Retinitis Pigmentosa
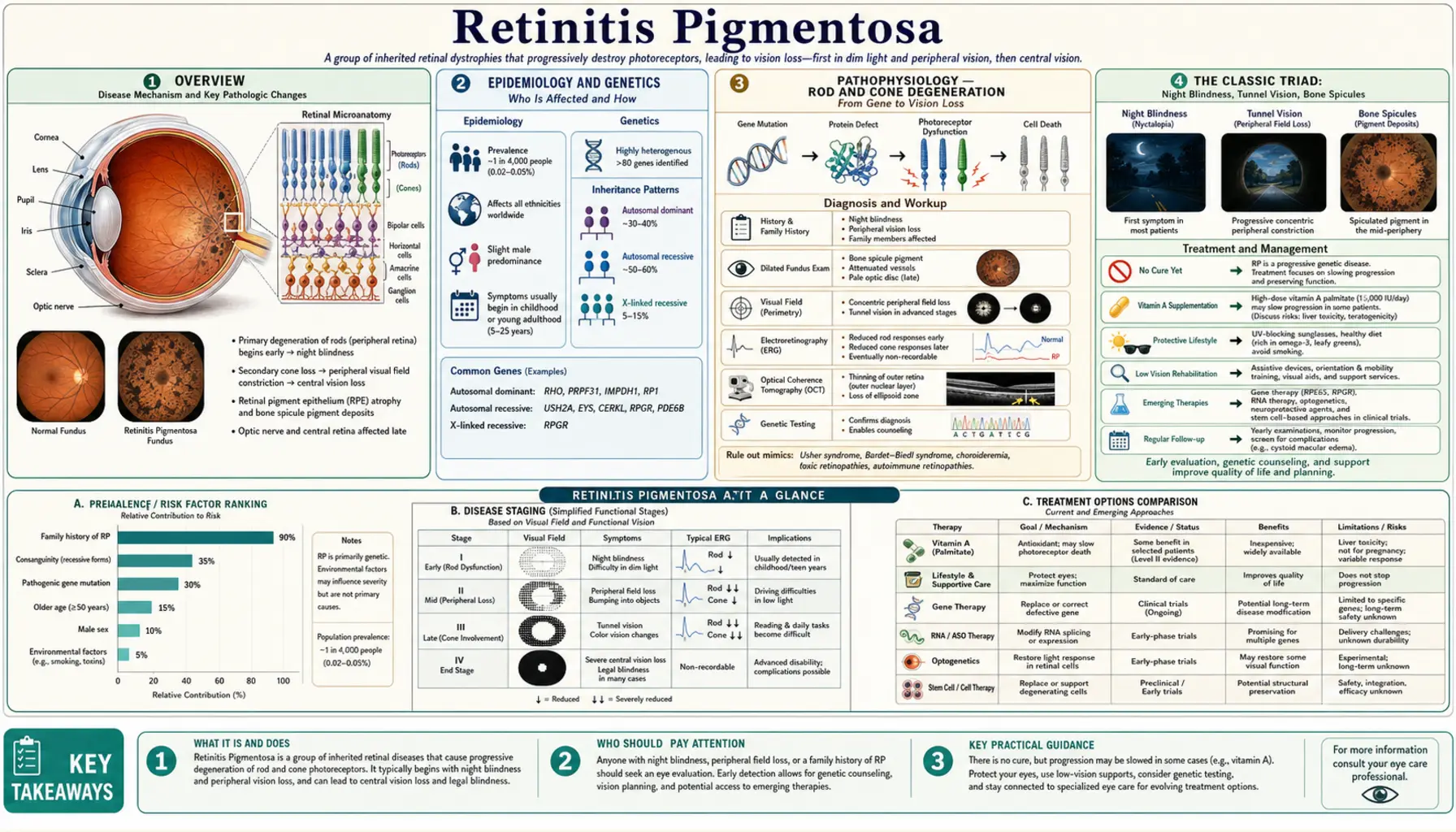
Table of Contents
- Overview
- Epidemiology and Genetics
- Pathophysiology — Rod and Cone Degeneration
- The Classic Triad: Night Blindness, Tunnel Vision, Bone Spicules
- Inheritance Patterns
- Syndromic Forms — Usher and Bardet-Biedl
- Diagnosis — ERG, Visual Field, Imaging
- Vitamin A Palmitate — A Controversial but Studied Treatment
- Lutein, Zeaxanthin, and DHA
- Gene Therapy — LUXTURNA for RPE65 Mutations
- Retinal Prosthesis — Argus II and Beyond
- Living with Retinitis Pigmentosa
- Key Research Papers
- Connections
- Featured Videos
Overview
Retinitis pigmentosa (RP) is an inherited degenerative disease of the retina — the light-sensitive tissue lining the back of the eye. It begins with the death of rod photoreceptors, the cells responsible for night and peripheral vision, and eventually affects cone photoreceptors, which handle central and color vision. The name comes from the characteristic dark pigment deposits that accumulate in the retina as rods die and the retinal pigment epithelium breaks down.
RP is not one disease but a collection of more than 100 distinct genetic conditions that all converge on the same end result: progressive photoreceptor degeneration. Because so many different genes are responsible, the disease can vary widely in severity, age of onset, and rate of progression from one person to the next — even within the same family carrying the same mutation.
RP is rare, affecting approximately 1 in 3,000 to 1 in 4,000 people worldwide. That translates to roughly 100,000 Americans and between 1 and 2 million people globally. Both sexes are affected approximately equally, with the exception of the X-linked form, which predominantly affects males. Symptoms typically begin in adolescence or young adulthood, though some genetic forms appear in childhood and others not until midlife.
