location, and the host inflammatory response.
Sequence selection: A complete NCC MRI protocol includes T1, T2, FLAIR, gadolinium-enhanced T1, and ideally T2* (GRE or SWI for calcifications) and CISS/FIESTA sequences (for ventricular cysts and cisternography).
Pathognomonic finding — the "hole-with-dot" sign: On T2-weighted imaging, a viable cysticercus appears as a round or oval hyperintense (CSF-isointense) cyst with a small hypointense eccentric dot — the scolex. This finding is pathognomonic for viable NCC when present. The scolex may not be visible in all cysts (dependent on cyst size, orientation, and MRI field strength), but when seen it provides definitive diagnosis without need for further confirmation.
Ring enhancement: Post-gadolinium T1 imaging shows thick, irregular ring enhancement around degenerating (colloidal stage) cysts. The enhancement reflects breakdown of the blood-brain barrier at the host-parasite interface during active inflammation. Ring enhancement in NCC is often "target-like" — an outer ring of edema, a ring of enhancing inflamed tissue, and a central degenerating cyst. This must be distinguished from the thin, smooth ring enhancement of a brain abscess and the thick, nodular enhancement of a glioblastoma.
FLAIR for edema: FLAIR sequences highlight perilesional edema (bright signal) that is not apparent on T2. Extensive perilesional FLAIR hyperintensity correlates with clinical severity and guides corticosteroid dosing.
Ventricular and subarachnoid cysts: Standard T2 may miss ventricular cysts that are isointense to CSF. CISS or FIESTA sequences (heavily T2-weighted fast spin echo with flow compensation) provide excellent contrast between cyst walls and CSF, making ventricular and subarachnoid cysts visible. Gadolinium CISS can show the ependymal or pial reaction around the cyst.
Limitations: MRI is relatively insensitive for calcified NCC — calcium appears hypointense on T2 and is easily missed unless SWI or GRE sequences are included. CT remains superior for detecting calcifications.
CT Scan
Computed tomography (CT) plays a complementary and sometimes primary role in NCC diagnosis, particularly in resource-limited endemic settings where CT is more widely available and affordable than MRI.
Calcified NCC — CT's strength: End-stage calcified NCC lesions are dense hyperdense foci on non-contrast CT, typically 2–10 mm in diameter, often multiple, scattered in cortex and subcortical white matter. CT is significantly more sensitive than standard MRI sequences (T1, T2, FLAIR) for detecting these calcifications. Importantly, calcified lesions can still be associated with perilesional edema (PECNCC — perilesional edema in calcified NCC) even years after the acute infection, and CT can miss this edema; MRI FLAIR is needed when PECNCC is suspected in a patient with recurrent seizures and known calcified NCC.
Ring-enhancing lesions: On contrast-enhanced CT, degenerating (colloidal stage) cysts appear as ring-enhancing lesions indistinguishable by CT alone from brain abscess, tuberculoma, or metastases. Clinical context (age, travel history, dietary history, serology) and MRI are needed to narrow the diagnosis.
Acute obstructive hydrocephalus: CT is the fastest imaging modality for evaluating hydrocephalus and is the first-line study in any patient with signs of raised ICP and suspected NCC. Ventricular enlargement, effacement of sulci, and transependymal edema (periventricular hypodensity) on CT indicate obstructive hydrocephalus requiring urgent neurosurgical management.
Practical role in endemic settings: CT remains the most widely used neuroimaging modality in countries where NCC is endemic (sub-Saharan Africa, Latin America, South/Southeast Asia). A CT showing multiple calcifications in a young adult with seizures in an endemic region is strongly suggestive of NCC even without serology.
EITB Western Blot
The enzyme-linked immunoelectrotransfer blot (EITB) — also known as the western blot for cysticercosis — is the serological gold standard for confirming NCC diagnosis. It was developed by the CDC and has been validated in multiple large studies.
Principle: EITB separates T. solium glycoprotein antigens by molecular weight on polyacrylamide gels, transfers them to nitrocellulose membranes, and then probes the membrane with patient serum. Patient antibodies bind to specific antigen bands. The assay uses a lentil lectin-purified glycoprotein antigen (LLGP) preparation containing 7 diagnostic bands at molecular weights of 50/42, 42/39/24/21/18/14 kDa.
Performance: Sensitivity 94–98% in patients with 2+ viable cysts; specificity near 100% when 2+ bands are present. One band alone is considered indeterminate — not definitive evidence of NCC.
