Rocky Mountain Spotted Fever
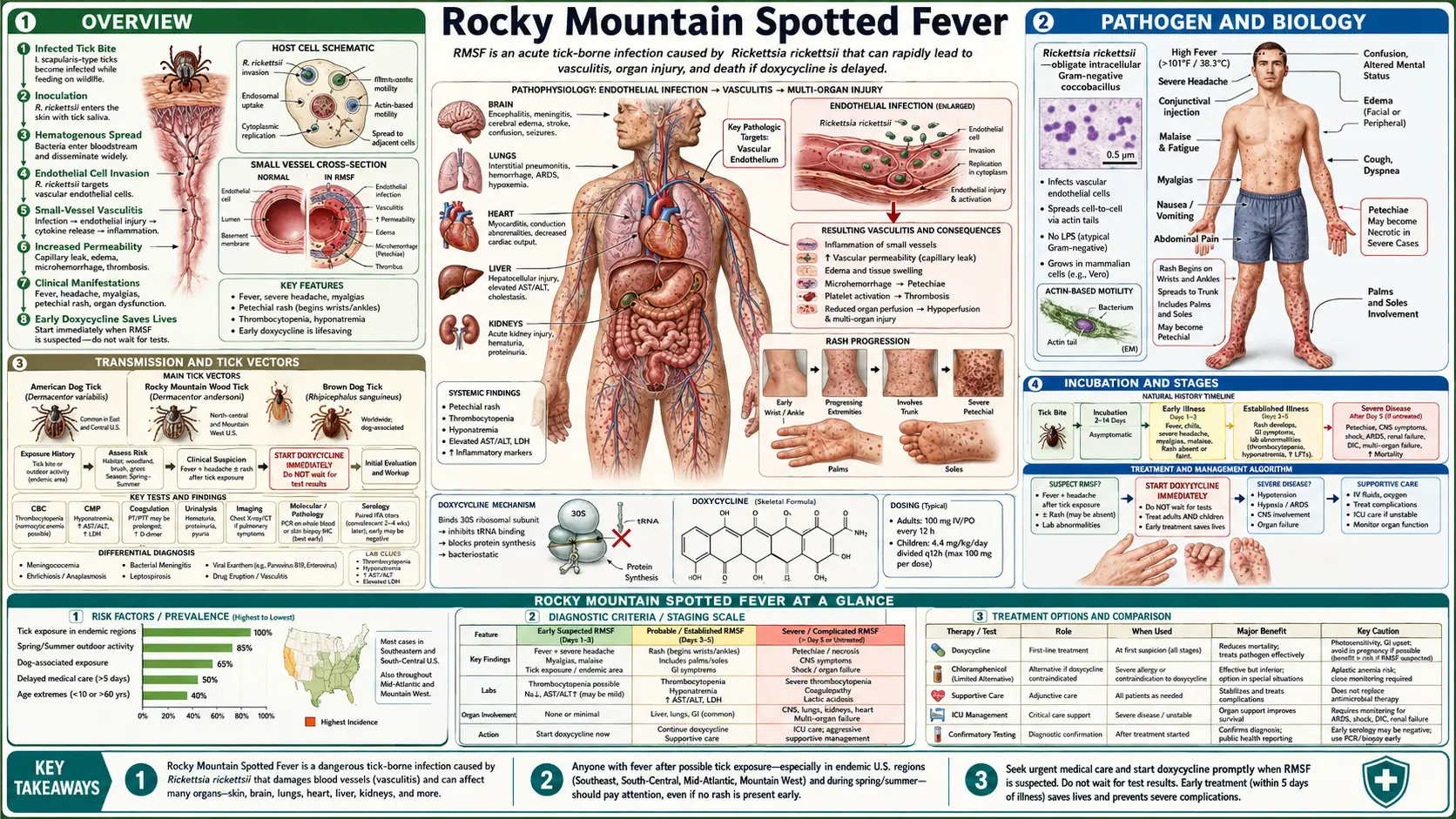
Table of Contents
- Overview
- Pathogen and Biology
- Transmission and Tick Vectors
- Incubation and Stages
- Symptoms and Clinical Presentation
- Diagnosis
- Treatment
- When to Seek Emergency Care
- Complications
- Prevention
- Key Research Papers
- PubMed Searches
- Connections
- Featured Videos
1. Overview
Rocky Mountain Spotted Fever (RMSF) is the most lethal tick-borne infectious disease in the United States and among the most dangerous bacterial infections in the Western Hemisphere. It is caused by Rickettsia rickettsii, an obligate intracellular bacterium transmitted primarily by the bite of hard-bodied ticks. Despite its name, most cases today occur in the South Atlantic and South Central United States — not the Rocky Mountain region.
