Retinal Detachment
Retinal detachment is a true ocular emergency. When the light-sensitive retina peels away from the back wall of the eye, it is cut off from its blood supply within minutes to hours. Without urgent surgical repair, permanent blindness in the affected eye is likely. Knowing the warning signs — sudden floaters, flashing lights, or a dark curtain spreading across your vision — and acting on them the same day you notice them can mean the difference between full sight and irreversible loss.
Table of Contents
- Overview and Definition
- Types of Retinal Detachment
- Causes and Risk Factors
- Warning Signs and Symptoms
- Diagnosis
- Surgical Treatment
- Recovery and Natural Support
- Complications
- Prognosis
- Prevention
- Key Research Papers
- Connections
- Featured Videos
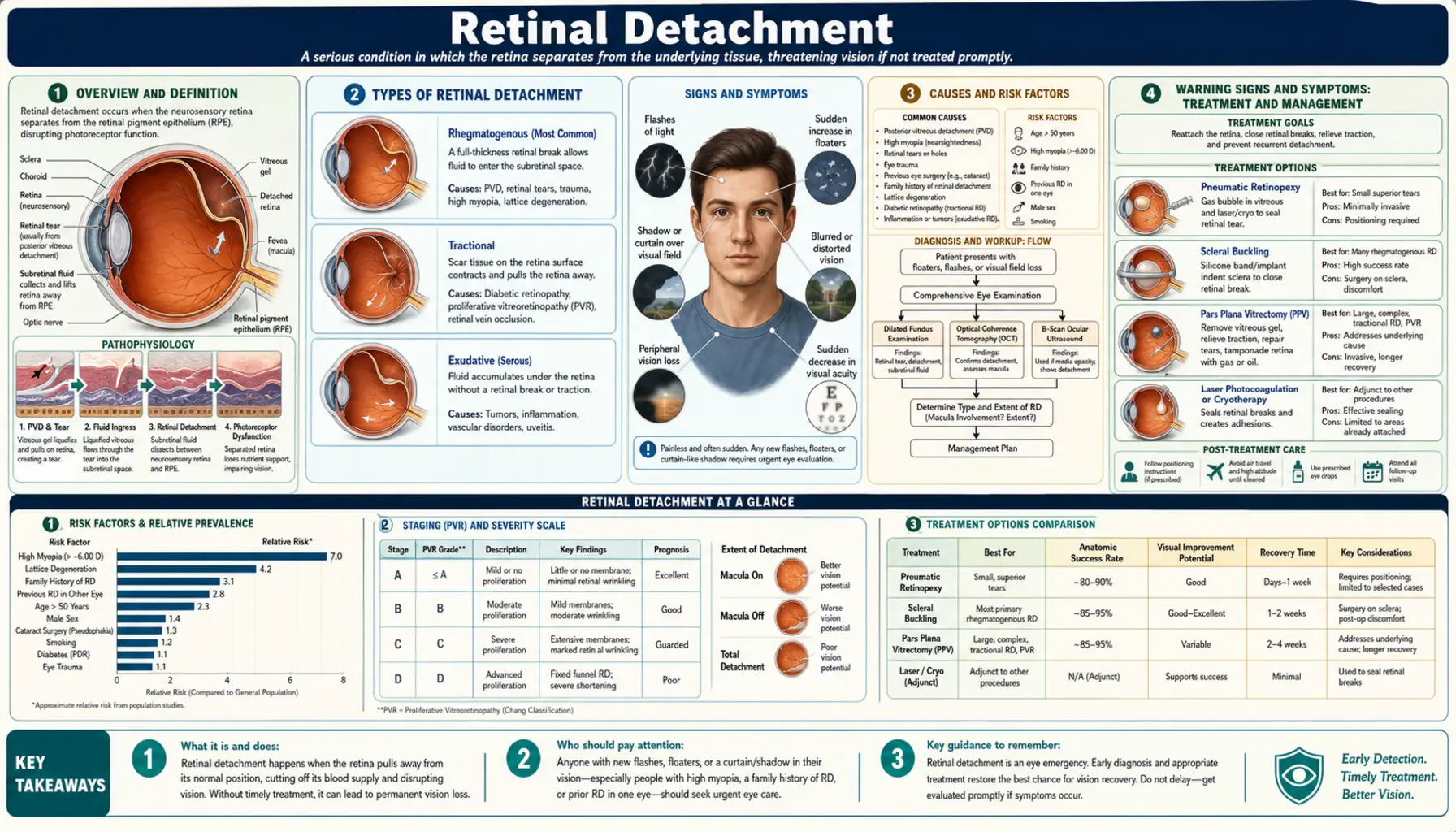
Overview and Definition
The retina is a paper-thin layer of nerve tissue lining the inside back surface of the eye. Think of it as the film in an old camera — it captures light, converts it into electrical signals, and sends those signals along the optic nerve to the brain where the image is interpreted. The retina is nourished by the retinal pigment epithelium (RPE), a layer of cells that sits directly beneath it and delivers oxygen and nutrients from the choroid (a network of blood vessels deeper in the eye wall).