Limitations in single lesion NCC: Sensitivity drops substantially for solitary enhancing granulomas (single-lesion parenchymal NCC) — approximately 28–50% in published studies. A negative EITB does not rule out NCC when clinical and radiological evidence is strong. Single-lesion NCC may not trigger a sufficient antibody response to reach the EITB detection threshold.
CSF vs serum: EITB performed on serum is at least as sensitive as on CSF for parenchymal NCC. CSF serology is sometimes superior in extraparenchymal NCC (subarachnoid or ventricular NCC), where serum may be negative. CSF EITB should be requested in suspected NCC with negative serum EITB and strong clinical/imaging evidence.
Use in endemic countries: EITB is available at reference laboratories in the US (CDC) and at selected laboratories in Latin America. Access in sub-Saharan Africa and South Asia is limited, making clinical and imaging-based diagnosis the practical standard in many endemic settings.
CSF Analysis in Meningeal NCC
Lumbar puncture and cerebrospinal fluid (CSF) analysis is most useful when subarachnoid, meningeal, or racemose NCC is suspected — situations where the inflammation extends into the CSF space. It is not routinely required for uncomplicated parenchymal NCC.
Cell count and differential: Meningeal NCC produces a pleocytosis, typically lymphocyte-predominant (10–500 cells/μL). CSF eosinophilia — usually defined as >10% of the differential — is suggestive of parasitic meningitis and occurs in a subset of NCC patients with subarachnoid disease. CSF eosinophilia is not specific for NCC; other helminths (Angiostrongylus, Baylisascaris, Gnathostoma, Trichinella) and fungal infections (Coccidioides) can produce it.
Protein: CSF protein is elevated (typically 45–200 mg/dL) in active meningeal NCC, reflecting the breakdown of the blood-CSF barrier in the inflamed subarachnoid space. Markedly elevated protein (>200 mg/dL) suggests severe arachnoiditis.
Glucose: Usually normal or mildly low. Severe hypoglycorrhachia (very low CSF glucose) is uncommon in NCC and should raise suspicion for co-existing bacterial or fungal meningitis.
CSF serology: As noted above, EITB on CSF has higher sensitivity than serum EITB in extraparenchymal NCC. Antigen detection assays (HP10) in CSF can quantify the parasite burden and monitor treatment response.
When NOT to do lumbar puncture: Lumbar puncture is contraindicated when obstructive hydrocephalus is present (risk of herniation). CT or MRI must be obtained first to rule out mass effect and ventricular obstruction in any patient with suspected meningeal NCC and signs of raised ICP before lumbar puncture is performed.
Echinococcus (Hydatid) Diagnosis
Echinococcus is a different tapeworm genus that causes hydatid disease — cysts in liver, lung, brain, and other organs — through an entirely different lifecycle (dogs are the definitive host; sheep, cattle, and humans are intermediate hosts). Diagnosis overlaps with but is distinct from Taenia/NCC diagnosis.
Liver ultrasound — WHO classification: The liver is the most common site of cystic echinococcosis (CE, caused by E. granulosus). Ultrasound is the first-line imaging modality and can classify cysts by the WHO/Gharbi system: CE1 (simple cyst, active), CE2 (multiseptated "honeycomb," active), CE3a (water lily sign — detached germinal layer, transitional), CE3b (heterogeneous with daughter cysts, transitional), CE4 (heterogeneous matrix, inactive), CE5 (calcified wall, inactive). The WHO classification guides treatment — active cysts (CE1-2) are treated, transitional cysts require individualization, and inactive cysts (CE4-5) may be monitored.
Pathognomonic signs: The most specific ultrasound finding is the "daughter cyst within mother cyst" pattern (CE2), where multiple small daughter cysts are visible within the main cyst cavity. The "water lily sign" (CE3a) shows a detached germinal membrane floating within clear cyst fluid. These findings are essentially diagnostic without serology.
Serology: ELISA (using crude hydatid fluid antigen or recombinant antigen B) combined with indirect hemagglutination (IHA) provides sensitivity of 80–90% for hepatic CE. Sensitivity is lower for pulmonary (60–70%) and cerebral/splenic CE (40–50%). False positives occur with other helminthiases (Taenia, Toxocara) and liver pathology. Cross-reactive antibodies between E. granulosus and E. multilocularis limit species differentiation by serology alone.