There is currently no cure. However, treatments can slow progression in certain subtypes, and gene therapy has now provided meaningful functional vision restoration in a specific genetic subtype involving RPE65 mutations. Research is accelerating rapidly, with dozens of gene therapy, neuroprotection, optogenetics, and stem cell trials underway. Understanding your genetic subtype has become critically important — not only for prognosis and family counseling, but for determining eligibility for emerging therapies.
Epidemiology and Genetics
Retinitis pigmentosa is the most common inherited retinal dystrophy. Its prevalence of approximately 1 in 3,500 makes it uncommon but not vanishingly rare — there are more people with RP in the United States than there are with many better-known genetic diseases. The condition affects people of all ethnicities and geographic origins, without a strong predilection for any particular population.
Genetic complexity is the defining challenge of RP. More than 100 causative genes have been identified, encoding proteins that serve a remarkable variety of functions in the retina: phototransduction, the visual cycle, structural maintenance of photoreceptor outer segments, intraflagellar transport in the connecting cilium, pre-mRNA splicing, and RPE metabolism, among others. Despite this diversity of molecular defects, they all funnel into the same clinical picture of progressive photoreceptor loss.
The most commonly mutated genes in RP include:
- RHO (rhodopsin): the most common cause of autosomal dominant RP, accounting for approximately 25% of AD cases. Rhodopsin is the light-sensitive protein in rod outer segments; over 150 different RHO mutations have been described, and they cause disease through a variety of mechanisms including misfolding, constitutive activation, and protein aggregation.
- RPGR (retinitis pigmentosa GTPase regulator): the most common cause of X-linked RP, accounting for 70–80% of X-linked cases. RPGR is localized to the photoreceptor connecting cilium and is essential for protein trafficking between the inner and outer segments.
- USH2A: the most common gene mutated in Usher syndrome type II (combined RP and hearing loss), and also a frequent cause of non-syndromic autosomal recessive RP.
- EYS (eyes shut homolog): one of the most common AR-RP genes in some populations; encodes a large extracellular matrix protein in the interphotoreceptor matrix.
- PRPH2 (peripherin-2): encodes a structural protein of photoreceptor outer segment disc membranes; mutations cause both rod-dominant RP and macular dystrophies.
- CNGB1, PDE6A, PDE6B: components of the rod phototransduction cascade; mutations cause AR-RP with early-onset rod dysfunction.
Genetic testing using comprehensive retinal dystrophy gene panels (typically 250+ genes) can now identify a causative mutation in approximately 60% of RP patients. For the remaining 40%, mutations likely lie in undiscovered genes, in regulatory regions not covered by current panels, or in complex structural variants. Identifying a causative mutation matters practically: it allows accurate genetic counseling for family members, provides prognostic information about likely disease course, and — increasingly — determines eligibility for targeted gene therapy trials.
Pathophysiology — Rod and Cone Degeneration
To understand retinitis pigmentosa, it helps to understand the retina's cellular architecture. The human retina contains two types of photoreceptors: approximately 120 million rods and approximately 6 million cones. These are not distributed evenly. Rods are distributed across the entire peripheral retina, with a relative absence at the very center (the fovea). They are exquisitely sensitive to light — a single photon can activate a rod — and are responsible for vision in dim light, night vision, and motion detection. Cones are heavily concentrated in the central retina, especially the macula and the foveal pit, and are responsible for high-acuity central vision and color discrimination.
In RP, a mutant protein in the photoreceptor or its supporting retinal pigment epithelium (RPE) cell initiates a cascade of rod photoreceptor dysfunction and death. The mechanism varies by mutation — some cause misfolded proteins that activate the unfolded protein response and apoptosis; others impair the regeneration of light-sensitive chromophore; others disrupt the trafficking of proteins along the connecting cilium, causing outer segment structural failure. Despite these different initiating events, rods die through a final common pathway of programmed cell death (apoptosis and, more recently recognized, parthanatos — a caspase-independent form of cell death involving PARP1 hyperactivation).
The degeneration typically begins in the mid-peripheral retina, where rod density is high. As rods in this zone die, the surrounding RPE cells — which normally phagocytose shed outer segment discs and support photoreceptor metabolism — lose their normal function. The RPE cells release their stored melanin granules, which migrate into the sensory retina and form the characteristic "bone spicule" deposits visible on fundoscopy: irregular, branching dark deposits concentrated around retinal blood vessels in the mid-periphery.
Retinal blood vessels constrict as the photoreceptor layer thins — this vascular attenuation is a hallmark finding reflecting reduced metabolic demand from the degenerating retina. The optic nerve head develops a waxy pallor as optic nerve fibers from dying photoreceptors degenerate. OCT imaging reveals progressive thinning of the outer nuclear layer (which contains photoreceptor cell bodies) and eventual loss of the ellipsoid zone band (which marks the junction between inner and outer segments and reflects metabolic activity of photoreceptors).
Cone death follows rod death, but by a mechanism that is not fully understood. One leading hypothesis is the "trophic factor" theory: rods secrete survival signals (including rod-derived cone viability factor, RdCVF, discovered by Sahel and Bhun) that cones depend on for their survival. As rods disappear, cones lose this trophic support and gradually degenerate even if the cones themselves carry no mutation. A second hypothesis involves oxygen toxicity: rods consume large amounts of oxygen (the photoreceptor layer is one of the most metabolically active tissues in the body), and as rods die, the remaining oxygen supply may become relatively hyperoxic for the surviving cones, generating oxidative damage. Both mechanisms may contribute, and both suggest therapeutic strategies: delivering RdCVF to preserve cones, or antioxidant supplementation to reduce oxidative damage to cones.
The Classic Triad: Night Blindness, Tunnel Vision, Bone Spicules
Retinitis pigmentosa is clinically recognized by three cardinal features that reflect the underlying biology of rod-first, peripheral-first degeneration.