Retinal detachment occurs when the retina separates from the RPE. Once detached, retinal cells begin to die from oxygen starvation within hours. The longer the detachment goes untreated — especially if it extends to the macula, the central region responsible for sharp reading and color vision — the worse the visual outcome. Studies show that repairing a detachment before it reaches the macula (a "macular-on" detachment) routinely restores near-normal vision, while a "macular-off" detachment that has been present for even a few days often leaves lasting central vision loss even after anatomically successful surgery.
Retinal detachment affects approximately 1 in 10,000 people per year in developed countries, with higher rates in people over age 50 and those with significant near-sightedness. It is slightly more common in men than women and more common in White populations than in people of African descent, likely due to differences in vitreous anatomy and myopia prevalence.
Types of Retinal Detachment
There are three distinct types of retinal detachment, each with a different underlying mechanism, patient population, and treatment approach.
Rhegmatogenous Retinal Detachment (RRD)
This is by far the most common type, accounting for roughly 90% of all cases. "Rhegmatogenous" comes from the Greek word for break or rent. In RRD, a tear or hole develops in the retina — typically at the peripheral retina where the tissue is thinnest — and liquid vitreous fluid seeps through the break and accumulates underneath, lifting the retina away from the RPE. The most frequent trigger is posterior vitreous detachment (PVD), a normal age-related event in which the gel-like vitreous that fills the eye shrinks and pulls away from the retina. In most people PVD is harmless, but in some it creates enough traction to tear the retina as it separates.
Tractional Retinal Detachment (TRD)
In tractional detachment, abnormal fibrovascular membranes — sheets of scar tissue — grow on the retinal surface and physically pull it away from the RPE. There is no tear or hole; the retina is mechanically dragged upward. The most common cause is proliferative diabetic retinopathy, in which new fragile blood vessels sprout abnormally, leak, and eventually scar. TRD is also seen in sickle-cell retinopathy, retinopathy of prematurity, and penetrating trauma. TRD tends to progress more slowly than RRD but is technically more challenging to repair.
Exudative (Serous) Retinal Detachment
In this type, fluid leaks from abnormal blood vessels or inflamed tissue beneath the retina and accumulates without any tear or tractional force — the retina is pushed off the RPE from below by the fluid. Causes include age-related macular degeneration (particularly the "wet" form), uveitis (intraocular inflammation), malignant hypertension, tumors (choroidal melanoma, metastases), and Vogt-Koyanagi-Harada (VKH) disease. Treatment targets the underlying cause rather than the detachment itself, which often resolves once the primary condition is controlled.
Causes and Risk Factors
Understanding who is at higher risk helps people know when to take symptoms seriously and seek care urgently.
High Myopia (Near-Sightedness)
People with significant myopia — particularly a prescription of -6.0 diopters or more — have elongated eyeballs. This stretching thins the peripheral retina and creates zones of weakness called lattice degeneration, where the retina is abnormally thin, sometimes laced with crisscrossing white lines. Lattice degeneration is found in about 8–10% of the general population but is far more common in highly myopic eyes, and it dramatically increases the risk of retinal tears and RRD. High myopes are 6–8 times more likely to experience retinal detachment than people with normal vision.
Age and Posterior Vitreous Detachment
PVD occurs in most people over age 60. In the vast majority it causes harmless floaters and resolves without complication. However, if the vitreous is abnormally adherent to the retina at certain points, it can tear the retina as it pulls free. The incidence of RRD rises steeply after age 50 and peaks between ages 60 and 70.
Prior Cataract Surgery
Cataract surgery is a known risk factor for retinal detachment, particularly in myopic eyes and when surgery is complicated by posterior capsule rupture. The risk is highest in the first year after surgery and in younger patients. The mechanism is thought to involve changes in vitreous dynamics after the natural lens is removed.