PCR and species identification: PCR on cyst fluid or puncture aspirate material can identify Echinococcus to species level (E. granulosus vs E. multilocularis) — important for prognosis (alveolar echinococcosis from E. multilocularis is far more aggressive and invasive) and treatment duration.
Revised Diagnostic Criteria for NCC (Del Brutto 2017)
The Del Brutto criteria, originally published in 2001 and revised in 2017, provide a systematic, evidence-based framework for assigning NCC diagnostic certainty. They are the internationally accepted standard for research and clinical practice.
Criteria categories:
- Absolute criteria: Histopathological demonstration of the parasite in biopsy; cystic lesion with scolex on CT/MRI (the "hole-with-dot" sign); direct visualization of subretinal parasite on fundoscopy.
- Major criteria: Any lesion highly suggestive of NCC on neuroimaging (cystic lesion without scolex, uni- or multilobular cystic lesions in subarachnoid space, enhancing lesion or disc-like calcification compatible with NCC); positive EITB or validated ELISA using whole glycoprotein fraction in serum; resolution of cystic lesions spontaneously or after antiparasitic drugs; history of cysticercosis outside the CNS.
- Minor criteria: Non-pathognomonic lesions suggestive of NCC (single enhancing lesions, solitary calcifications); other compatible neuroimaging findings; clinical manifestations suggestive of NCC (seizures, focal deficits, elevated ICP); positive CSF-EITB or validated ELISA; exposure in an endemic area.
- Epidemiological criteria: Living in endemic area; frequent travel to endemic area; household contact with T. solium infection.
Diagnostic levels:
- Definitive NCC: 1 absolute criterion OR 2 major + any minor + any epidemiological criteria OR 1 major + 3 minor criteria OR 1 major + 1 minor + 1 epidemiological criterion (if EITB is the major criterion).
- Probable NCC: 1 major + 2 minor OR 1 minor + 1 epidemiological criterion.
- Possible NCC: 1 minor only or nonspecific findings with strong epidemiological evidence.
These criteria guide treatment decisions — definitive and probable NCC warrant antiparasitic treatment (when appropriate for lesion stage), while possible NCC may be observed or treated empirically depending on clinical context.
Key Research Papers
- Del Brutto OH et al. Revised diagnostic criteria for neurocysticercosis. J Neurol Sci. Search PubMed [PubMed PMID 28260308]
- Garcia HH et al. Neurocysticercosis. Lancet. Search PubMed [PubMed PMID 17269187]
- Nash TE et al. Treatment of neurocysticercosis: current status and future research needs. Neurology. Search PubMed [PubMed PMID 23079626]
- Garcia HH et al. A trial of antiparasitic treatment to reduce the rate of seizures due to cerebral cysticercosis. N Engl J Med. Search PubMed [PubMed PMID 21572778]
- Carpio A et al. Neurocysticercosis: new knowledge, new doubts. Curr Neurol Neurosci Rep. Search PubMed [PubMed PMID 25023047]
- Bhatt GC et al. Cysticercosis and Neurocysticercosis. Pediatr Clin North Am. Search PubMed [PubMed PMID 22900875]
- Garcia HH et al. Taenia solium cysticercosis. Lancet. Search PubMed [PubMed PMID 24528876]
- Rajshekhar V et al. Solitary cysticercus granuloma: the commonest cause of focal seizures in patients from a developing country. Neurology. Search PubMed [PubMed PMID 15929899]
- White AC et al. Diagnosis and treatment of neurocysticercosis: 2017 clinical practice guidelines by IDSA and ASTMH. Clin Infect Dis. Search PubMed [PubMed PMID 22030207]
- Fleury A et al. High prevalence of calcified silent neurocysticercosis in a rural village of Mexico. Neuroepidemiology. Search PubMed [PubMed PMID 26272177]
PubMed Searches
- Neurocysticercosis diagnosis MRI CT imaging
- Tapeworm stool microscopy ova and parasite exam
- Cysticercosis EITB western blot serology
- Echinococcus hydatid cyst ultrasound diagnosis WHO classification
- Del Brutto diagnostic criteria neurocysticercosis 2017
Connections
- All Parasites
- Tapeworm Overview
- Tapeworm Symptoms Hub
- Intestinal Tapeworm Symptoms
- Neurocysticercosis — Brain Cysts
- NCC Treatment
- Praziquantel and Albendazole
- All Tapeworm Treatments
- Lab Tests