Nyctalopia (Night Blindness)
Night blindness is typically the earliest symptom and often precedes any structural changes visible on imaging. Patients describe difficulty seeing in dim or darkened environments — struggling in movie theaters, needing extra time to adjust when moving from a bright space to a dark one, difficulty driving after dusk. In its early stages, this may manifest specifically as impaired dark adaptation: the process by which the eye adjusts from photopic (cone-mediated, bright-light) to scotopic (rod-mediated, dim-light) vision normally takes about 20–30 minutes and relies on rhodopsin regeneration in the rods. In RP, this adaptation is slowed before frank night blindness develops.
Night blindness from RP must be distinguished from other causes: vitamin A deficiency (the most common cause of night blindness worldwide), congenital stationary night blindness (a non-progressive condition), and choroideremia (another X-linked inherited retinal dystrophy). The electroretinogram is diagnostic: in RP, scotopic rod responses are severely reduced or absent even in early disease.
Progressive Concentric Visual Field Constriction (Tunnel Vision)
As the mid-peripheral rods die and the degeneration expands, the visual field contracts concentrically. Patients report bumping into objects at the edge of their vision, difficulty in crowded environments like supermarkets or busy streets, problems reading maps or seeing the full frame of a computer screen, and challenges playing sports that require peripheral awareness. This loss is often not perceived until substantial field is already gone — because the visual cortex "fills in" missing peripheral information using surrounding context.
Visual field testing is the primary tool for monitoring progression. Goldmann kinetic perimetry maps the extent and shape of the remaining visual island. Automated static perimetry (Humphrey visual field) tests specific fixed points and is useful for tracking central field. In typical RP, the field constricts from an annular scotoma (ring-shaped blind area) in the mid-periphery, leaving an island of central vision and sometimes a small remaining island of far peripheral vision, until eventually only the central macular area remains functional — and in advanced disease, that too is lost.
Bone Spicule Pigmentation and Other Fundus Features
The fundoscopic appearance of established RP is characteristic: irregular dark pigment deposits scattered through the mid-peripheral retina, concentrated around and along retinal blood vessels in a branching, bony pattern (giving them the name "bone spicules" from their resemblance to bone cross-sections under the microscope). These deposits represent melanin pigment released from dying RPE cells migrating into the retina.
Accompanying signs include narrowed, attenuated retinal arterioles (reflecting reduced photoreceptor oxygen demand) and a waxy pale optic disc (reflecting optic nerve fiber loss from degenerated photoreceptors). In early RP, the fundus may look nearly normal — the ERG abnormality precedes structural changes. The pigment deposits typically become more prominent over time.
A common and treatable complication of RP is cystoid macular edema (CME): accumulation of fluid in the cystic spaces of the macula, detectable on OCT. CME occurs in 20–40% of RP patients and can significantly reduce central visual acuity beyond what would be expected from photoreceptor loss alone. Importantly, CME in RP is treatable with oral carbonic anhydrase inhibitors (acetazolamide, methazolamide), topical dorzolamide, or intravitreal anti-VEGF agents — treatment can meaningfully improve central vision in affected patients.
Posterior subcapsular cataracts develop earlier and more frequently in RP patients than in the general population, and cataract surgery can substantially improve vision in patients whose visual acuity is disproportionately impaired by the cataract.
Inheritance Patterns
One of the complexities of retinitis pigmentosa is that it does not follow a single inheritance pattern. The same clinical syndrome — progressive rod-cone degeneration with the classic triad — can be inherited as autosomal dominant, autosomal recessive, X-linked, or, rarely, mitochondrial. The pattern of inheritance influences disease severity, age of onset, and prognosis.
Autosomal Dominant RP (AD-RP)
Autosomal dominant RP accounts for approximately 30–40% of familial RP cases. One mutant copy of a gene is sufficient to cause disease. Affected individuals typically have an affected parent, and each child of an affected individual has a 50% chance of inheriting the mutation. AD-RP is generally milder than the recessive or X-linked forms, with later onset (often in the third or fourth decade) and slower progression. The most common genetic cause is mutation in the rhodopsin gene (RHO); other common genes include PRPH2, PRPF31, PRPF8, and IMPDH1.
Autosomal Recessive RP (AR-RP)
Autosomal recessive RP is the most common form, accounting for approximately 50–60% of familial RP cases (and many simplex cases where no family history is apparent). Two mutant copies are required — one inherited from each parent who is a carrier but unaffected. The more severe presentation is typical: earlier onset (often in the teens), more rapid progression. Common genes include USH2A, EYS, CNGB3 (for cone-rod dystrophy variants), RPGRIP1L, and CNGA1. Because carriers are asymptomatic, families often have no warning of risk until an affected child is diagnosed.
X-Linked RP (XL-RP)
X-linked RP, caused predominantly by mutations in RPGR and RP2, accounts for approximately 5–15% of RP cases but represents the most severe form. Because males have only one X chromosome, a single mutant copy of an X-linked gene causes full disease in males. Affected males typically have onset in childhood, severe night blindness and visual field loss by the second decade, and may lose central vision by the fifth decade. Females with one mutant copy (carriers) are usually only mildly affected or asymptomatic, though they may show patches of abnormal pigmentation on fundoscopy and can have measurable visual field loss.
Simplex RP and Digenic RP
Approximately 25% of RP patients have no affected family members (simplex RP). This may represent a new de novo mutation, an AR mutation with non-penetrant carriers in the family, or XL-RP where the carrier mother is asymptomatic. Genetic testing is especially important in simplex cases. In rare instances, RP is digenic: heterozygous mutations in two different genes together cause disease (the original example being RDS/PRPH2 + ROM1), neither mutation alone being sufficient.
