Epiretinal Membrane
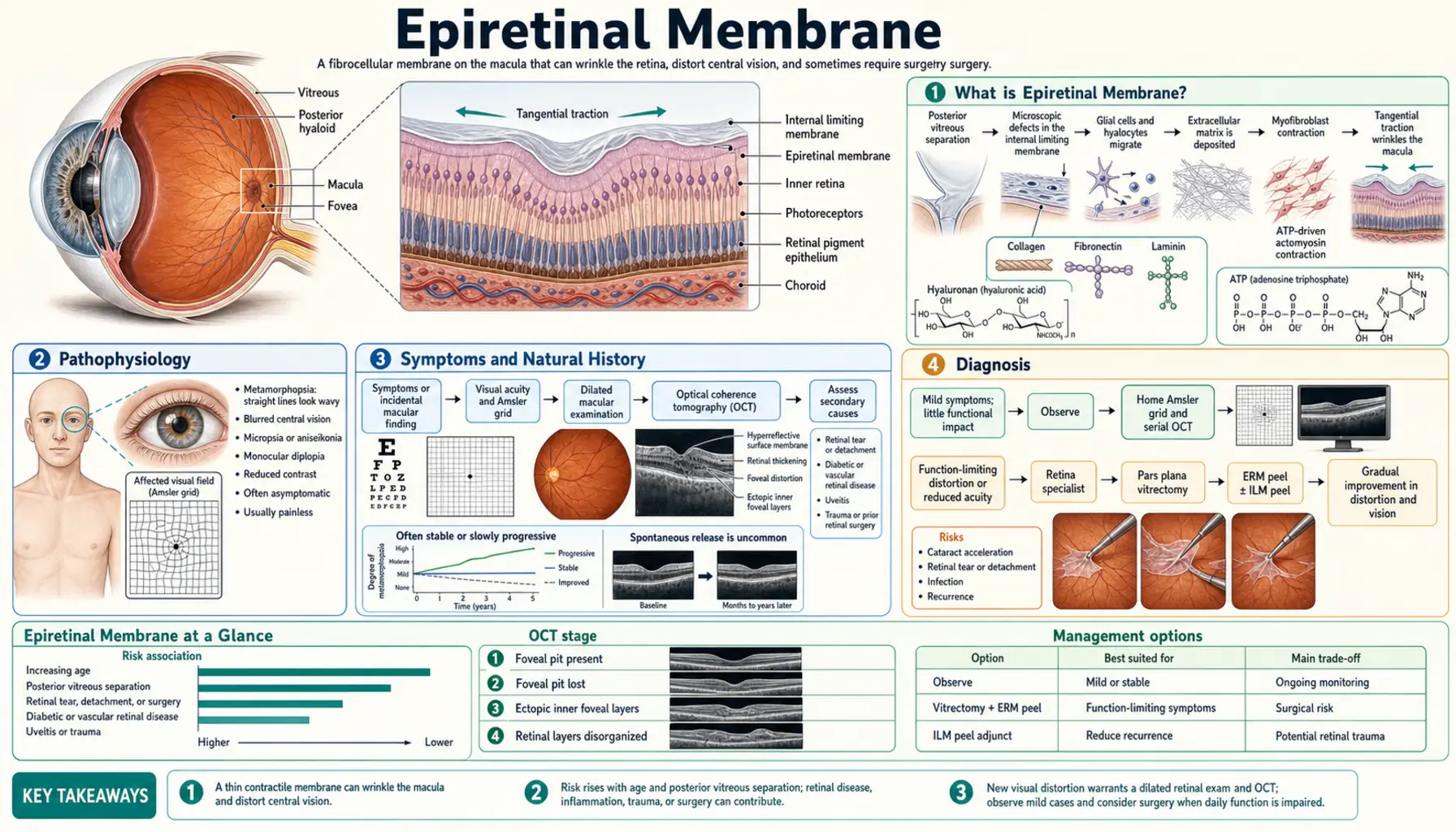
Epiretinal membrane (ERM) — also called macular pucker, cellophane maculopathy, or premacular fibrosis — is a thin fibrocellular layer that grows on the inner surface of the retina over the macula. It is common in adults over 60, often discovered incidentally, and ranges from a minor finding requiring only monitoring to a treatable cause of significant visual distortion. Surgical outcomes are excellent when intervention is timely.
