Complex Regional Pain Syndrome (CRPS)
- What is CRPS?
- Type I vs. Type II: What's the Difference?
- The History: From RSD to CRPS
- Causes and Pathophysiology
- Budapest Criteria: How CRPS is Diagnosed
- Stages and Progression
- Conventional Treatment
- Mirror Therapy and Graded Motor Imagery
- Low-Dose Naltrexone
- Natural and Lifestyle Approaches
- Complications
- Key Research Papers
- Connections
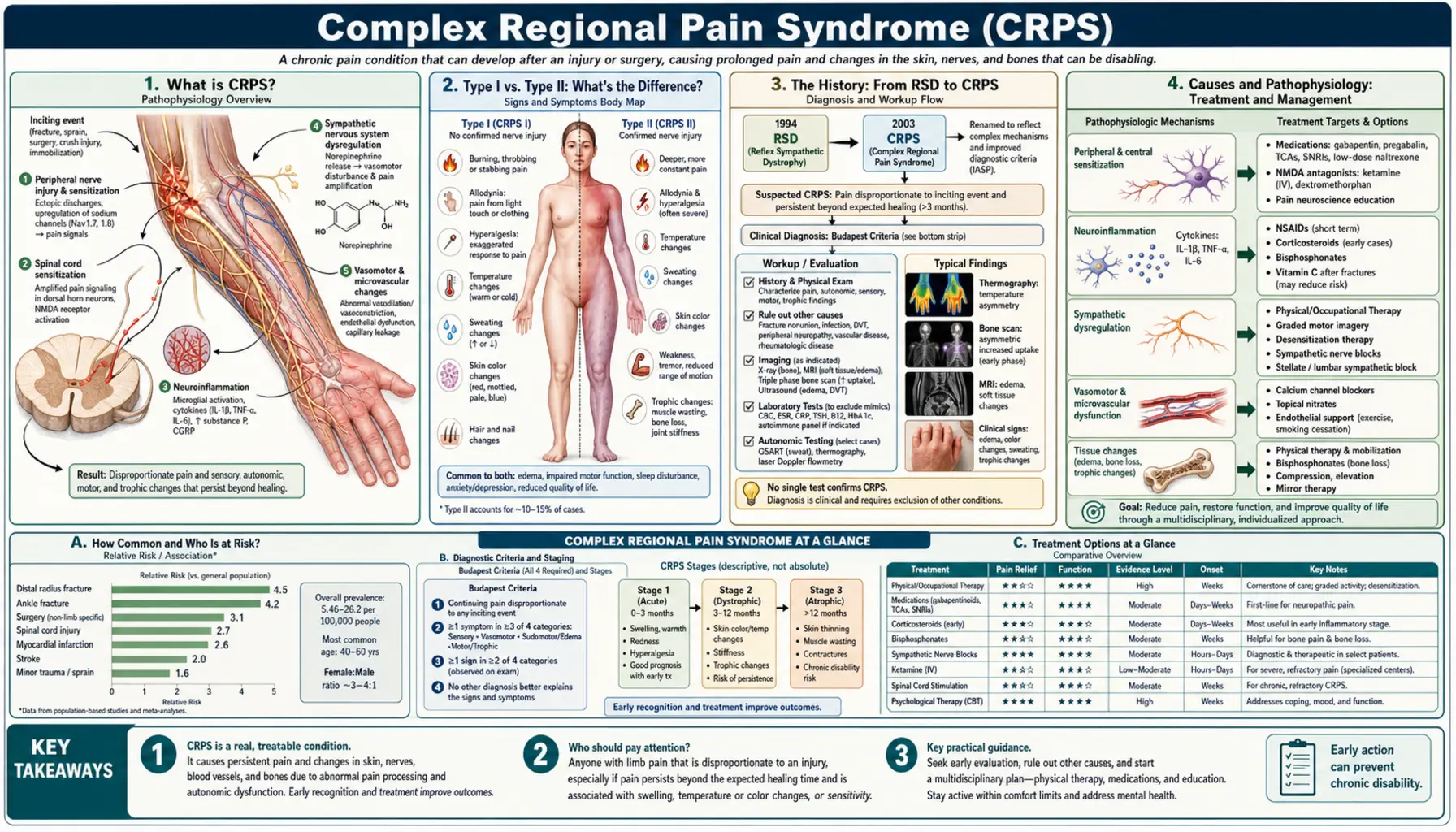
What is CRPS?
Complex Regional Pain Syndrome (CRPS) is a chronic pain condition characterized by severe, out-of-proportion pain — usually in a limb (arm, leg, hand, or foot) — along with abnormal changes in skin color, temperature, and texture, and autonomic nervous system dysfunction. Pain is typically burning or aching and disproportionate to any observable tissue injury.
