Uveitis
Uveitis is inflammation of the uvea, the middle layer of the eye that supplies blood to the retina. It is one of the leading causes of preventable blindness in working-age adults worldwide. Unlike many eye conditions that develop slowly over decades, uveitis can flare suddenly and damage vision within days if not treated. Understanding what it is, what triggers it, and how it is managed can make a real difference in protecting your sight.
Table of Contents
- Overview and Definition
- Types of Uveitis
- Causes and Risk Factors
- Symptoms
- Diagnosis
- Conventional Treatment
- Natural and Lifestyle Approaches
- Complications
- Prognosis
- Prevention
- Key Research Papers
- Connections
- Featured Videos
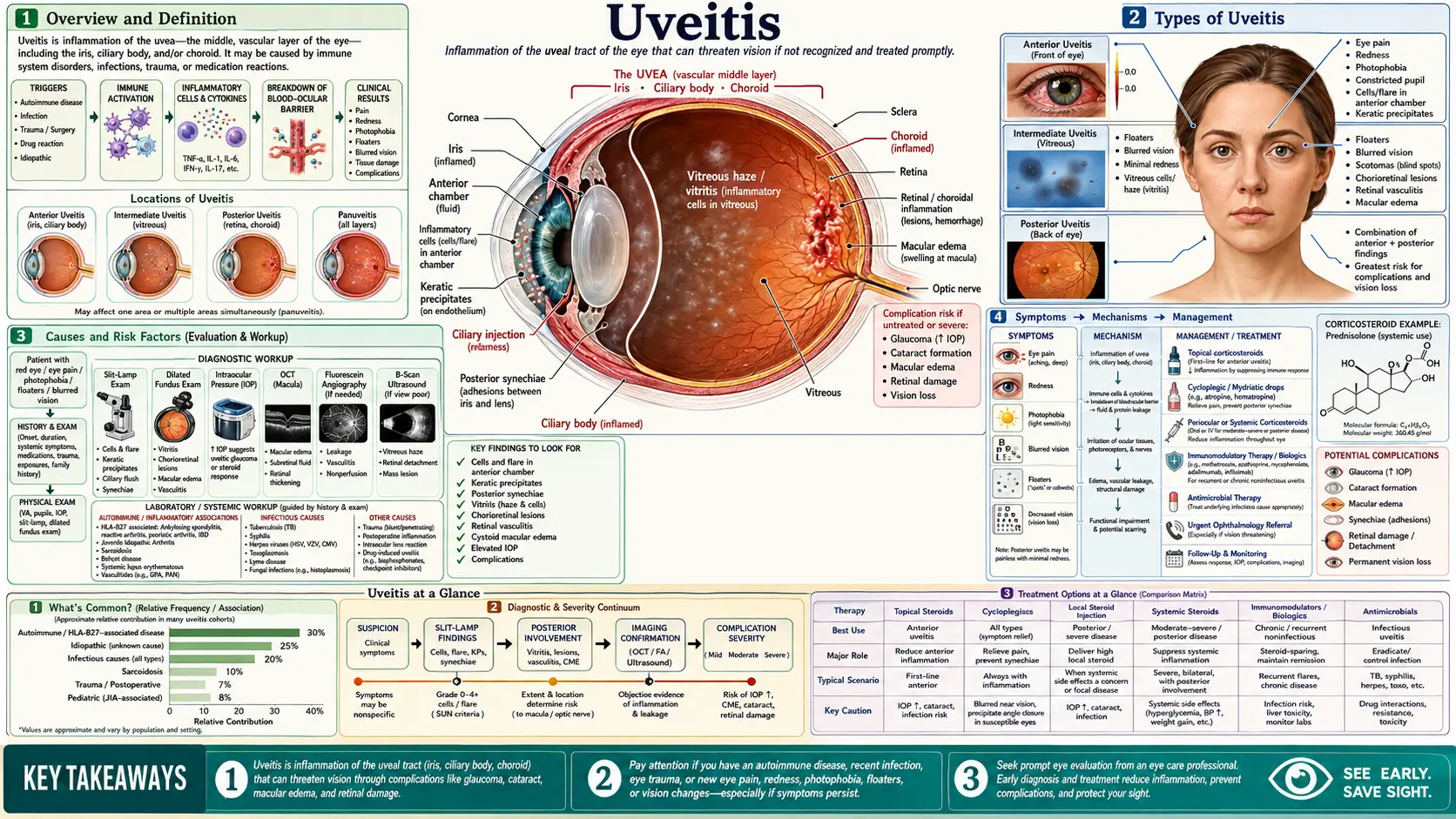
Overview and Definition
The eye is often described as a layered sphere. The outermost layer is the tough white sclera and the clear cornea. The innermost layer is the light-sensing retina. Sandwiched between them is the uvea, a richly vascular, pigmented middle coat made up of three connected structures:
- Iris — the colored ring that controls how much light enters through the pupil.