- What is Epiretinal Membrane?
- Pathophysiology
- Symptoms and Natural History
- Diagnosis
- Grading and Classification
- Surgical Treatment — Vitrectomy + Membrane Peeling
- Prognosis and Outcomes
- Non-Surgical Management and Monitoring
- Nutrition and Eye Health Support
- Cautions and Considerations
- References and Research
- Connections
- Featured Videos
What is Epiretinal Membrane?
An epiretinal membrane is a thin, translucent-to-opaque sheet of fibrocellular tissue that develops on the inner surface of the retina, predominantly over the macula — the central, high-resolution region of the retina responsible for reading, face recognition, and fine detail. As the membrane contracts, it distorts the underlying retinal architecture, producing the visual distortion and blur that characterize the condition.
ERM goes by several names depending on how it is described:
- Macular pucker — describes the puckered, wrinkled appearance of the retina when the membrane contracts
- Cellophane maculopathy — used when the membrane is thin and translucent, like cellophane wrap over the macula, without causing significant wrinkling
- Premacular fibrosis — used when the membrane is thick, opaque, and fibrotic with prominent distortion
- Surface wrinkling retinopathy — older term in the literature
Prevalence
ERM affects approximately 7–12% of adults over age 60, rising to roughly 20% in those over 75. It is bilateral in 10–20% of cases. Most are asymptomatic discoveries on routine retinal examination or during evaluation for another ocular complaint.
Primary vs Secondary ERM
- Primary (idiopathic) ERM: No identifiable underlying cause. Posterior vitreous detachment (PVD) — the normal age-related separation of the vitreous gel from the retina — triggers a healing response in which glial cells (Müller cells, fibrous astrocytes) and other cell types migrate onto the inner limiting membrane and proliferate, forming the ERM. This accounts for ~75% of cases.
- Secondary ERM: Caused by a known retinal or ocular condition, including retinal tears, retinal detachment or detachment repair surgery, laser photocoagulation, cryotherapy, uveitis (intraocular inflammation), retinal vein occlusion, diabetic retinopathy, and ocular trauma.
Pathophysiology
The formation of an epiretinal membrane follows a reproducible cellular cascade, most commonly initiated by posterior vitreous detachment.
Step 1: Posterior Vitreous Detachment (PVD)
The vitreous humor — a gel filling the eye's central cavity — is attached to the retina at birth. With age, it undergoes syneresis (liquefaction) and progressively separates from the retinal surface. When separation occurs near the macula, microscopic breaks in the inner limiting membrane (ILM) allow retinal glial cells, retinal pigment epithelium (RPE) cells, hyalocytes (vitreous resident cells), fibrous astrocytes, and macrophages to migrate onto the retinal surface. PVD is therefore the essential initiating event in most idiopathic ERM.
Step 2: Cell Migration and Proliferation
The migrating cells settle on the inner limiting membrane and begin to proliferate. The cellular composition of the resulting membrane includes:
- Müller cells (the dominant retinal glial cell)
- Retinal pigment epithelium (RPE) cells
- Fibrous astrocytes
- Macrophages and monocytes
- Hyalocytes (vitreous-resident macrophage-like cells)
- Myofibroblasts (transdifferentiated from the above, acquiring contractile properties)
Step 3: Membrane Formation and Contraction
Cells lay down extracellular matrix proteins — collagen types I, II, and IV, fibronectin, laminin — forming a fibrocellular membrane. Critically, myofibroblasts within the membrane generate centripetal contractile forces. This pulls the underlying retina into folds and wrinkles, distorting the architecture of the macula and the geometry of the foveal pit (the depression at the macula's center responsible for 20/20 vision).