Syndromic Forms — Usher and Bardet-Biedl
While most RP is non-syndromic (limited to the retina), approximately 20–30% of RP occurs as part of a broader genetic syndrome involving other organ systems. Recognizing syndromic RP changes the diagnostic workup, the specialist team required, and the treatment approach.
Usher Syndrome
Usher syndrome is the most common cause of combined visual and hearing impairment, affecting approximately 1 in 25,000 people. It combines sensorineural hearing loss with retinitis pigmentosa, and in some types, vestibular dysfunction (impaired balance). There are three clinical types:
- Usher type I: profound congenital deafness, severe vestibular dysfunction (delayed walking as infants, balance problems lifelong), and RP onset typically in the first decade. Caused by mutations in MYO7A, CDH23, PCDH15, USH1C, USH1G, and CIB2. The most severe form.
- Usher type II: moderate to severe congenital hearing loss (not profound), no vestibular dysfunction, and RP onset typically in the second or third decade. The most common type. Caused primarily by USH2A mutations, also ADGRV1 and WHRN.
- Usher type III: progressive hearing loss (not congenital), variable vestibular dysfunction, and RP. Rare. Caused by CLRN1 mutations; most common in Finnish and Ashkenazi Jewish populations.
Children with Usher type I are typically identified early through newborn hearing screening. The RP diagnosis may not be made until years later. Cochlear implants can restore hearing in Usher type I and III patients; gene therapy for the retinal component is being investigated for USH2A.
Bardet-Biedl Syndrome (BBS)
Bardet-Biedl syndrome is a ciliopathy — a disease of primary cilia — caused by mutations in over 20 BBS genes encoding proteins of the BBSome complex involved in ciliary transport. BBS is characterized by a pentad of findings: RP (onset typically in childhood, severe cone involvement), obesity (central, onset in childhood), polydactyly (extra fingers or toes, usually post-axial), renal anomalies (ranging from cysts to renal failure), and cognitive impairment (variable). Additional features include hypogonadism, diabetes, and congenital heart defects. Prevalence is approximately 1 in 100,000 in most populations, but higher in Bedouin Arabs (1 in 13,500) and Newfoundlanders (1 in 17,500) due to founder effects.
Other Syndromic Forms
Kearns-Sayre syndrome: caused by a large mitochondrial DNA deletion; features RP with progressive external ophthalmoplegia (weakness of the eye muscles), ptosis, and cardiac conduction defects (requiring pacemaker). Onset typically before age 20.
Refsum disease: caused by mutations in PHYH (phytanoyl-CoA dioxygenase) or PEX7; results in accumulation of phytanic acid, a branched-chain fatty acid derived from phytol in dietary chlorophyll. Clinical features: RP, peripheral neuropathy, cerebellar ataxia, sensorineural hearing loss, and anosmia. Critically, Refsum disease is treatable: a diet restricted in phytanic acid sources (beef, lamb, dairy fat, fatty fish) can stabilize or partially reverse neurological features and slow retinal deterioration. Plasma phytanic acid levels should be measured in any RP patient with peripheral neuropathy.
Diagnosis — ERG, Visual Field, Imaging
The diagnosis of retinitis pigmentosa is based on a combination of clinical history, fundoscopy, electrophysiology, and imaging. Early disease may look entirely normal on fundoscopy — the ERG abnormality precedes structural changes — making electrophysiology essential for early diagnosis.
Fundoscopy and Slit-Lamp Exam
The classic fundoscopic triad of bone spicule pigmentation, arteriolar attenuation, and waxy disc pallor is diagnostic of established RP. However, in early disease, the fundus may appear normal or show only subtle mid-peripheral pigment changes. Slit-lamp exam may reveal a posterior subcapsular cataract. The vitreous often shows fine cells in RP (inflammatory cells or pigment granules).
Electroretinogram (ERG)
The full-field electroretinogram is the gold standard functional test for RP. It measures the aggregate electrical response of the entire retina to flashes of light, recorded via electrodes placed on the cornea or conjunctiva. The standard protocol (ISCEV standard) includes:
- Scotopic (dark-adapted) rod response: a dim blue flash after 20–30 minutes of dark adaptation; reflects rod function. This is the most sensitive test for RP — rod responses are severely reduced (less than 50% of normal amplitude) or absent in nearly all RP patients even in early disease.
- Scotopic combined rod-cone response: a bright flash after dark adaptation; reflects combined rod and cone function.
- Photopic (light-adapted) cone response: flicker (30 Hz) and single-flash responses after light adaptation; reflects cone function. Cone responses are also reduced in RP, especially later in disease.
The ERG can distinguish RP (rod-cone dystrophy) from cone-rod dystrophy (cones affected first) and from macular dystrophies (pattern ERG affected, full-field ERG relatively normal). Serial ERG measurements track disease progression and are used in clinical trials as an objective endpoint.
Visual Field Testing
Goldmann kinetic perimetry maps the boundary of the visual field using targets of various sizes and brightnesses moved from non-seeing to seeing areas. It is the preferred method for tracking the characteristic concentric constriction of RP. Automated static perimetry (Humphrey visual field analyzer) tests a grid of fixed points and is complementary — useful for monitoring central field involvement and for functional endpoints in trials.
Optical Coherence Tomography (OCT)
OCT provides cross-sectional imaging of retinal layers with micrometer resolution. In RP, OCT shows:
- Progressive thinning and eventual loss of the outer nuclear layer (photoreceptor cell bodies)
- Disruption and loss of the ellipsoid zone (EZ) band — a hyperreflective line at the inner segment/outer segment junction that marks metabolically active photoreceptors; the extent of surviving EZ is a measure of remaining photoreceptor density and predicts visual acuity
- Cystoid macular edema (CME) when present — fluid-filled spaces in the inner nuclear and outer plexiform layers of the macula
- External limiting membrane (ELM) disruption as disease progresses
Wide-field OCT and OCT angiography (OCT-A) extend structural assessment to the peripheral retina. The ellipsoid zone width measured on OCT is now used as a structural endpoint in clinical trials for gene therapies.