- Ciliary body — the ring of muscle and glandular tissue behind the iris that focuses the lens and produces the aqueous humor (the clear fluid filling the front of the eye).
- Choroid — the deeply pigmented, blood-vessel-rich layer lining most of the back of the eye and nourishing the retina.
When any part of this middle coat becomes inflamed — whether from an infection, an autoimmune response, or an injury — the condition is called uveitis. The inflammation can be confined to one part of the uvea or spread across the entire structure.
Uveitis affects an estimated 2 to 5 million people in the United States and accounts for roughly 10 to 15 percent of cases of legal blindness in the developed world. It strikes people of all ages but peaks in adults between 20 and 60 — the prime of working and family life. Because the uvea is so vascular, inflammation there can rapidly spill over to damage the lens, retina, optic nerve, and fluid-drainage system of the eye.
Types of Uveitis
Ophthalmologists classify uveitis by where in the eye the inflammation is located. This anatomical classification matters enormously because the underlying causes, treatments, and risks of complications differ by type.
Anterior Uveitis (Iritis / Iridocyclitis)
Anterior uveitis affects the iris and ciliary body — the front chamber of the eye. It is by far the most common form, accounting for roughly 50 to 90 percent of all uveitis cases in most clinical series. Most anterior uveitis is unilateral (one eye at a time), acute (comes on suddenly), and responds well to steroid eye drops. Chronic forms are rarer but more sight-threatening. The term iritis refers specifically to isolated iris inflammation; iridocyclitis means both iris and ciliary body are involved.
Intermediate Uveitis (Pars Planitis)
Intermediate uveitis centers on the vitreous — the gel-filled cavity behind the lens — and the peripheral retina and pars plana (the flat part of the ciliary body). Patients typically notice floaters and blurry vision. Pain and redness are often mild or absent. It is associated with conditions such as multiple sclerosis and sarcoidosis, but in many young patients no systemic cause is found (idiopathic pars planitis).
Posterior Uveitis (Chorioretinitis)
Posterior uveitis involves the choroid and/or retina at the back of the eye. Because there are no pain receptors in the retina, patients may have surprisingly little discomfort even while the inflammation silently damages their central vision. Infectious causes — particularly toxoplasmosis and cytomegalovirus — are common. Posterior uveitis carries the highest risk of permanent vision loss.
Panuveitis
Panuveitis is inflammation involving all three anatomical segments simultaneously. It is the most severe form and is associated with systemic diseases such as sarcoidosis, Behcet disease, and Vogt-Koyanagi-Harada (VKH) syndrome. Vision-threatening complications are the rule rather than the exception without aggressive treatment.
Causes and Risk Factors
Identifying the cause of uveitis is one of the most important — and sometimes most challenging — tasks in management. About 30 to 50 percent of cases are idiopathic (no identifiable cause is found even after a thorough work-up). The remainder split broadly between infectious and non-infectious (autoimmune or immune-mediated) origins.
Infectious Causes
- Toxoplasmosis — The most common cause of posterior uveitis worldwide. The parasite Toxoplasma gondii forms cysts in the retina; reactivation causes focal necrotizing chorioretinitis. Transmission is through undercooked meat or contact with infected cat feces.
- Herpes viruses — Herpes simplex (HSV) and varicella-zoster (VZV) most commonly cause anterior uveitis with elevated intraocular pressure; cytomegalovirus (CMV) causes a devastating retinitis in immunocompromised individuals (AIDS, organ transplants).
- Tuberculosis (TB) — An important cause globally, often presenting as granulomatous posterior or panuveitis. Ocular TB does not always mean active pulmonary disease; it may represent an immune-mediated reaction to remote infection.
- Syphilis — "The great masquerader" can mimic almost any pattern of uveitis. All uveitis patients should be screened for syphilis because it is treatable and curable.