Resulting Visual Dysfunction
The mechanical distortion of the macula produces the characteristic symptoms: metamorphopsia (straight lines appear wavy), micropsia (objects appear smaller than normal), and reduced visual acuity from displacement of the photoreceptors from their optimal focal position. Unlike age-related macular degeneration, ERM does not destroy photoreceptors — the visual cells remain intact beneath the membrane, which is why surgical peeling can achieve substantial visual recovery even years after symptom onset.
Symptoms and Natural History
Common Symptoms
- Metamorphopsia: The hallmark symptom — straight lines (door frames, tiles, text lines) appear wavy, bent, or distorted. Detected with the Amsler grid.
- Blurred or hazy central vision: Difficulty reading, recognizing faces, or performing fine detail tasks.
- Micropsia: Objects in the affected eye appear smaller than in the fellow eye — due to photoreceptor displacement spreading them apart on the retina.
- Monocular diplopia: Rare; severe ERM can produce two overlapping images in one eye due to extreme retinal wrinkling.
- Gray or translucent area in central vision — less common than metamorphopsia.
Asymptomatic Cases
A significant proportion of ERM — particularly early or thin membranes (cellophane maculopathy stage) — cause no visual symptoms and are found only during routine dilated fundus examination or OCT imaging performed for other reasons. These require monitoring rather than intervention.
Natural History
ERM does not follow a uniform course:
- Approximately 50% remain stable for years without progression.
- Approximately 30% show slow, gradual progression in membrane thickness and visual symptoms over months to years.
- Approximately 15–20% show partial spontaneous improvement — thought to be due to partial membrane contraction pulling it away from the macula or partial lysis, though complete spontaneous resolution is rare.
Progression Risk Factors
- Thicker membrane on OCT at presentation
- Ectopic inner foveal layers (EIFL) — a specific OCT finding indicating photoreceptor disruption
- Secondary ERM (from retinal tears, RVO, diabetic retinopathy) — more aggressive than idiopathic
- Younger patients — tend to have more proliferative membranes
- Presence of hard exudates or retinal thickening at presentation
Diagnosis
Optical Coherence Tomography (OCT) — Gold Standard
OCT provides cross-sectional imaging of the retina at micron-level resolution and is the cornerstone of ERM diagnosis and monitoring. Key OCT findings include:
- A hyperreflective (bright) band on the inner retinal surface representing the membrane itself
- Loss of the normal foveal depression (foveal contour flattening or inversion)
- Retinal thickening at the macula
- Retinal folds and wrinkling of the inner layers
- Ectopic inner foveal layers (EIFL): Inner retinal layers pulled over the foveal center — a key prognostic OCT finding associated with worse visual outcomes and used in the Govetto grading system
Visual Acuity Testing
Standard Snellen chart testing quantifies vision loss. In early ERM, acuity may be 20/25 to 20/30. In moderate disease, 20/40 to 20/60. In severe ERM, 20/100 or worse. The threshold of 20/40 or worse with functional impact is commonly used to guide the decision to offer surgery.
Amsler Grid
A simple grid of horizontal and vertical lines viewed at reading distance with one eye covered. Distortion or waviness of the lines (metamorphopsia), missing areas, or blurring indicate macular disease. Cheap, reproducible, and excellent for both clinical screening and home monitoring between appointments. Best performed with reading glasses or appropriate near correction in good lighting.
Fluorescein Angiography (FA)
Intravenous dye study that illuminates retinal blood vessels and identifies areas of leakage, ischemia, or neovascularization. Used in ERM primarily to exclude other causes of central visual distortion — macular degeneration (wet form), diabetic macular edema, or retinal vein occlusion. Not required in straightforward idiopathic ERM.
Microperimetry
Maps the sensitivity of individual macular locations under direct retinal imaging, correlating functional loss with structural OCT findings. Used in research settings and for detailed preoperative and postoperative evaluation in complex cases.