Fundus Autofluorescence (FAF)
FAF imaging detects the natural fluorescence of lipofuscin — a metabolic byproduct of outer segment phagocytosis — in RPE cells. In RP, a ring of abnormal high autofluorescence typically surrounds the area of degeneration, corresponding to stressed but surviving RPE at the border of the advancing lesion. The area within the ring (fully degenerated RPE) shows reduced autofluorescence. The rate of shrinkage of the surviving autofluorescent area (the "AF ring") is used in clinical trials to track structural progression.
Genetic Testing
A comprehensive retinal dystrophy gene panel (250+ genes) is now standard of care for RP patients. It identifies a causative mutation in approximately 60% of cases. Genetic testing results are essential for:
- Genetic counseling of patients and family members (identifying carriers, informing reproductive decisions)
- Prognosis — some genotype-phenotype correlations are established (RPGR XL-RP is severe; PRPH2-related disease is milder)
- Eligibility for current gene therapy (only RPE65-mutation patients qualify for LUXTURNA)
- Enrollment in gene therapy clinical trials targeting specific mutations (e.g., RPGR, USH2A, CNGB3 trials currently enrolling)
Vitamin A Palmitate — A Controversial but Studied Treatment
Vitamin A palmitate remains the most widely discussed supplement for RP, and it is the only nutritional intervention for which there is a randomized clinical trial demonstrating a statistically significant (if modest) slowing of disease progression.
The pivotal study, published by Berson EH et al. in the New England Journal of Medicine in 1993 (PMID 8479463), randomized 601 adults with typical RP to four treatment groups: vitamin A palmitate 15,000 IU/day, vitamin A 15,000 IU/day plus vitamin E 400 IU/day, trace vitamin A 75 IU/day (placebo), or trace vitamin A plus vitamin E 400 IU/day. Over an average of 4.3 years of follow-up, participants taking 15,000 IU/day vitamin A palmitate showed an average annual rate of decline in cone ERG amplitude of approximately 8.3% per year versus 10.0% per year in the group not receiving vitamin A — a statistically significant slowing. A surprising finding was that vitamin E at 400 IU/day appeared to slightly accelerate cone ERG decline, so vitamin E supplements at high doses are not recommended for RP patients.
Follow-up analyses by Berson and colleagues over subsequent years continued to support a modest protective effect. The estimated benefit translates to an extension of functional vision by roughly 1–2 years over a decade of supplementation.
Important caveats:
- Not for all RP types: Vitamin A palmitate is potentially harmful in ABCA4-related retinal dystrophy (Stargardt disease and some RP variants), where it may accelerate the accumulation of lipofuscin and toxic bisretinoids. Genetic testing is important before starting vitamin A.
- X-linked RP caution: limited data in X-linked RP; the original Berson trial was primarily in typical (non-X-linked) RP.
- Not for children: not recommended in pediatric RP (no trial data; safety profile at 15,000 IU is not established in children).
- Absolutely contraindicated in pregnancy: high-dose vitamin A is teratogenic. Women of childbearing age should use reliable contraception if taking 15,000 IU/day vitamin A palmitate.
- Liver toxicity monitoring: annual liver function tests are recommended. Chronic intake of 15,000 IU/day is at the threshold of potential hepatotoxicity.
- Use only the palmitate ester form: not beta-carotene, not retinol acetate — the trial specifically used retinyl palmitate.
The Foundation Fighting Blindness and most retinal specialists recommend discussing vitamin A palmitate with your retina specialist before starting. It is not FDA-approved specifically for RP (it's a supplement, not a drug), but it is widely used off-label for appropriate patients. The most reasonable current approach is: confirm diagnosis with genetic testing, rule out ABCA4-related disease, discuss with specialist, start only if appropriate, monitor annually.
Lutein, Zeaxanthin, and DHA
Building on the vitamin A palmitate work, researchers have investigated additional nutritional adjuncts that might further slow RP progression. The best-studied are lutein (a carotenoid) and DHA (docosahexaenoic acid, an omega-3 fatty acid).
Lutein and Zeaxanthin
Lutein and zeaxanthin are the two carotenoids that make up macular pigment — the yellow pigment concentrated in the fovea that filters high-energy blue light and neutralizes reactive oxygen species. They are obtained entirely from the diet (green leafy vegetables, egg yolks) — the body cannot synthesize them — and accumulate in the retina selectively. Higher macular pigment optical density (measured non-invasively by heterochromatic flicker photometry) is associated with lower risk of age-related macular degeneration and with better visual function in several retinal diseases.
In RP, the key study was by Berson EH et al. (2010), a double-masked randomized trial of 225 adults with RP already taking vitamin A palmitate, randomized to add lutein (12 mg/day from lutein esters) versus placebo. Over 4 years, the lutein group showed a significantly slower decline in mean sensitivity of the visual field (5-2 test, central 30 degrees) compared to vitamin A alone — particularly in non-X-linked RP patients. The benefit was primarily on the mid-peripheral field, precisely the region first affected in RP. The supplement was safe and well-tolerated.
The current evidence-supported recommendation for many RP patients on vitamin A palmitate is to add lutein 12 mg/day. Zeaxanthin is typically included in lutein supplement formulations. High-lutein foods (kale, spinach, eggs) are also advisable.