- Lyme disease — Borrelia infection can cause intermediate or posterior uveitis, particularly in endemic regions of North America and Europe.
- Fungal infections — Candida and Aspergillus can seed the eye through the bloodstream, particularly in intravenous drug users or patients on total parenteral nutrition.
Non-Infectious / Autoimmune Causes
- HLA-B27-associated diseases — The human leukocyte antigen HLA-B27 is a genetic marker strongly linked to a cluster of inflammatory conditions. People who carry HLA-B27 and develop one of these conditions have a high risk of acute anterior uveitis:
- Ankylosing spondylitis (a.k.a. axial spondyloarthritis)
- Reactive arthritis (formerly Reiter syndrome)
- Psoriatic arthritis
- Inflammatory bowel disease (Crohn disease, ulcerative colitis)
- Sarcoidosis — A multisystem granulomatous disease that can affect any part of the uvea. Ocular sarcoidosis typically causes granulomatous anterior uveitis with large "mutton-fat" keratic precipitates, and may also cause choroidal granulomas, retinal vasculitis, and optic nerve involvement.
- Behcet disease — A systemic vasculitis characterized by recurrent oral ulcers, genital ulcers, and ocular inflammation. Ocular Behcet causes a severe, recurrent, obliterative retinal vasculitis that can destroy vision rapidly without aggressive immunosuppression.
- Vogt-Koyanagi-Harada (VKH) syndrome — An autoimmune attack on melanocytes (the pigment cells in the uvea, skin, inner ear, and meninges). It causes bilateral granulomatous panuveitis with serous retinal detachments, neurological symptoms, and skin depigmentation. More common in Asian, Hispanic, Middle Eastern, and Native American populations.
- Multiple sclerosis (MS) — Intermediate uveitis (pars planitis) is the most common ocular manifestation of MS. About 25 percent of MS patients develop uveitis over their lifetime.
- Juvenile idiopathic arthritis (JIA) — Children with certain subtypes of JIA (particularly antinuclear antibody-positive, oligoarticular JIA in young girls) develop a chronic, asymptomatic anterior uveitis that can silently scar the eye. Regular screening is essential.
- Lens-induced uveitis — Hypermature or traumatized cataracts can leak lens proteins into the anterior chamber, triggering an immune reaction.
Risk Factors
- Family history of uveitis or autoimmune disease
- HLA-B27 positivity (present in roughly 8 percent of white Northern Europeans)
- Immunocompromised state (HIV, organ transplant, immunosuppressive therapy)
- Exposure to endemic infectious agents (toxoplasmosis in tropical regions, TB in high-prevalence countries)
- Intravenous drug use (risk of fungal and bacterial endophthalmitis)
- Eye trauma or prior intraocular surgery
Symptoms
Symptoms vary considerably depending on which part of the eye is inflamed. This is one of the reasons uveitis can be missed — not all forms cause the classic painful red eye.
Anterior Uveitis — Typical Symptoms
- Red eye — Redness concentrated around the rim of the cornea (ciliary flush or perilimbal injection), rather than the diffuse redness of conjunctivitis.
- Eye pain — A deep, aching pain that is often worse in bright light. Unlike the gritty surface discomfort of dry eye or a scratch, this pain feels internal.
- Photophobia — Intense sensitivity to light. Even ordinary indoor lighting can be painful. This happens because light causes the inflamed iris to constrict, which is agony when the iris is swollen and stuck.
- Blurry vision — Inflammatory cells and protein leak into the aqueous humor, clouding the view like looking through fogged glass.
- Small or irregular pupil — Inflammation can cause the iris to stick to the lens (posterior synechiae), making the pupil irregular in shape or difficult to dilate.
Intermediate and Posterior Uveitis — Often Subtler
- Floaters — Clumps of inflammatory cells in the vitreous cast shadows on the retina. Patients describe them as spots, strings, or "snowballs" drifting across their vision.
- Blurry or hazy vision — Vitreous haze from inflammatory cells can reduce contrast sensitivity even when distance acuity tests reasonably well.
- Vision loss — Often gradual, sometimes sudden, particularly if macular edema or retinal detachment develop. This is the feature patients notice last, because the visual system compensates remarkably well until damage is significant.
- Little or no pain — Posterior uveitis can be entirely painless. Many patients with severe choroidal inflammation feel nothing until central vision deteriorates.