RMSF is a medical emergency. Without appropriate antibiotic treatment started within the first 5 days of illness, the case fatality rate can reach 20–25%. Even with treatment, mortality is approximately 5–7%. The disease progresses with alarming speed from nonspecific flu-like symptoms to multiorgan failure, and the classic triad of fever, rash, and tick bite history is present in only a minority of patients at initial presentation. Doxycycline must be started on clinical suspicion alone — waiting for laboratory confirmation is a potentially fatal error.
In the United States, approximately 6,000 cases are reported annually to the CDC, but significant underreporting is believed to occur. Latin American countries, particularly Mexico and Brazil (where Brazilian spotted fever, caused by the closely related R. rickettsii, kills dozens per year), also bear substantial disease burden.
2. Pathogen and Biology
Rickettsia rickettsii is a gram-negative, obligate intracellular coccobacillus in the family Rickettsiaceae, order Rickettsiales. It is classified in the spotted fever group (SFG) of rickettsiae, which also includes R. conorii (Mediterranean spotted fever), R. parkeri (Americas), R. africae (African tick bite fever), and others.
Obligate Intracellular Lifestyle
R. rickettsii cannot replicate outside living host cells because it lacks many biosynthetic pathways and depends on host-cell metabolites including ATP. It replicates primarily in the cytoplasm of infected cells, a location that protects it from many host immune effectors and from antibiotics with poor intracellular penetration. Critically, R. rickettsii uses actin-based motility (similar to Listeria) to spread directly from cell to cell, propelling itself through the cytoplasm and into adjacent cells without exiting into extracellular space.
Endothelial Tropism and Vasculitis
The defining pathologic lesion of RMSF is widespread endothelial cell infection and injury. R. rickettsii infects vascular endothelium throughout the body, causing a systemic vasculitis that underlies virtually all of RMSF’s clinical manifestations:
- Endothelial infection activates NF-κB, upregulates adhesion molecules (ICAM-1, VCAM-1, E-selectin), and induces cytokine production (TNF-α, IL-1, IL-6, IL-8).
- Microvascular injury increases endothelial permeability, causing fluid shifts, edema, and hypovolemia.
- Platelet consumption at sites of endothelial injury contributes to thrombocytopenia.
- Microvascular occlusion by platelet-fibrin thrombi causes tissue ischemia and infarction in end-organs including brain, lung, kidneys, skin, and heart.
Outer Membrane Proteins
OmpA and OmpB are major surface cell antigens of R. rickettsii that mediate adherence to host endothelial cells and are the primary targets of protective immunity and serologic testing (indirect immunofluorescence antibody assay). These proteins show cross-reactivity among SFG rickettsiae, complicating species-specific serologic diagnosis.
3. Transmission and Tick Vectors
Primary Tick Vectors in North America
- Dermacentor variabilis (American dog tick): The predominant vector in the eastern US and West Coast. A three-host tick (feeds on different hosts at each life stage) with a broad host range. Adults prefer dogs and medium-large mammals; larvae and nymphs feed on small rodents and other small mammals that serve as R. rickettsii reservoir hosts.
- Dermacentor andersoni (Rocky Mountain wood tick): Vector in the Rocky Mountain region (Colorado, Montana, Idaho). Similar biology to D. variabilis.
- Rhipicephalus sanguineus (brown dog tick): An emerging and increasingly important RMSF vector, particularly in Arizona, where major outbreaks (including one with 23% case fatality rate) have been linked to this tick. Unlike the other vectors, R. sanguineus completes its entire life cycle on dogs and may survive indoors, creating peridomestic transmission cycles.
- Amblyomma cajennense complex: Primary vectors in Latin America, responsible for Brazilian spotted fever and Mexican RMSF.
Transmission Biology
Unlike Borrelia burgdorferi (Lyme disease), which requires prolonged tick attachment (36–48 hours) to transmit, R. rickettsii can potentially be transmitted in as little as 2–10 minutes in some circumstances, though the risk of transmission increases substantially with longer attachment. The bacteria are in tick salivary glands and can be reactivated (“reactivation phenomenon”) from a state of low infectivity to high infectivity during the blood meal.
Crushing ticks with bare fingers is a hazard: Rickettsia can be transmitted through mucous membranes or skin abrasions if tick hemolymph contacts these surfaces. Always use fine-tipped tweezers or tick-removal tools.