DHA and Omega-3 Fatty Acids
DHA is the dominant fatty acid of photoreceptor outer segment membranes, comprising over 50% of the fatty acid content of the outer segment phospholipids. It is essential for the fluidity of disc membranes required for rhodopsin conformational change during phototransduction, and for normal photoreceptor development. Animal models of RP show abnormal DHA incorporation in outer segments and some studies suggest DHA supplementation can slow degeneration in rodent RP models.
The main human trial, the DHAX (DHA Xanthophyll) Study (Hoffman DR et al., 2004), randomized children with X-linked RP to DHA supplementation versus placebo and found a non-significant trend toward slower visual field loss in the DHA group over 4 years. A larger phase 3 trial of DHA in adults with RP (Birch DG et al.) showed no statistically significant benefit in the full cohort, though subgroup analyses suggested possible benefit in specific genetic subtypes. DHA supplementation at doses of 1,200–2,000 mg/day is generally safe (occasional fishy taste or GI discomfort), and many RP specialists recommend it given photoreceptor biology, despite the lack of a definitive trial result.
Practical takeaway: the combination of vitamin A palmitate 15,000 IU/day + lutein 12 mg/day + DHA (from fish oil or algal oil) is the current evidence-guided supplement regimen for appropriate RP patients — always discuss with your retina specialist before starting.
Gene Therapy — LUXTURNA for RPE65 Mutations
The approval of voretigene neparvovec (LUXTURNA) by the FDA in December 2017 was a landmark in medicine: it was the first FDA-approved gene therapy targeting a genetic disease in the United States. For RP and the broader field of inherited retinal dystrophies, it proved that gene therapy is not only theoretically sound but clinically effective.
The Biology of RPE65-Mediated Disease
RPE65 encodes retinoid isomerase (RPE-specific 65 kDa protein), an enzyme in the visual cycle that converts all-trans retinyl esters to 11-cis retinol in the RPE. 11-cis retinol is then oxidized to 11-cis retinal, which is the chromophore that combines with opsin to form rhodopsin (in rods) or cone opsins. Without functional RPE65, the visual cycle is blocked: photoreceptors cannot regenerate their light-sensitive visual pigment after it is bleached by light. The result is severely impaired vision from birth or early childhood, with progressive photoreceptor degeneration. Mutations in RPE65 cause Leber congenital amaurosis type 2 (LCA2) and early-onset severe RP — overlapping diagnoses that are now considered the same genetic disease on a spectrum.
How LUXTURNA Works
LUXTURNA consists of a recombinant adeno-associated virus serotype 2 (AAV2) vector carrying a functional copy of the human RPE65 gene under control of a hybrid promoter. It is delivered by subretinal injection: a vitreoretinal surgeon performs a vitrectomy and then injects a small volume of the vector solution directly into the subretinal space (between the photoreceptors and the RPE), where the AAV2 efficiently transduces RPE cells. Each eye is treated in a separate procedure, typically 6–18 days apart. The vector DNA persists in the RPE cells as an episome (it does not integrate into chromosomes), and the RPE cells produce normal RPE65 protein, restoring the visual cycle.
Clinical Trial Results
The pivotal Phase 3 trial (Russell S et al., Lancet 2017, PMID 29110997) enrolled 31 participants (ages 4–44) with confirmed biallelic RPE65 mutations and sufficient surviving retinal cells. Primary endpoint: multi-luminance mobility test (MLMT) — navigating an obstacle course at seven different light levels; the score reflected the lowest light level at which the patient could navigate successfully. At one year, 65% of LUXTURNA-treated eyes improved by 1.8 light levels versus 0% in controls — a dramatic, statistically significant difference (p < 0.0001). Secondary endpoints including full-field light sensitivity threshold (FST) and visual field also showed highly significant improvement. Results were maintained at 3 years, with no significant safety concerns beyond those expected from the subretinal surgery itself.
The functional improvements were meaningful for patients: people who had been legally blind navigating dim environments could now navigate them successfully. Patients reported being able to see stars, navigate unlit hallways, and drive (in some cases) for the first time.
Limitations and Practical Considerations
LUXTURNA is approved for patients with confirmed biallelic RPE65 mutations and sufficient viable retinal cells (too advanced degeneration cannot be rescued). Approximately 1,000–2,000 Americans have RPE65-mutation retinal disease. The therapy is extraordinarily expensive — approximately $850,000 for bilateral treatment — though insurance coverage (including Medicare) and patient assistance programs from Spark Therapeutics exist. The treatment requires expertise in subretinal surgery, available at specialized centers. The long-term durability beyond 3 years is being studied in ongoing follow-up.
The Broader Gene Therapy Pipeline
LUXTURNA opened the door. Dozens of gene therapy programs for other RP genes are now in clinical trials: RPGR (X-linked RP, multiple programs including from MeiraGTx and Applied Genetic Technologies), CNGB3 and CNGA3 (achromatopsia), CNGA1 (AR-RP), USH2A (Usher syndrome/RP), RHO (autosomal dominant RP, requiring RNA silencing + replacement approaches), and PROM1, PDE6A/B, and others. Anti-sense oligonucleotide (ASO) therapies, CRISPR gene editing approaches, and optogenetics (using viral vectors to express light-sensitive channelrhodopsin proteins in surviving retinal ganglion cells) are also in trials. The pace of development means that patients diagnosed today — particularly those with identified causative mutations — have real reason for optimism about treatments that may be available within their lifetime.
Retinal Prosthesis — Argus II and Beyond
For patients with advanced RP who have lost most functional photoreceptors and have bare light perception or worse, retinal prostheses (sometimes called "bionic eyes") offer a way to bypass the dead photoreceptors and deliver electrical stimulation directly to the surviving inner retinal neurons (bipolar and ganglion cells).