OCT Angiography (OCTA)
Non-invasive imaging of the retinal vasculature, including assessment of the foveal avascular zone (FAZ). In ERM, the FAZ may be distorted or enlarged, correlating with visual outcome. Increasingly used alongside standard OCT.
Grading and Classification
OCT-Based Govetto Grading System
The most widely used contemporary classification system grades ERM by OCT morphology and correlates with visual prognosis:
- Stage 1: Ectopic inner foveal layers (EIFL) present; foveal contour maintained; retinal architecture largely preserved; visual acuity usually 20/40 or better.
- Stage 2: Loss of foveal contour; onset of retinal thickening; inner layers beginning to be displaced.
- Stage 3: Loss of foveal pit; significant macular thickening; inner and outer retinal layer disorganization beginning; visual acuity typically 20/50 to 20/100.
- Stage 4: Disorganization of inner retinal layers (DRIL); inner and outer layer boundaries disrupted; worst visual prognosis even after surgery.
Earlier stage at surgery is associated with better postoperative visual outcomes — a key argument for not waiting until advanced disease before offering surgery to motivated patients.
Gass Classification (Historical)
Described by J. Donald Gass based on biomicroscopic (slit-lamp) findings:
- Cellophane maculopathy (Grade 0): Thin, transparent, refractile membrane over the macula without retinal distortion. Asymptomatic or minimally symptomatic. Corresponds to early/Stage 1-2 Govetto.
- Preretinal macular fibrosis (Grade 1-2): Thicker, opaque, gray-white membrane with visible retinal folds and wrinkling. Corresponds to symptomatic Stage 2-4 Govetto.
OCT has largely replaced purely biomicroscopic grading in current clinical practice.
Surgical Treatment — Vitrectomy + Membrane Peeling
Surgical Indications
Surgery is appropriate when:
- Symptomatic metamorphopsia affecting daily functioning (reading, driving, work)
- Best-corrected visual acuity (BCVA) of 20/40 or worse attributable to the ERM
- Progressive worsening documented on serial OCT over 3–6 months
- Significant patient distress despite preserved VA (metamorphopsia can be disabling even at 20/30)
- OCT Stage 2 or above with functional complaints
Pars Plana Vitrectomy (PPV)
The standard surgical approach. Three tiny (23-, 25-, or 27-gauge) instrument ports are placed through the pars plana (the non-visual peripheral retina), avoiding the lens and retina. The vitreous gel is removed using a high-speed vitreous cutter, creating access to the retinal surface. Modern small-gauge (25g/27g) vitrectomy is sutureless, performed under local anesthesia with sedation, and takes 30–60 minutes.
ERM Peeling
The epiretinal membrane is grasped with microsurgical intraocular forceps and peeled off the retinal surface under high magnification. A key challenge is identifying the membrane's edge — surgeons use vital dyes to stain the membrane and improve visualization:
- Brilliant Blue G (BBG): Preferentially stains the internal limiting membrane (ILM); well-tolerated; currently the preferred vital dye due to favorable safety profile.
- Indocyanine green (ICG): Historically used but carries a dose-dependent phototoxicity risk to the retinal pigment epithelium and photoreceptors — less favored in current practice unless BBG is unavailable.
Internal Limiting Membrane (ILM) Peeling
After ERM peeling, many surgeons perform concurrent ILM peeling — removing the thin basement membrane that sits between the retina and the vitreous cavity. Rationale: the ILM can serve as a scaffold for residual or new membrane cells to repopulate, driving ERM recurrence. ILM peeling reduces recurrence from ~10% without ILM peel to ~1–2% with ILM peel. The trade-off is a slightly higher rate of microperimetry-detected paracentral sensitivity deficits — representing subclinical Müller cell disruption — though most patients do not notice this clinically.
Cataract Formation After Vitrectomy
Nuclear sclerotic cataract (lens clouding) develops in nearly all phakic (natural-lens) patients after vitrectomy, typically within 1–2 years. Options:
- Combined vitrectomy + phacoemulsification cataract surgery: One procedure; preferred in patients over 60 with any pre-existing lens opacity.