Previous Retinal Detachment in the Fellow Eye
Having had a detachment in one eye raises the lifetime risk of detachment in the other eye to approximately 10–15%, compared to 0.01% in the general population. Both eyes share similar anatomical characteristics, so if one is vulnerable, the other often is too.
Family History
First-degree relatives of people who have had retinal detachment have a modestly elevated risk, particularly in families where high myopia runs strongly.
Trauma
A direct blow to the eye — from a sports injury, airbag deployment, or assault — can create retinal tears immediately or months later as contusion-related changes evolve. Even indirect trauma (whiplash, blast injury) can occasionally trigger detachment.
Lattice Degeneration
This peripheral retinal thinning can be found and monitored on dilated eye exams. While prophylactic laser treatment of lattice is sometimes considered in high-risk patients, the evidence for treating asymptomatic lattice is not straightforward — routine surveillance is typically the approach.
Diabetes and Sickle-Cell Disease
Conditions that cause abnormal retinal blood vessel growth (neovascularization) predispose to tractional retinal detachment. Uncontrolled diabetes is the leading cause of TRD in adults in developed countries.
Warning Signs and Symptoms
These symptoms require same-day emergency evaluation. Do not wait until the next morning, the next available appointment, or the weekend. Call your ophthalmologist immediately or go to an emergency room.
Sudden Floaters
A sudden shower, swarm, or curtain of new black dots, cobwebs, or strands in your vision is a red-flag symptom. Everyone has some floaters — old ones that have been there for years are usually benign. But a dramatic, sudden increase in floaters means the vitreous may have just torn the retina, releasing a burst of pigment or blood cells into the vitreous cavity. This is not normal aging. It is an emergency until proven otherwise.
Flashes of Light (Photopsia)
Flashes that look like lightning, camera flashes, or sparks — especially in the peripheral (side) vision — indicate that the vitreous is tugging on the retina. The retina has no pain receptors, but mechanical stimulation causes it to generate false light signals. Flashes alone can indicate a retinal tear before detachment has occurred, making them an important warning to act on.
A Shadow, Curtain, or Veil in Vision
Once the retina begins to detach, the area of detached retina stops functioning and creates a corresponding blind spot. This typically starts as a dark arc or shadow in the peripheral vision and, if left untreated, progresses toward the center like a curtain being drawn across the visual field. If the detachment is in the superior (upper) retina, the curtain comes from the bottom of the visual field, and vice versa — the visual field defect is inverted relative to the anatomical location of the detachment.
Sudden Blurry or Distorted Central Vision
Once the macula — the central, high-resolution part of the retina — is involved in the detachment, sharp central vision drops suddenly. Reading, recognizing faces, and fine detail work become difficult. Macular involvement is the single most important factor determining final visual outcome, which is why speed of treatment is so critical.
What NOT to Wait For
Retinal detachment is painless. There is no redness, no discharge, and no discomfort. People sometimes dismiss the symptoms because they feel fine physically. Do not let the absence of pain convince you this can wait. The retina silently dies while you hesitate.
Diagnosis
Diagnosing retinal detachment requires a comprehensive eye examination by an ophthalmologist. The following tools are used.
Dilated Fundus Examination
Eye drops are used to widen (dilate) the pupil, giving the ophthalmologist a clear view of the peripheral retina. Using an indirect ophthalmoscope — a headlamp-style device that projects a bright light — the doctor can see nearly the entire retina including the far periphery where tears most often occur. The exam involves pressing gently on the eye with a small probe (scleral depression) to roll the peripheral retina into view. It is uncomfortable but essential.
Slit-Lamp Biomicroscopy
A slit lamp with a contact or non-contact lens provides a magnified, stereoscopic view of the posterior segment and is used to examine the macula in detail and assess the extent of detachment.
B-Scan Ultrasound
When the view to the retina is blocked — by dense cataract, vitreous hemorrhage, or corneal opacity — B-scan ultrasound uses sound waves to image the posterior segment. A detached retina appears as a bright, mobile membrane on ultrasound. This is a critical tool for trauma cases where hyphema or hemorrhage obscures the view.
Optical Coherence Tomography (OCT)
OCT provides high-resolution cross-sectional images of retinal layers and is particularly valuable for detecting subtle macular involvement, shallow detachments, and early retinoschisis (splitting of retinal layers that can mimic detachment). It is also used post-operatively to monitor macular recovery.
Differentiating from Retinoschisis
Retinoschisis — a splitting of the retina's inner layers — is common in older adults and can look like a detachment on casual exam. OCT and careful indirect ophthalmoscopy with scleral depression differentiate the two: retinoschisis typically has an absolute visual field defect (not a relative one), no vitreoretinal traction, and a smooth elevated surface without folds.