Geographic and Seasonal Patterns
Despite the name, most US RMSF cases occur in the South Atlantic states (North Carolina, South Carolina, Tennessee) and South Central states (Oklahoma, Arkansas, Missouri), with peak incidence April through September corresponding to peak tick activity. Arizona has seen major outbreaks. The western Rocky Mountain states now account for a small fraction of total US cases.
4. Incubation and Stages
Incubation Period
Symptoms typically begin 2–14 days after tick bite, with a median of 7 days. Patients often do not recall a tick bite (ticks, especially immature stages, can be very small and the bite is painless due to tick salivary anesthetics).
Early Phase (Days 1–4): Nonspecific Symptoms
The illness begins with abrupt onset of high fever (39–40°C), severe headache, malaise, and myalgias. This early phase is clinically indistinguishable from influenza, enteroviral illness, meningitis, or many other infectious diseases. The rash — the hallmark of RMSF — is typically absent in the first 2–4 days. This is the window during which treatment is most effective and most lives are saved.
Rash Emergence (Days 2–5)
The characteristic rash appears on average 2–4 days after fever onset, initially as blanching erythematous macules on the wrists and ankles (a helpful early finding), then spreading centrifugally to the trunk, palms, and soles. Within 1–2 days the macules become petechiae or purpura as the rash progresses from macular/maculopapular to petechial, reflecting extravasation of red blood cells through damaged capillary walls. The classic distribution — spreading from extremities toward the trunk and notably including the palms and soles — is diagnostically helpful when present, as palmoplantar involvement is unusual in most other rash illnesses.
Severe Phase (Days 5+)
Without effective treatment, the vasculitis progresses to multiorgan failure. This phase is characterized by worsening encephalopathy, acute respiratory distress syndrome (ARDS), acute kidney injury, hepatitis, myocarditis, DIC, and shock. “Overwhelming RMSF” (fulminant RMSF) can progress to death within 5–8 days of illness onset, sometimes in the absence of a visible rash (5–15% of fatal cases never develop the characteristic petechial rash).
5. Symptoms and Clinical Presentation
The Classic Triad
Textbooks describe the RMSF triad as fever, rash, and tick bite history. In practice, all three are present together in fewer than 60% of patients at initial clinical presentation — a critical point that means RMSF must be considered in any febrile illness with appropriate epidemiologic context (endemic area, tick exposure season, outdoor activities), even in the absence of rash or tick bite history.
Fever
Present in virtually all patients (>99%). Typically 39–40°C, abrupt onset. May be accompanied by chills. Fever that persists despite standard antipyretic doses should raise suspicion for a serious infection.
Headache
Severe headache is present in approximately 90% of patients — frequently described as the worst headache of the patient’s life, which can mimic bacterial meningitis (which itself must be considered in the differential).
The Rash
Present in 85–90% of patients overall during the course of illness, but only in approximately 50–60% at the time of first physician contact (usually within the first 3 days). Key features:
- Onset: Typically day 2–4 of fever; appearing on day 6 or later strongly suggests the diagnosis was missed
- Initial appearance: Blanching, macular or maculopapular, erythematous
- Distribution (early): Wrists and ankles — beginning on the flexor surfaces of the wrists and the ankles is a helpful early clue
- Centrifugal spread: Spreads to forearms, arms, legs, trunk — and then to palms and soles. Palmoplantar involvement develops in 36–82% of patients and when present is an important diagnostic clue
- Petechial evolution: As vasculitis progresses, macules become petechial and purpuric (non-blanching), sometimes with areas of confluent purpura and skin necrosis in severe disease
- Rash-less RMSF: 5–15% of patients, particularly those presenting very early or with fulminant disease, may die without ever developing a rash (“spotless RMSF”)
Other Prominent Symptoms
- Myalgias (muscle aches) — often severe, particularly affecting the legs
- Nausea, vomiting, abdominal pain — can mislead toward an abdominal diagnosis
- Photophobia, conjunctival injection
- Edema (periorbital, peripheral) from capillary leak
- Confusion, altered mental status (encephalopathy from CNS vasculitis)
6. Diagnosis
RMSF is primarily a clinical diagnosis. No laboratory test has sufficient sensitivity to exclude RMSF in the early phase of illness when treatment is most beneficial. The CDC and IDSA guidelines both emphasize that treatment must not be delayed pending laboratory confirmation.