- Sequential surgery: ERM peeling first; planned cataract surgery 6–12 months later; preferred in younger patients with clear lenses.
Surgical Outcomes
- 80–90% of patients see visual acuity improvement after ERM surgery
- Mean gain: 2–3 Snellen lines at 12 months
- Metamorphopsia improvement lags behind VA improvement: functional recovery continues for up to 2 years as the macula gradually "unfolds"
- Face-down positioning is not required after ERM peeling (unlike macular hole surgery)
- Gas or silicone oil tamponade is rarely used in uncomplicated ERM surgery
Prognosis and Outcomes
Visual Acuity Recovery
Most studies report mean postoperative visual acuity improvement of 2–3 Snellen lines at 1 year. Approximately 80–90% of operated eyes show some improvement; fewer than 5% worsen. The best predictor of postoperative VA is preoperative VA — patients with better vision at surgery tend to achieve better vision afterward, reinforcing the argument for earlier rather than later intervention once symptoms are functionally limiting.
Metamorphopsia Recovery
Distortion recovers more slowly than VA and is less predictable. At 6 months, 60–70% of patients report improved metamorphopsia. Most continued improvement occurs up to 24 months. Some degree of residual distortion persists in 20–30% of patients even after successful ERM removal, reflecting structural changes to the photoreceptor layer that persist after the membrane is peeled.
Factors Predicting Better Outcomes
- Earlier surgery: thinner membrane, less photoreceptor displacement, lower Govetto stage
- Preoperative VA of 20/40 or better
- Absence of EIFL on OCT (Govetto Stage 1)
- Intact photoreceptor IS/OS (inner segment/outer segment) junction on OCT
- Shorter symptom duration before surgery
- Idiopathic rather than secondary ERM
Recurrence
ERM recurrence after complete peeling occurs in approximately 2–5% of cases without ILM peeling, and 1–2% with concurrent ILM peeling. Recurrent ERM is typically less aggressive than the original and often managed conservatively.
Fellow Eye Risk
10–20% of patients with unilateral ERM will develop ERM in the fellow eye over follow-up periods of 5 years or more. Annual dilated fundus examination with OCT of the fellow eye is appropriate after a diagnosis of unilateral ERM.
Non-Surgical Management and Monitoring
Watchful Waiting
For patients with mild, stable, asymptomatic ERM — particularly cellophane maculopathy (Govetto Stage 1) without distortion — observation is the appropriate initial approach. Many such membranes remain stable for years. Surgery carries real risks and a recovery period; it is elective and should be deferred when the condition is not affecting quality of life.
Serial OCT Monitoring
For patients under observation, OCT imaging every 6–12 months tracks membrane thickness, retinal thickening, and foveal contour. Any progression — worsening OCT morphology, new symptoms, or declining VA — prompts re-discussion of surgical timing.
Home Amsler Grid Monitoring
Patients should perform daily Amsler grid testing at home (with reading glasses or correct near correction, in good lighting, one eye covered at a time). New distortion, missing areas, or change in the appearance of the grid warrants prompt evaluation — not waiting for the next scheduled appointment.
Anti-VEGF Injections
Intravitreal anti-VEGF agents (bevacizumab, ranibizumab, aflibercept) are the mainstay of treatment for wet age-related macular degeneration and diabetic macular edema. They have no established role in idiopathic ERM, where neovascularization is not part of the pathophysiology. In secondary ERM driven by a vascular condition (diabetic retinopathy, retinal vein occlusion), anti-VEGF treatment of the underlying condition may secondarily reduce membrane stimulus.
No Proven Medical Therapy
As of 2026, no oral medication, eye drop, or dietary supplement has been demonstrated in controlled trials to prevent ERM formation, slow progression, or cause regression. Patients should be counseled clearly on this point to avoid spending money on unproven treatments.