Surgical Treatment
All rhegmatogenous retinal detachments require surgery. There is no medication or eye drop that can reattach a detached retina. The three main surgical options each work by sealing the retinal break(s) and facilitating reattachment of the retina to the RPE.
Pneumatic Retinopexy
This is the least invasive option and can often be performed in the office under local anesthesia. The surgeon injects an expanding gas bubble (usually sulfur hexafluoride, SF6, or perfluoropropane, C3F8) into the vitreous cavity. The patient must then position their head so that the bubble floats up against the retinal tear, tamponading (blocking) it from the inside. Within days, the RPE pumps out the subretinal fluid, reattaching the retina. The tear is then permanently sealed with laser photocoagulation or cryotherapy (freezing). Pneumatic retinopexy works best for single tears in the superior retina and has lower primary success rates (70–80%) than the other procedures, but it avoids incisions and has faster visual recovery when it succeeds. A critical restriction: patients cannot fly or travel to high altitude while the gas bubble is present, as altitude change causes the bubble to expand dangerously, spiking intraocular pressure. The gas bubble gradually absorbs over 2–8 weeks depending on the gas used.
Scleral Buckle
In scleral buckling, a silicone band or sponge is sutured to the outside of the eye wall (sclera), indenting the eye wall inward. This reduces the pull (traction) of the vitreous on the retinal tear and brings the outer eye wall closer to the detached retina, helping it reattach. The subretinal fluid may be drained through a small incision, or it can be left to absorb spontaneously. The tear is sealed with cryotherapy or laser. Scleral buckling has excellent long-term outcomes and avoids entering the vitreous cavity, preserving the vitreous gel — an advantage for young patients. It is the procedure of choice in many young myopic patients and in cases where vitrectomy access is limited. A scleral buckle stays in place permanently and can sometimes cause increased myopia or double vision (diplopia) from altered eye muscle mechanics.
Pars Plana Vitrectomy (PPV)
Vitrectomy is now the most commonly performed procedure for retinal detachment repair in many countries. The surgeon makes small (0.6–0.9 mm) incisions into the eye and uses fine instruments to remove the vitreous gel entirely. With the vitreous removed, the traction on the retinal breaks is eliminated. The surgeon then identifies and treats all breaks with endolaser (laser applied from inside the eye) and fills the eye with a gas bubble or silicone oil to provide long-term tamponade while the breaks heal. Gas gradually absorbs over weeks; silicone oil is a longer-lasting tamponade used for complex cases but requires a second surgery to remove it (typically 3–6 months later). Vitrectomy allows treatment of multiple and posterior breaks, complex detachments, and TRD, and is increasingly favored for its versatility. The main downsides are accelerated cataract formation (nearly universal within 2 years in phakic patients) and all the restrictions that come with gas tamponade.
Timing: Macular-On vs. Macular-Off
If the macula remains attached (macular-on detachment), surgery is urgent — ideally within 24 hours — to prevent the detachment from progressing to involve the macula. If the macula has already detached (macular-off), surgery is still urgent but the calculus changes slightly: some surgeons delay 24–48 hours in macular-off cases to allow the patient to fast, optimize surgical conditions, and schedule during daylight hours, since the visual prognosis is already determined by the duration of macular detachment. Operating in haste in the middle of the night for macular-off does not improve the final visual outcome but increases surgical risk. For macular-on detachment, every hour counts.
Recovery and Natural Support
Recovery from retinal detachment surgery takes weeks to months, depending on the procedure and whether the macula was involved.
Face-Down Positioning
After vitrectomy with gas tamponade, most patients are required to maintain face-down (prone) positioning for anywhere from a few days to two weeks. This keeps the gas bubble floating against the upper retina where breaks are typically located. It is physically and mentally grueling. Specially designed face-down pillows and massage tables exist to make this more tolerable. Compliance with positioning directly affects surgical success rates.
Activity Restrictions
During recovery, patients must avoid strenuous physical activity, heavy lifting (more than 5–10 lbs), and anything that significantly raises blood pressure. Bending at the waist, coughing forcefully, and straining are also discouraged. These restrictions typically last 4–6 weeks.
No Flying With a Gas Bubble
This restriction cannot be overstated. Flying at altitude — or ascending to high altitude by land — while a gas bubble is in the eye can cause the bubble to expand and create dangerously high intraocular pressure, potentially resulting in optic nerve damage and permanent vision loss. Patients must carry a written physician note stating they cannot fly and know the estimated absorption date of their gas. Silicone oil, by contrast, does not expand with altitude and does not restrict air travel.