When to See a Doctor Immediately
Any sudden onset of eye pain, marked redness, or rapid vision change warrants same-day evaluation by an eye doctor. Uveitis that is left untreated for even a few days can cause scarring that is difficult or impossible to reverse. Do not wait to see if it "clears up on its own."
Diagnosis
Uveitis is diagnosed primarily through a slit-lamp examination — a biomicroscope that allows the ophthalmologist to examine the eye's structures in exquisite detail under high magnification. No blood test or scan can replace this hands-on exam.
Slit-Lamp Examination
- Anterior chamber cells and flare — Inflammatory white cells in the aqueous humor are graded on a standardized 0–4+ scale. Flare refers to the turbid appearance of the aqueous when it is protein-laden, similar to the way a sunbeam reveals dust in air.
- Keratic precipitates (KPs) — Clusters of inflammatory cells deposited on the inner surface of the cornea. Small, white "stellate" KPs suggest non-granulomatous inflammation; large, greasy "mutton-fat" KPs point toward granulomatous causes such as sarcoidosis or TB.
- Posterior synechiae — Adhesions between the iris and the front surface of the lens, seen as an irregular pupil or a pupil that does not dilate normally.
- Vitreous haze grading — A standardized 0–4+ scale rating how cloudy the vitreous gel has become from inflammatory infiltrate.
Intraocular Pressure (IOP)
IOP is measured at every visit. Uveitis can either raise IOP (by blocking fluid drainage with inflammatory debris or steroids) or lower it (severely inflamed ciliary bodies produce less fluid). Both extremes are important to track.
Dilated Fundus Examination
After dilating the pupils with drops, the ophthalmologist examines the vitreous, retina, choroid, and optic nerve with indirect ophthalmoscopy and contact lenses. This is the only way to detect posterior uveitis, retinal vasculitis, choroidal granulomas, or early signs of macular edema.
Imaging Studies
- Optical coherence tomography (OCT) — A non-invasive cross-sectional scan of the macula that detects cystoid macular edema (CME), epiretinal membranes, and sub-retinal fluid with extraordinary precision. CME is the most common cause of vision loss in uveitis, and OCT can detect it before it is visible to the naked eye.
- Fluorescein angiography (FA) — A dye injected intravenously highlights retinal blood vessels, revealing vasculitis, capillary non-perfusion, optic disc leakage, and areas of active choroiditis.
- Indocyanine green angiography (ICGA) — Penetrates deeper than fluorescein and visualizes the choroidal circulation, useful for detecting choroidal granulomas in sarcoidosis and VKH.
- B-scan ultrasound — Used when the view to the posterior pole is obscured (by dense vitreous haze, cataract, or corneal opacity) to assess for choroidal thickening, vitreous debris, and retinal detachment.
Systemic Work-Up
Finding the underlying cause guides treatment. The extent of the work-up depends on the clinical picture — a young adult with a first episode of acute anterior uveitis after a GI illness may only need HLA-B27 testing, while a patient with bilateral granulomatous posterior uveitis needs a much broader panel.
- HLA-B27 typing
- Complete blood count, comprehensive metabolic panel
- Syphilis serology (RPR or VDRL confirmed by FTA-ABS or TPPA)
- QuantiFERON-TB Gold or tuberculin skin test (PPD)
- Chest X-ray or CT (for sarcoidosis, TB)
- Serum ACE and lysozyme (sarcoidosis markers)
- Antinuclear antibody (ANA) — especially in children, to rule out JIA-associated uveitis
- Toxoplasma IgG/IgM serology (in posterior uveitis)
- HIV testing (in immunocompromised presentations or CMV retinitis)
- Lyme serology in endemic areas
Conventional Treatment
The goals of treatment are to suppress inflammation, prevent damage, preserve vision, and treat any underlying systemic disease. Therapy is tailored to the type, severity, and cause of uveitis.
Corticosteroids — The Foundation of Treatment
Corticosteroids remain the first-line anti-inflammatory agents for most non-infectious uveitis. They are used in several forms:
- Topical steroid eye drops (prednisolone acetate 1%, difluprednate) — The mainstay for anterior uveitis. A typical acute-episode regimen starts at every 1–2 hours while awake and tapers over weeks as inflammation resolves. Frequent dosing is critical — missing drops allows inflammation to flare.
- Periocular steroid injections — Triamcinolone acetonide injected into the sub-Tenon's space (just outside the eye wall) delivers a high local concentration without systemic absorption. Used for intermediate and posterior uveitis.