Nutrition and Eye Health Support
No specific diet or supplement has been proven to prevent or treat ERM. However, several nutrients support overall retinal and macular health and are appropriate to discuss, particularly when patients have concurrent risk factors such as diabetes, hypertension, or age-related macular degeneration risk.
Omega-3 Fatty Acids
Docosahexaenoic acid (DHA) is a structural component of photoreceptor membranes. EPA and DHA have anti-inflammatory properties relevant to retinal health. Fish consumption 2–3 times per week (salmon, sardines, mackerel, herring) or supplementation with 1–2 g of combined EPA+DHA daily is a reasonable evidence-informed recommendation for retinal health, though no trial has specifically targeted ERM.
Lutein and Zeaxanthin
These carotenoids are selectively concentrated in the macula, where they function as a blue-light filter and antioxidant. Supplemental lutein 10 mg + zeaxanthin 2 mg daily (or equivalent dietary intake from kale, spinach, cooked eggs) is supported by the AREDS2 trial in patients with risk factors for age-related macular degeneration and is a sensible adjunct for general macular health in ERM patients.
AREDS2 Formula
The AREDS2 formula (vitamin C 500 mg, vitamin E 400 IU, zinc 80 mg, copper 2 mg, lutein 10 mg, zeaxanthin 2 mg) reduces progression risk in established intermediate AMD by ~25%. For ERM patients who also have AMD risk factors (drusen, family history), AREDS2 supplementation is evidence-based. For ERM-only patients without AMD risk, it is reasonable but unproven specifically for ERM.
Blood Sugar and Blood Pressure Control
Diabetic retinopathy and retinal vein occlusion are common causes of secondary ERM. Tight glycemic control (HbA1c target as appropriate for individual patient) and blood pressure management (target <130/80 mmHg in most patients) reduce the risk of the vascular complications that drive secondary ERM formation.
Smoking Cessation
Smoking is the single most modifiable risk factor for age-related macular degeneration and impairs retinal vascular health broadly. Cessation is strongly encouraged for all retinal patients.
Anti-Inflammatory Diet
A Mediterranean-style diet rich in vegetables, fruit, whole grains, legumes, fish, and olive oil — and low in processed foods, refined carbohydrates, and trans fats — supports vascular and retinal health through anti-inflammatory and antioxidant mechanisms. This is appropriate general guidance for patients managing ERM alongside other age-related ocular and systemic conditions.
Cautions and Considerations
- Surgery is elective: ERM surgery is not an emergency. The decision should be made jointly by the patient and surgeon after a thorough discussion of current visual impact, surgical risks, recovery timeline, and realistic expectations for improvement. Patients with mild or stable ERM are not harmed by continued observation.
- Cataract is nearly universal post-vitrectomy: Patients with a natural lens should be counseled pre-operatively that cataract surgery will very likely be needed within 1–2 years of vitrectomy, either as a combined procedure or staged separately.
- Retinal risks: Intraoperative retinal tear occurs in approximately 1–2% of vitrectomy cases; retinal detachment in <1%. Endophthalmitis (intraocular infection) is a rare but devastating complication (<0.05%). Surgeons use prophylactic povidone-iodine and antibiotic drops perioperatively.
- ICG phototoxicity: Indocyanine green used for ILM staining carries dose- and light-exposure-dependent retinal toxicity risk. Surgeons who still use ICG should minimize concentration and exposure time; brilliant blue G (BBG) is the current preferred alternative.
- Persistent metamorphopsia: Even after technically successful surgery, some degree of residual distortion persists in a minority of patients. Patients should be counseled that metamorphopsia resolution lags VA improvement and that two years of recovery are needed before assessing the final functional result.
- Treat the underlying condition first: For secondary ERM from active diabetic retinopathy, uveitis, or retinal vein occlusion, the driving condition should be optimally treated before ERM surgery to reduce recurrence risk.
- Post-operative activity restrictions: Avoid eye rubbing, strenuous lifting, and swimming for 2–4 weeks after surgery. Face-down positioning is not routinely required for ERM surgery.