Driving
Patients cannot drive until the gas bubble has absorbed sufficiently and vision in the surgical eye meets legal driving standards. This typically means 6–12 weeks of not driving (longer if the other eye has poor vision).
Nutrition and Natural Support
While no supplement replaces surgery, certain nutrients support retinal healing and long-term retinal health:
- Omega-3 fatty acids (DHA/EPA): DHA is the most abundant fatty acid in the retina and is essential for photoreceptor membrane structure and function. Dietary omega-3s from fatty fish (salmon, sardines, mackerel) or fish oil supplements support retinal recovery and reduce retinal inflammation.
- Vitamin A: The retina requires vitamin A (retinol) to produce rhodopsin, the light-sensitive pigment in rod cells. Severe vitamin A deficiency causes night blindness and can worsen retinal cell survival. Adequate dietary intake through liver, eggs, and orange/yellow vegetables is important during recovery.
- Lutein and zeaxanthin: These carotenoids concentrate in the macula and filter damaging blue light. Foods rich in lutein include kale, spinach, and egg yolks. They are not curative for retinal detachment but support macular integrity long-term.
- Vitamin C and E: Antioxidants reduce oxidative stress in retinal tissue. The AREDS2 formulation (studied extensively for macular degeneration) includes high-dose C, E, zinc, lutein, and zeaxanthin and supports general retinal health.
- Blood pressure control: Uncontrolled hypertension can cause hypertensive retinopathy and contributes to exudative detachment. Maintaining systolic blood pressure below 130 mmHg reduces vascular stress on retinal vessels.
- Blood sugar control: In diabetic patients, tight glycemic control is the single most powerful intervention to prevent tractional retinal detachment. Every percentage point reduction in HbA1c substantially reduces the risk of proliferative diabetic retinopathy.
Complications
Even with successful anatomical reattachment, several complications can affect the visual outcome or require additional intervention.
Proliferative Vitreoretinopathy (PVR)
PVR is the most feared complication of retinal detachment repair and the leading cause of surgical failure. It occurs when retinal pigment epithelial cells and glial cells migrate into the vitreous cavity and onto the retinal surface, forming contractile membranes that create new traction and re-detach the retina. PVR complicates approximately 5–10% of primary RRD repairs and is more common after large tears, inferior detachments, and vitreous hemorrhage. Treating established PVR requires complex vitrectomy to peel membranes off the retina, which is technically demanding with guarded visual prognosis.
Re-Detachment
Even after successful initial repair, 5–10% of retinal detachments re-detach, usually within the first few months. Causes include missed breaks at the original surgery, new breaks opening up, or early PVR. A sudden return of symptoms after initial recovery requires immediate re-evaluation.
Epiretinal Membrane (ERM)
After vitrectomy, a thin scar membrane can grow on the macular surface, causing distortion and blurring of central vision. ERMs develop in 5–20% of eyes after retinal detachment repair. Mild ERMs are monitored; significant ones causing visual impairment can be peeled surgically (membranectomy) in a subsequent procedure.
Cataract Progression
Vitrectomy universally accelerates cataract formation in patients who still have their natural lens (phakic patients). Within 2 years, nearly all phakic patients develop visually significant cataracts requiring cataract surgery. Many surgeons combine cataract removal with vitrectomy in older patients.
Macular Hole
In some cases, particularly after macular-off detachment, a macular hole can form in the central retina, causing a permanent central blind spot. Macular holes can sometimes be repaired with additional surgery.
Persistent Visual Loss
Even with anatomically perfect reattachment, some degree of permanent visual impairment is common, particularly in macular-off detachments of long duration. The photoreceptors in the macula can suffer irreversible damage from even a few days of ischemia. Visual recovery continues for 12–18 months after surgery, but many patients are left with reduced contrast sensitivity, metamorphopsia (distortion), and difficulty in low light even when Snellen acuity (the standard chart) measures 20/20.
Prognosis
Modern retinal detachment surgery has a high overall success rate, but outcomes vary considerably based on the type of detachment, timing of repair, and whether the macula is involved.
Anatomical Success
Approximately 90% of rhegmatogenous retinal detachments are successfully reattached with a single surgical procedure. The remaining 10% require a second or third surgery, and the vast majority of these are also ultimately reattached. Tractional detachments (TRD) have somewhat lower primary success rates due to the complexity of membrane peeling, but outcomes have improved dramatically with modern wide-angle visualization systems and smaller-gauge instrumentation.