- Intravitreal steroid implants — The fluocinolone acetonide implant (Retisert, Yutiq) releases steroid continuously inside the eye for 2–3 years. It is highly effective for chronic non-infectious posterior uveitis but carries significant risks of steroid-induced glaucoma and cataract.
- Systemic oral prednisone — Used when inflammation is bilateral, posterior, or inadequately controlled by local therapy. Long-term systemic steroids carry well-known side effects (bone loss, weight gain, diabetes, hypertension, adrenal suppression) and are not a sustainable long-term strategy.
Mydriatics and Cycloplegics
Drops such as atropine, cyclopentolate, or tropicamide dilate the pupil and paralyze the ciliary muscle. This accomplishes two things: it relieves the spasm-driven pain of anterior uveitis, and it prevents the iris from sticking to the lens. These drops are typically used for the first few weeks of an acute anterior uveitis episode.
Steroid-Sparing Immunosuppressants
When uveitis is chronic, recurrent, or posterior, long-term systemic immunosuppression is often necessary to control the disease while minimizing steroid exposure. The main agents are:
- Methotrexate — A folate antagonist widely used for JIA-associated uveitis and other chronic non-infectious forms. Given weekly (oral or subcutaneous). Requires folic acid supplementation and monitoring of liver function and blood counts.
- Mycophenolate mofetil (CellCept) — Often favored over methotrexate for posterior uveitis. Generally well tolerated; main side effects are GI upset and increased infection risk.
- Azathioprine — An older agent with a long track record in Behcet disease and VKH syndrome. Requires TPMT enzyme testing before starting to avoid dangerous myelosuppression.
- Cyclosporine — Particularly effective for Behcet uveitis but limited by nephrotoxicity and hypertension with long-term use.
Biologic Therapies
Adalimumab (Humira), a TNF-alpha inhibitor, became the first biologic approved by the FDA specifically for non-infectious intermediate, posterior, and panuveitis in adults who have failed conventional immunosuppression. The pivotal VISUAL I and VISUAL II trials demonstrated that adalimumab significantly reduced the risk of uveitis flares and vision-threatening complications compared to placebo. Infliximab, another TNF inhibitor, is used off-label, particularly for Behcet disease where the evidence base is strong. Other biologics being evaluated include secukinumab (anti-IL-17) and tocilizumab (anti-IL-6).
Anti-Infective Therapy
Infectious uveitis requires targeted treatment of the causative organism:
- Toxoplasmosis — Classic regimen: pyrimethamine + sulfadiazine + leucovorin (folinic acid). Alternatives include clindamycin, trimethoprim-sulfamethoxazole, or azithromycin. Steroids are added cautiously after anti-parasitic cover is established.
- Herpetic uveitis — Oral valacyclovir or acyclovir for HSV and VZV; intravenous ganciclovir or oral valganciclovir for CMV. Intravitreal ganciclovir or foscarnet may be needed for CMV retinitis.
- Ocular syphilis — Intravenous penicillin G, following the same regimen as neurosyphilis.
- Ocular TB — Standard four-drug anti-TB therapy (isoniazid, rifampin, pyrazinamide, ethambutol) for six to nine months, with adjunctive systemic steroids.
Natural and Lifestyle Approaches
Natural approaches do not replace medical treatment for active uveitis — this is an inflammatory condition that can cause permanent blindness without proper management. However, evidence supports several complementary strategies that may reduce the frequency and severity of flares and support overall eye health.
Omega-3 Fatty Acids
Omega-3 polyunsaturated fatty acids — particularly EPA (eicosapentaenoic acid) and DHA (docosahexaenoic acid) — competitively inhibit the production of pro-inflammatory prostaglandins and cytokines. Studies in inflammatory eye diseases suggest that higher omega-3 intake is associated with reduced inflammation markers. Fatty fish (salmon, sardines, mackerel, herring), walnuts, and flaxseed are the richest food sources. A daily supplement of 2–3 grams of combined EPA+DHA is generally safe, though it may interact with anticoagulants.
Vitamin D
Vitamin D deficiency is remarkably common and has been associated with an increased risk of autoimmune conditions including the inflammatory arthropathies that cause HLA-B27-related uveitis. Vitamin D acts as an immune modulator, promoting regulatory T-cell activity that helps prevent excessive immune responses. Getting adequate sunlight exposure, eating vitamin D-rich foods (fatty fish, eggs), and supplementing to maintain a serum 25-OH vitamin D level above 40–60 ng/mL is a reasonable general strategy for people with recurrent immune-mediated uveitis.