Argus II
The Argus II (Second Sight Medical Products) was the first epiretinal prosthesis to receive FDA approval for RP (2013) and the first retinal prosthesis approved anywhere in the world (CE mark 2011). The system consists of:
- A miniature camera mounted in a pair of glasses that captures the visual scene in real time
- A video processing unit worn on the body that converts the camera image into stimulation patterns
- A wireless transmitter that sends the patterns to a receiver implanted in the eye
- A 60-electrode array sutured to the surface of the retina (epiretinal), which delivers electrical pulses to remaining retinal ganglion cells and their axons
The 60 electrodes produce 60 discrete phosphenes (perceived flashes of light) — not a high-resolution image, but a pixelated grid of light and dark that allows detection of motion, location of large objects, discrimination of light from dark, reading of large high-contrast text, and improved mobility. In the pivotal trial published by Humayun MS et al. (Ophthalmology 2012, PMID 22281057), subjects showed statistically significant improvement in spatial-motor tasks (finding and touching a white square, walking along a white line on the floor) with the device on versus off.
The Argus II requires that some viable retinal ganglion cells and inner retinal neurons remain — it cannot work in completely degenerated retinas. The surgery is technically demanding and the implant carries risks of retinal detachment, infection, and erosion. Second Sight Medical Products pivoted to developing a cortical visual prosthesis (the Orion device, which bypasses the eye entirely and stimulates the visual cortex) after challenges with Argus II commercialization.
Other Approaches
The subretinal photovoltaic approach (PRIMA, Pixium Vision) uses a different strategy: a photovoltaic chip implanted under the retina converts incoming near-infrared light (from video glasses) directly into electrical stimulation of the bipolar cell layer without a wired external receiver. Early trials showed patients could read large letters and recognize faces. Alpha-IMS (Retina Implant AG), another subretinal device, uses ambient light directly to drive stimulation.
Optogenetics represents a potentially transformative approach: AAV vectors deliver genes encoding light-sensitive proteins (channelrhodopsins or halorhodopsins) into surviving retinal ganglion cells or bipolar cells, converting them into light sensors that can respond to specially designed video glasses emitting patterned amber or amber-spectrum light. The first human trial (Sahel JA et al., Nature Medicine 2021) reported a patient with RP who, using optogenetic gene therapy combined with video glasses, regained partial functional vision including the ability to perceive, locate, count, and touch objects — the first reported partial recovery of visual function through optogenetics. Multiple optogenetics programs are now in trials.
Living with Retinitis Pigmentosa
A diagnosis of retinitis pigmentosa changes a person's life. The progressive, incurable nature of the disease — affecting vision progressively from early adulthood — raises profound practical and emotional challenges. Importantly, there are many ways to adapt, compensate, and maintain quality of life even as vision narrows.
Low Vision Aids and Assistive Technology
Modern assistive technology has transformed life with visual impairment. Smartphones with accessibility features (iOS VoiceOver, Android TalkBack), screen magnification, and apps designed for low vision can be life-changing: Be My Eyes connects users with sighted volunteers or AI assistance for visual tasks; Seeing AI (Microsoft) uses the camera to read text, describe scenes, and identify faces; Aira provides on-demand remote sighted assistance. Screen readers, magnification software for computers, and high-contrast settings extend productive use of computers and tablets.
Optical low vision aids include handheld magnifiers, stand magnifiers, bioptic telescopes for distance viewing, and video magnifiers (CCTV systems) that project greatly magnified images on a screen. Large-print books, audiobooks, and e-readers with adjustable font and contrast remain valuable.
Orientation and Mobility Training
Orientation and mobility (O&M) specialists teach safe, independent travel skills: cane technique (the long white cane extends the effective range of safe detection ahead), use of visual landmarks, sighted guide technique, and navigating public transportation. Guide dog programs provide companionship and safety for people with sufficient remaining vision to handle a dog or those with bare light perception. Most vision rehabilitation centers and state services for the visually impaired offer O&M training without charge.
Driving
Night driving restrictions are typically necessary early in RP — the combination of night blindness and constricted peripheral field makes nighttime driving dangerous. As the disease progresses, complete driving cessation is required by law in most jurisdictions once visual field or acuity falls below the legal standard. This is one of the most difficult functional losses for many RP patients. Driving cessation should be an open conversation between the patient, their retina specialist, and in some cases the state licensing authority.
Treating Treatable Complications
Two complications of RP are frequently undertreated yet potentially highly impactful:
- Cystoid macular edema (CME): present in 20–40% of RP patients; reduces central acuity beyond what photoreceptor loss alone would predict. Oral carbonic anhydrase inhibitors (acetazolamide 250–500 mg/day; methazolamide for patients who do not tolerate acetazolamide) reduce CME and can significantly improve visual acuity in responsive patients. Topical dorzolamide is an alternative for those who cannot tolerate systemic side effects. Response should be assessed by OCT 4–8 weeks after starting treatment.
- Posterior subcapsular cataract: RP patients develop PSC earlier than the general population. Cataract surgery in an RP patient with a significant cataract contributing to visual acuity loss can meaningfully improve functional vision — though it does not affect the underlying retinal degeneration. Surgery is slightly higher risk in RP due to longer surgery times and potential for cystoid macular edema postoperatively.
Mental Health and Peer Support
Depression, anxiety, and grief are common responses to progressive vision loss — and they are underdiagnosed and undertreated in RP. The knowledge that vision will continue to deteriorate, uncertainty about the timeline, loss of driving and independence, impact on career and family planning, and the isolation of living in a world not designed for visual impairment all contribute. Psychological support — whether individual therapy, group therapy, or peer support networks — is an important component of comprehensive RP care.