CRPS develops after an initiating event (injury, surgery, or occasionally spontaneously) but then takes on a life of its own, independent of the original injury healing. It affects about 200,000 people in the US annually. Women are 3–4 times more affected than men. Onset most commonly occurs after a fracture or sprain, particularly of the wrist (Colles' fracture is a classic trigger) or ankle.
Type I vs. Type II: What's the Difference?
CRPS Type I (formerly Reflex Sympathetic Dystrophy, RSD): No confirmed nerve damage. Pain and symptoms arise without identifiable nerve injury — the nervous system has essentially "gone wrong" on its own. This is by far the more common form (~90% of cases). The mechanisms involve peripheral and central sensitization, neuroinflammation, and sympathetic nervous system dysregulation.
CRPS Type II (formerly Causalgia): Occurs after a confirmed, identifiable nerve injury (e.g., from surgery, laceration, or crush injury). The distribution of pain and symptoms follows the injured nerve's territory. Despite having a confirmed nerve cause, treatment approaches overlap significantly with Type I.
In practice, both types cause the same constellation of signs and symptoms and are managed similarly.
The History: From RSD to CRPS
CRPS has been recognized since the American Civil War, when surgeon Silas Weir Mitchell described "causalgia" — burning pain in soldiers after peripheral nerve injuries. The term Reflex Sympathetic Dystrophy (RSD) dominated for decades and implied that an overactive sympathetic nervous system was always responsible.
However, research showed that sympathetically independent pain is common in CRPS, and the "reflex" and "sympathetic" terminology was misleading. In 1994, the International Association for the Study of Pain (IASP) renamed the condition Complex Regional Pain Syndrome. Many patients and advocacy groups still use the terms RSD and CRPS interchangeably.
Causes and Pathophysiology
CRPS develops when the normal healing process goes wrong in multiple systems simultaneously. Key mechanisms:
- Peripheral sensitization: Damaged tissues release inflammatory mediators (substance P, CGRP, bradykinin, nerve growth factor) that lower the pain threshold in local nociceptors — they fire with less stimulation.
- Central sensitization: The spinal cord and brain rewire in response to persistent peripheral input; pain signals are amplified and persist even after peripheral healing.
- Neuroinflammation: Pro-inflammatory cytokines (TNF-α, IL-1β, IL-6) remain chronically elevated in the affected limb; neuropeptides cause ongoing vasodilation and tissue changes.
- Sympathetic-sensory coupling: Sympathetic nerve fibers grow abnormal sprouts around dorsal root ganglion neurons, creating cross-talk that did not exist before — this is why emotional stress and temperature changes provoke CRPS pain.
- Cortical reorganization: The brain region representing the affected limb in the somatosensory cortex shrinks and reorganizes — which is why mirror therapy and graded motor imagery work.
Budapest Criteria: How CRPS is Diagnosed
There is no blood test or imaging finding that confirms CRPS. Diagnosis is clinical, based on the 2003 Budapest Criteria (validated and used worldwide). The patient must meet all of the following:
- Continuing pain disproportionate to any inciting event.
- Reports of at least one symptom in 3 of 4 categories: sensory (allodynia/hyperalgesia), vasomotor (temperature/color changes), sudomotor/edema (swelling, sweating), motor/trophic (weakness, tremor, nail/hair/skin changes).
- Displays at least one sign in 2 or more categories at the time of evaluation.
- No other diagnosis better explains the symptoms.
Supportive testing: three-phase bone scan (hot spots in early CRPS); skin temperature asymmetry greater than 1°C; X-ray (patchy osteoporosis in chronic CRPS); MRI (bone marrow edema pattern).
Stages and Progression
The traditional three-stage model (Stage 1: acute — warm, red, painful; Stage 2: dystrophic — cooling, mottled, stiffening; Stage 3: atrophic — cold, pale, wasted muscle) is now considered an oversimplification. CRPS does not progress in a linear, predictable fashion. Many patients plateau or partially recover at any point. Some cases spontaneously remit, especially pediatric cases. Longer duration without treatment predicts worse outcomes.
Conventional Treatment
A multimodal approach is required — no single treatment works alone:
- Physical and occupational therapy: The cornerstone. Graded exposure, desensitization, edema control, range-of-motion exercises, mirror therapy, and graded motor imagery. Early mobilization is critical.
- Medications: Gabapentin/pregabalin (reduce central sensitization); tricyclic antidepressants (amitriptyline — neuropathic pain and sleep); SNRIs (duloxetine); low-dose naltrexone (LDN — see dedicated section); corticosteroids (short course in acute CRPS only); ketamine infusions (NMDA receptor antagonist — used in refractory cases at specialized centers); calcitonin (addresses bone pain and osteoporosis component); bisphosphonates (pamidronate/alendronate — evidence in chronic CRPS).