- Amsler grid use requires correct technique: Testing must be done at reading distance with reading glasses (or near correction) in adequate lighting, one eye occluded at a time. Incorrect technique generates false negatives.
References and Research
Key Research Papers
- Mitchell P et al. Prevalence and associations of epiretinal membranes. The Blue Mountains Eye Study. Ophthalmology. 1997;104(6):1033–1040. PMID 9186446 https://doi.org/10.1016/S0161-6420(97)30190-0
- Govetto A et al. Prevalence and clinical insights of retinal folds as a predictive sign of epiretinal membranes. Retina. 2016;36(7):1403–1412 — Search PubMed https://doi.org/10.1097/IAE.0000000000000934
- Michels RG. Vitreous surgery for macular pucker. Am J Ophthalmol. 1981;92(5):628–639 — Search PubMed https://doi.org/10.1016/0002-9394(81)90383-5
- Falkner-Radler CI et al. Specificity of the Amsler grid and the preferential hyperacuity perimetry (PHP) in the diagnosis of various macular conditions. Ophthalmology. 2012;119(1):19–25 — Search PubMed https://doi.org/10.1016/j.ophtha.2011.07.016
- Dawson SR et al. Vision-related quality of life in patients with early epiretinal membrane. Retina. 2009;29(4):517–521 — Search PubMed https://doi.org/10.1097/IAE.0b013e31819d40e4
- Sandali O et al. Fourier-domain optical coherence tomography imaging in epiretinal membranes: a descriptive study of 107 cases. Eur J Ophthalmol. 2011;21(2):209–216 — Search PubMed https://doi.org/10.5301/EJO.2010.3582
- Haritoglou C et al. Indocyanine green-assisted peeling of the internal limiting membrane. Am J Ophthalmol. 2002;134(1):163–164 — Search PubMed https://doi.org/10.1016/S0002-9394(02)01451-7
- Oster SF et al. Brilliant blue G (BBG)-assisted vitreoretinal surgery. Curr Opin Ophthalmol. 2012;23(3):167–172 — Search PubMed https://doi.org/10.1097/ICU.0b013e328353e576
- Wickham L et al. Surgical outcomes in macular epiretinal membranes: role of membrane characteristics and surgical technique. Ophthalmology. 2011;118(7):1376–1382 — Search PubMed https://doi.org/10.1016/j.ophtha.2010.12.003
- Pournaras CJ et al. Regulation of retinal local oxygen tension and preretinal neovascularization in vitreoretinal diseases. Prog Retin Eye Res. 2008;27(3):284–307 — Search PubMed https://doi.org/10.1016/j.preteyeres.2008.01.002
- Spiteri Cornish K et al. Peeling of the internal limiting membrane with and without the use of indocyanine green: a comparative study by optical coherence tomography and microperimetry. Br J Ophthalmol. 2011;95(9):1195–1198 — Search PubMed https://doi.org/10.1136/bjo.2010.196790
- Koerner F, Garweg J. Vitrectomy for macular pucker and vitreomacular traction syndrome. Doc Ophthalmol. 1999;97(3-4):449–458 — Search PubMed https://doi.org/10.1023/A:1002136307735
PubMed Topic Searches
- Epiretinal membrane vitrectomy outcomes
- Macular pucker OCT grading
- ILM peeling ERM recurrence
- Brilliant blue G vitreoretinal surgery
- Posterior vitreous detachment ERM
- Metamorphopsia ERM surgery recovery
- Ectopic inner foveal layers ERM
- Lutein zeaxanthin macular health
Connections
- Ophthalmology
- Macular Degeneration
- Retinal Detachment
- Diabetic Retinopathy
- Retinal Vein Occlusion
- Retinitis Pigmentosa
- Glaucoma
- Uveitis
- Cataracts
- Vitamin A
- Vitamin C
- Vitamin E
- Zinc
- Diabetes
- Omega-3 Fatty Acids
Featured Videos