The Foundation Fighting Blindness (blindness.org) is the primary nonprofit organization funding RP and inherited retinal disease research in the United States. It also operates patient support networks, hosts annual VisionWalk fundraising events, and maintains a detailed website with current research updates and resources. RP International and numerous disease-specific support communities exist for Usher syndrome, Bardet-Biedl syndrome, and specific genetic subtypes.
Research and Clinical Trials
Participating in clinical research is one of the most meaningful actions an RP patient can take — both for the potential personal benefit of accessing emerging therapies early and for advancing knowledge that will help future patients. The website clinicaltrials.gov lists all registered clinical trials; searching "retinitis pigmentosa" yields dozens of currently enrolling studies including gene therapy, optogenetics, neuroprotection, stem cell, and oral small molecule trials. The Foundation Fighting Blindness Clinical Trial Finder (clinicaltrials.fightingblindness.org) filters these specifically for inherited retinal disease patients. Knowing your genetic mutation is increasingly a prerequisite for trial eligibility.
Key Research Papers
- Berson EH, Rosner B, Sandberg MA, et al. A randomized trial of vitamin A and vitamin E supplementation for retinitis pigmentosa. N Engl J Med. 1993;328(22):1551–1559. PMID 8479463 — Landmark RCT establishing that vitamin A palmitate 15,000 IU/day slows cone ERG decline in typical RP; also found that high-dose vitamin E may accelerate decline.
- Berson EH et al. Randomized trial of lutein in retinitis pigmentosa (2010 lutein + vitamin A study). PubMed search: Berson lutein vitamin A retinitis pigmentosa 2010 — Adding lutein 12 mg/day to vitamin A palmitate slowed mid-peripheral visual field decline compared to vitamin A alone in non-X-linked RP.
- Russell S, Bennett J, Wellman JA, et al. Efficacy and safety of voretigene neparvovec (AAV2-hRPE65v2) in patients with RPE65-mediated inherited retinal dystrophy: a randomised, controlled, open-label, phase 3 trial. Lancet. 2017;390(10097):849–860. — Search PubMed — Pivotal Phase 3 trial showing LUXTURNA dramatically improved functional vision in RPE65-mutation patients; led to first FDA approval of a gene therapy for a genetic disease.
- Hartong DT, Berson EL, Dryja TP. Retinitis pigmentosa. Lancet. 2006;368(9549):1795–1809. — Search PubMed — Comprehensive authoritative review of RP genetics, pathophysiology, clinical features, and treatments. Widely cited foundational reference.
- RPGR mutations and X-linked retinitis pigmentosa. PubMed search: RPGR X-linked retinitis pigmentosa mutation — RPGR is the most common cause of X-linked RP, the most severe form; mutations cluster in an ORF15 hypermutable region.
- Usher syndrome: combined retinitis pigmentosa and sensorineural hearing loss. PubMed search: Usher syndrome retinitis pigmentosa hearing loss review — Usher syndrome is the most common genetic cause of combined deaf-blindness; three clinical types based on severity of hearing loss and age of RP onset.
- Humayun MS, Dorn JD, da Cruz L, et al. Interim results from the international trial of Second Sight’s visual prosthesis. Ophthalmology. 2012;119(4):779–788. — Search PubMed — International trial of the Argus II epiretinal prosthesis in RP patients with bare light perception; demonstrated statistically significant improvement in spatial-motor tasks with device on versus off.
- Electroretinogram (ERG) in the diagnosis and monitoring of retinitis pigmentosa. PubMed search: electroretinogram retinitis pigmentosa diagnosis monitoring — Full-field ERG is the gold standard functional test for RP; scotopic rod responses are severely reduced even in early disease before fundoscopic changes appear.
- Bardet-Biedl syndrome: ciliopathy with RP, obesity, and polydactyly. PubMed search: Bardet-Biedl syndrome retinitis pigmentosa genetics — BBS is caused by mutations in BBSome cilia transport proteins; RP is combined with obesity, polydactyly, renal anomalies, and cognitive impairment.
- Carbonic anhydrase inhibitors for cystoid macular edema in retinitis pigmentosa. PubMed search: carbonic anhydrase inhibitor cystoid macular edema retinitis pigmentosa — Oral acetazolamide and topical dorzolamide can reduce CME and improve visual acuity in the 20–40% of RP patients who develop this treatable complication.
- RHO rhodopsin mutations and autosomal dominant retinitis pigmentosa. PubMed search: rhodopsin RHO mutation autosomal dominant retinitis pigmentosa — RHO is the most common cause of AD-RP (~25% of AD cases); over 150 mutations described causing disease through misfolding, constitutive activation, and protein aggregation.
- Refsum disease: phytanic acid accumulation, RP, and dietary treatment. PubMed search: Refsum disease phytanic acid retinitis pigmentosa treatment — Refsum disease is a treatable syndromic cause of RP; dietary restriction of phytanic acid (dairy fat, fatty fish, beef, lamb) can stabilize or reverse neurological manifestations.
Connections
- Ophthalmology
- Macular Degeneration — another progressive retinal disease involving photoreceptor and RPE degeneration; overlapping research into gene therapy and neuroprotection
- Glaucoma — optic nerve disease causing visual field loss; important differential diagnosis for tunnel vision; shares some neuroprotection research pathways
- Cataracts — posterior subcapsular cataracts develop earlier in RP patients; cataract surgery can meaningfully improve remaining functional vision
- Amblyopia — reduced visual acuity from developmental causes; part of the broader ophthalmology context for visual impairment evaluation
- Dry Eye Disease — common ophthalmology condition; shares retina specialist care setting with RP patients
- Vitamin A — vitamin A palmitate 15,000 IU/day is the most studied nutritional supplement for slowing RP progression in appropriate patients
- All Conditions — complete disease index