Visual Outcomes by Macular Status
- Macular-on RRD: When surgery is performed before the macula detaches, 80–90% of patients recover vision of 20/40 or better (good enough to drive). Many recover 20/20.
- Macular-off RRD, short duration (<1 week): Approximately 60–70% achieve 20/40 or better. Visual recovery is slower — often improving for up to a year post-surgery.
- Macular-off RRD, long duration (>2 weeks): Only about 30–40% achieve 20/40. Many patients are left with permanently reduced central acuity, even with perfect anatomical repair.
The takeaway is unambiguous: time is vision. Seeking care the same day symptoms appear is the single most powerful thing a patient can do to protect their visual outcome.
Long-Term Fellow Eye Risk
After one retinal detachment, the fellow eye has a 10–15% lifetime risk of detachment. Annual dilated eye exams are recommended indefinitely. Any new floaters, flashes, or visual field changes in the fellow eye should trigger immediate evaluation.
Prevention
Retinal detachment cannot always be prevented, but several strategies meaningfully reduce risk.
Regular Dilated Eye Exams
Annual or biannual dilated fundus exams allow ophthalmologists to identify high-risk findings — lattice degeneration, suspicious tears, symptomatic retinal breaks — before they become detachments. Highly myopic individuals and those with a personal or family history of RRD should not skip these exams.
Prompt Evaluation of New Symptoms
The single most important prevention strategy is treating any new floaters or flashes of light as an emergency. Many retinal tears can be sealed with laser photocoagulation or cryotherapy in the office before fluid gets under the retina and causes detachment. This is a relatively minor procedure done under local anesthesia with very high success rates when performed early.
Protective Eyewear
Wearing appropriate eye protection during contact sports (racquetball, squash, boxing, basketball, hockey), power tool work, and activities with projectile risk significantly reduces the risk of traumatic retinal tears and detachment.
Diabetes Management
For people with diabetes, maintaining tight blood sugar control (target HbA1c below 7%) and having annual dilated retinal screenings dramatically reduces the risk of proliferative diabetic retinopathy and tractional retinal detachment. Early treatment with pan-retinal photocoagulation (PRP) laser or anti-VEGF injections at the proliferative stage prevents TRD before surgery becomes necessary.
Blood Pressure Management
Controlling hypertension reduces the risk of exudative retinal detachment from hypertensive retinopathy and protects overall retinal vasculature health.
Post-Cataract Surgery Vigilance
Patients who have undergone cataract surgery — especially those who are highly myopic — should be educated about retinal detachment symptoms before leaving the surgery center and should understand the importance of immediate evaluation if they develop sudden new floaters, flashes, or visual field changes in the months to years after their procedure.
Key Research Papers
The following peer-reviewed studies have shaped the modern understanding and treatment of retinal detachment.
- Search PubMed — Epidemiology of rhegmatogenous retinal detachment: a 20-year prospective population study.
- Search PubMed — Randomized clinical trial of scleral buckling versus primary vitrectomy for rhegmatogenous retinal detachment.
- Search PubMed — Retinal detachment: a review of current management strategies.
- Search PubMed — Pneumatic retinopexy for superior rhegmatogenous retinal detachment repair.
- Search PubMed — Management of retinal detachment: a review of clinical approaches and outcomes.
- Search PubMed — Effect of duration of macular detachment on the visual outcome following surgical repair of primary macula-off rhegmatogenous retinal detachment.
- Search PubMed — Proliferative vitreoretinopathy: development, classification, prevention, and management.
- Search PubMed — Visual outcome and reattachment rates in primary vitrectomy for complex rhegmatogenous retinal detachment.
- Search PubMed — Outcomes of retinal detachment repair: a large prospective cohort study.
- Search PubMed — Tractional retinal detachment secondary to proliferative diabetic retinopathy: surgical outcomes and predictive factors.
PubMed Searches for Further Reading
- Rhegmatogenous retinal detachment surgery — PubMed
- Pars plana vitrectomy retinal detachment — PubMed
- Proliferative vitreoretinopathy treatment — PubMed
- Macular-off retinal detachment visual prognosis — PubMed
- Tractional retinal detachment diabetic retinopathy — PubMed
Connections
- Ophthalmology
- Glaucoma
- Cataracts
- Diabetic Retinopathy
- Macular Degeneration
- Uveitis
- Diabetes
- Dry Eye Disease