Antioxidant-Rich Diet
Dark leafy greens (spinach, kale, collard greens) are rich in lutein and zeaxanthin — xanthophyll carotenoids concentrated in the macula that filter damaging blue light and act as local antioxidants. While research on lutein specifically in uveitis is limited, the broader anti-inflammatory dietary pattern (Mediterranean-style, high in vegetables, fruit, whole grains, olive oil, and fish) is associated with lower systemic inflammatory markers and better outcomes in immune-mediated diseases.
Avoiding Smoking
Tobacco smoking significantly worsens outcomes in inflammatory eye diseases. It promotes systemic oxidative stress and inflammation, impairs the response to immunosuppressive medications, and independently increases the risk of macular degeneration and cataract — two of uveitis's most dangerous complications. Quitting smoking is one of the highest-value lifestyle changes a uveitis patient can make.
Stress Management
Psychological stress reliably triggers flares of autoimmune and inflammatory conditions. Mechanisms include stress-hormone-driven shifts in immune regulation (cortisol initially suppresses inflammation, but chronic stress dysregulates the HPA axis and ultimately promotes it). Mind-body practices with a reasonable evidence base include mindfulness-based stress reduction (MBSR), yoga, regular aerobic exercise, and adequate sleep. None of these is a replacement for medication, but they may extend remission intervals.
Regular Ophthalmology Follow-Up
For patients with conditions known to cause uveitis — particularly JIA in children and HLA-B27-positive spondyloarthropathies in adults — scheduled screening visits allow subclinical inflammation to be caught and treated before it causes damage. The frequency depends on the specific condition and risk profile; your ophthalmologist will set the schedule.
Complications
Uveitis is dangerous not only because of the inflammation itself but because of the secondary structural damage it can cause over time. These complications are the primary reason uveitis is one of the leading causes of preventable vision loss.
Cystoid Macular Edema (CME)
CME is the accumulation of fluid in the central retina (macula), disrupting the precise photoreceptor architecture needed for sharp central vision. It is the most common vision-threatening complication of uveitis, occurring in up to 40 percent of patients with intermediate or posterior uveitis. Symptoms are blurring and distortion of central vision. OCT is the gold standard for detection. Treatment involves local and systemic steroids, intravitreal anti-VEGF agents, and controlling the underlying uveitis.
Glaucoma
Uveitic glaucoma affects approximately 20 percent of uveitis patients over their lifetime. Inflammation raises IOP through multiple mechanisms: inflammatory cells clog the trabecular meshwork that drains aqueous humor; posterior synechiae can block fluid flow from the posterior to anterior chamber (causing iris bombe, a dramatic forward bowing of the iris); and long-term topical and systemic steroid use independently elevates IOP in genetically susceptible individuals ("steroid responders"). Uveitic glaucoma can be very difficult to control and may ultimately require filtering surgery or drainage implants.
Cataracts
Both uveitis and its treatment cause cataracts. Chronic inflammation directly damages the lens epithelium; corticosteroids — both topical and systemic — promote formation of posterior subcapsular cataracts, which selectively blur vision and cause severe glare. Cataract surgery in a uveitic eye is more complex and has higher complication rates than routine cataract surgery; inflammation must be fully suppressed for at least three months before operating.
Posterior Synechiae and Seclusio Pupillae
Posterior synechiae are adhesions between the posterior iris surface and the anterior lens capsule. When they encircle the entire pupil (360-degree synechiae), they create a closed ring called seclusio pupillae, which completely blocks aqueous flow and causes acute angle-closure glaucoma with rapidly rising IOP. This is a medical emergency requiring urgent laser iridotomy.
Retinal Detachment
Chronic inflammation can cause membranes to form on the surface of the retina (epiretinal membranes) or within the vitreous. These membranes can contract and pull the retina away from the underlying pigment epithelium, causing tractional or rhegmatogenous retinal detachment. Prompt surgical repair is required to preserve vision.
Hypotony
Severe, chronic inflammation of the ciliary body can so thoroughly damage its secretory function that aqueous humor production falls critically low (IOP below 6 mmHg). Sustained hypotony leads to choroidal effusions, macular folds, and eventually a shrunken, non-functional eye (phthisis bulbi). This is one of the most feared end-stage complications of untreated uveitis.