- Interventional procedures: Sympathetic nerve blocks (stellate ganglion for upper extremity, lumbar sympathetic for lower extremity); spinal cord stimulation (SCS) — FDA-approved, shown to reduce pain 50% and improve quality of life in multiple RCTs; intrathecal drug delivery.
- Psychological interventions: CBT, acceptance and commitment therapy (ACT), pain neuroscience education — essential components of comprehensive care.
Mirror Therapy and Graded Motor Imagery
Two of the most evidence-supported non-invasive treatments for CRPS — both targeting the brain's representation of the affected limb.
Mirror therapy: A box with a mirror placed vertically in the patient's midline. The unaffected limb performs exercises and is reflected in the mirror while the affected limb is hidden. The brain receives visual feedback of a "normal" moving limb in the affected side's position — this retrains motor and sensory cortex representation. Best evidence is for hand/arm CRPS.
Graded Motor Imagery (GMI): A 3-stage program: (1) left/right limb recognition training (using smartphone apps showing photos — reactivates cortical lateralization); (2) imagined movements without actually moving; (3) mirror therapy. GMI addresses cortical reorganization step by step and is superior to either component alone in multiple RCTs.
Low-Dose Naltrexone
Naltrexone is an opioid receptor antagonist approved in standard doses (50 mg/day) for addiction. At low doses (1.5–4.5 mg/day, taken at bedtime), it paradoxically acts as an anti-inflammatory and neuroprotective agent by briefly blocking opioid receptors — causing a rebound increase in endorphin production (the endorphin upregulation hypothesis) — and most importantly by blocking TLR4 receptors on microglia, the brain's immune cells. This reduces microglial activation and neuroinflammation.
Case series, small trials, and patient reports support LDN's benefit in CRPS. A typical protocol: start at 1.5 mg/night, increase to 3 mg after 2 weeks, then to 4.5 mg if needed. Requires a compounding pharmacy (standard 50 mg tablets cannot be split accurately to these doses). Side effects are generally mild (vivid dreams for the first few weeks).
Natural and Lifestyle Approaches
- Vitamin C: 500–1000 mg/day for 50 days post-fracture or post-surgery reduces CRPS incidence by approximately 80% in multiple RCTs — this is a prevention intervention with strong evidence.
- Alpha-lipoic acid (ALA): 600 mg three times daily; reduces oxidative stress in neural tissue; evidence exists in diabetic neuropathy and emerging evidence in CRPS.
- Magnesium: An NMDA receptor modulator; reduces central sensitization; IV magnesium is used in some ketamine protocols; oral magnesium glycinate 300–400 mg/day is a reasonable adjunct.
- Swimming or hydrotherapy: Water provides gentle resistance and desensitization without weight-bearing; often the only tolerated exercise in early CRPS.
- Mindfulness-based stress reduction (MBSR): Reduces pain catastrophizing and central sensitization amplification; well-validated in chronic pain generally.
- Anti-inflammatory diet: A Mediterranean-pattern diet with an omega-3 emphasis may reduce neuroinflammation and support recovery.
Complications
Psychological: Depression affects approximately 50% of CRPS patients, along with anxiety and PTSD — all of which worsen pain and must be treated directly. Suicide risk is elevated in severe chronic CRPS.
Physical: Muscle atrophy and contractures from immobility; skin fragility; osteoporosis (especially in the affected limb); and spread to other limbs (approximately 35% of cases with severe CRPS eventually experience spread to additional limbs).
Social: Disability, job loss, and relationship strain from a condition that is often invisible and disbelieved by others — including medical professionals. CRPS in children and adolescents typically has a better prognosis with aggressive physical therapy and family-centered care.
Key Research Papers
- Harden RN, et al. Validation of proposed diagnostic criteria (the "Budapest Criteria") for complex regional pain syndrome. Pain. 2010. PMID: 20493633
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
PubMed Topic Searches
- complex regional pain syndrome treatment
- CRPS spinal cord stimulation
- mirror therapy CRPS RSD
- low dose naltrexone neuropathic pain
- vitamin C CRPS prevention fracture
- graded motor imagery chronic pain
Connections
- Pain & Allergy
- Chronic Pain
- Neuropathic Pain
- Migraine
- Complex Regional Pain Syndrome (CRPS / RSD): the full deep dive — the longer chronic-pain treatment of the same condition, covering the Budapest criteria in detail, bisphosphonates, ketamine infusions, sympathetic blocks, spinal-cord stimulation, and vitamin C prophylaxis after wrist fracture.
- Fibromyalgia
- Depression
- Anxiety
- Vitamin C
- Magnesium