Band Keratopathy
Calcium deposits in the superficial cornea, forming a chalky white horizontal band across the visual axis, can develop in longstanding uveitis particularly in children with JIA. It can be removed with EDTA chelation treatment but tends to recur if inflammation is not controlled.
Prognosis
The outlook for uveitis varies enormously depending on the type, cause, and how promptly treatment begins.
Anterior Uveitis
Acute anterior uveitis (iritis) typically responds quickly to topical steroids and cycloplegics. Most episodes resolve fully within 6–8 weeks with appropriate treatment. Vision generally returns to baseline, and structural complications are uncommon in a first episode. However, recurrences are frequent — up to 50 percent of patients experience at least one additional episode within five years, particularly those who are HLA-B27-positive. Chronic anterior uveitis (as in JIA) is harder to manage and carries higher complication rates.
Intermediate Uveitis
The course tends to be protracted, with chronic smoldering inflammation punctuated by flares. CME is the main cause of vision loss. With proper immunosuppression, many patients maintain useful vision, but the disease often requires treatment for years or even decades.
Posterior and Panuveitis
These carry the highest risk of permanent vision impairment. Infectious posterior uveitis (toxoplasmosis) leaves chorioretinal scars at the site of active lesions; while subsequent episodes can be treated, each leaves additional scar tissue. VKH syndrome, Behcet disease, and severe sarcoidosis can devastate vision despite aggressive therapy, though early and sustained immunosuppression significantly improves outcomes. Overall, studies suggest that approximately 35 percent of uveitis patients have some degree of visual impairment over their disease course, with 5 to 10 percent reaching legal blindness.
Prognostic Factors
- Earlier diagnosis and treatment consistently correlate with better outcomes.
- Bilateral disease, posterior involvement, and panuveitis predict more complications.
- Underlying systemic conditions (particularly Behcet disease) are associated with greater vision loss.
- Achieving and maintaining remission, rather than tolerating low-grade persistent inflammation, appears critical for long-term visual preservation.
Prevention
Because many causes of uveitis are infectious or autoimmune — conditions not fully preventable — the emphasis in prevention is on reducing flare frequency, catching recurrences early, and preventing complications.
- Know your risk profile. If you carry HLA-B27 or have a condition such as ankylosing spondylitis, psoriatic arthritis, or IBD, learn the warning signs of uveitis (sudden eye pain, redness, photophobia) so you seek care at the very first symptom rather than waiting days.
- Adhere to your medication regimen. For people on immunosuppressants or biologics for systemic inflammatory disease, consistent adherence reduces both joint and eye flares. Missing doses is a common trigger for rebound inflammation.
- Regular screening for high-risk children. Children with JIA — particularly young girls with ANA-positive oligoarticular disease — should have slit-lamp examinations every 3–4 months even if their eyes feel perfectly normal. Their uveitis is often silent until complications develop.
- Food safety measures for toxoplasmosis prevention. Cook meat thoroughly (internal temperature ≥71°C/160°F), wash hands and surfaces after handling raw meat, avoid consuming untreated water, and have someone else change the cat litter box (or wear gloves and wash hands afterwards) to reduce the risk of acquiring T. gondii.
- Protect against herpes reactivation triggers. Emotional stress, UV sun exposure to the face, fever illnesses, and immunosuppression are known triggers of herpes virus reactivation. People with recurrent herpetic anterior uveitis may be offered long-term suppressive antiviral therapy (e.g., oral acyclovir or valacyclovir) to reduce reactivation frequency.
- Manage underlying systemic disease optimally. Well-controlled ankylosing spondylitis, IBD, or sarcoidosis is associated with fewer and less severe uveitis episodes. Working with your rheumatologist, gastroenterologist, or pulmonologist is integral to eye health.
- Avoid tobacco. Smoking is an independent risk factor for more severe and recurrent uveitis and worsens related complications.
Key Research Papers
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
- Search PubMed
Connections
- Ophthalmology
- Glaucoma
- Cataracts
- Retinal Detachment
- Macular Degeneration
- Ankylosing Spondylitis
- Crohn's Disease
- Dry Eye Disease
- Uveitis & Eye Involvement in AS
- Behçet's Disease — systemic vasculitis in which hypopyon and posterior uveitis with retinal vasculitis are defining ocular features.