Serologic Testing (Indirect Immunofluorescence Antibody Assay, IFA)
The gold-standard confirmatory test. IgG antibodies to R. rickettsii antigens typically do not reach diagnostic titers until 7–10 days after illness onset. Testing is most useful for confirming a diagnosis retrospectively. A single acute IFA titer of ≥1:64 is supportive; a 4-fold or greater rise in IFA titer between acute (day 0–7) and convalescent (day 14–21) sera is confirmatory. IFA cannot definitively distinguish among SFG rickettsiae without additional molecular testing.
PCR on Whole Blood or Tissue Biopsy
PCR targeting OmpA, OmpB, or 17-kDa outer membrane protein genes can detect rickettsial DNA in whole blood or skin biopsy specimens, with highest yield in the first week of illness before initiation of antibiotics. Sensitivity of blood PCR is approximately 70–80% in the first 7 days; it drops substantially with antibiotic treatment. Skin biopsy PCR has similar sensitivity and allows species-level identification.
Skin Biopsy with Immunohistochemistry (IHC)
Punch biopsy of a petechial skin lesion for IHC using antibodies against Rickettsia antigens detects bacteria within vascular endothelium. Sensitivity approximately 70%, specificity >99%. Requires availability at reference laboratories. This test also confirms the pathologic diagnosis of vasculitis.
Supportive Laboratory Findings
No single routine laboratory finding is diagnostic, but the following pattern should heighten clinical suspicion in the right setting:
- Thrombocytopenia (platelet count often 100,000–150,000/mm³; may be severely low in fulminant disease)
- Elevated liver enzymes (AST and ALT, reflecting hepatocellular injury from endothelial infection of hepatic vasculature)
- Hyponatremia (from SIADH or capillary leak) — present in approximately 50% of cases
- Elevated creatinine (prerenal and intrinsic renal injury)
- Normal or low white blood cell count early; may develop leukocytosis with band forms later
- Elevated C-reactive protein and ESR
- CSF analysis (if LP performed): typically mild pleocytosis (<100 cells/mm³, predominantly mononuclear), slightly elevated protein, normal glucose
7. Treatment
Doxycycline: The Only Effective Treatment
Doxycycline is the treatment of choice for RMSF in all patients, including children of all ages and pregnant women, when the diagnosis is seriously considered. This is an unambiguous recommendation from the CDC, IDSA, and American Academy of Pediatrics. The old concern about tetracycline-class tooth staining in children under 8 years old has been studied specifically for doxycycline and has been found to not cause clinically significant staining at the short courses used for RMSF treatment.
The most important principle in RMSF treatment: START DOXYCYCLINE IMMEDIATELY ON CLINICAL SUSPICION. Do not wait for laboratory confirmation.
- Adults: Doxycycline 100 mg PO or IV every 12 hours
- Children <45 kg (100 lb): Doxycycline 2.2 mg/kg per dose IV or PO every 12 hours (maximum 100 mg per dose)
- Duration: Continue for at least 3 days after fever resolves; minimum total course of 5–7 days
- IV vs. oral: IV is preferred for severely ill patients, those with altered mental status, or those who cannot take oral medications. Doxycycline has excellent oral bioavailability (>90%) so oral is appropriate for patients who can tolerate it.
Why Treatment Within 5 Days Is Critical
Studies by Helmick and others, and more recent analyses, consistently show that the case fatality rate for RMSF is dramatically higher when antibiotic therapy is started on day 5 or later of illness compared to days 1–4. One landmark study found 6.5% mortality when doxycycline was given within the first 4 days, versus 22.9% when started on day 5 or later. This stark difference explains why the clinical adage states: “Treat first, confirm later.”
What NOT to Use
- Chloramphenicol: Previously used as an alternative (especially in pregnancy), but associated with higher mortality than doxycycline in multiple studies. Not recommended as initial therapy.
- Beta-lactams (penicillin, ampicillin, cephalosporins): Completely ineffective against Rickettsia. Must not be used as the sole therapy for suspected RMSF, even while awaiting cultures to rule out bacterial meningitis.
- Fluoroquinolones: Limited evidence; not recommended as primary therapy.
- Macrolides (azithromycin, erythromycin): Inadequate activity against R. rickettsii; not recommended.
8. When to Seek Emergency Care
RMSF is not a disease that can be safely managed at home with watchful waiting. Any patient in an endemic area during tick season who develops unexplained fever with any of the following should seek emergency evaluation immediately:
- Fever persisting more than 2–3 days with no clear explanation
- Any rash developing in association with fever (especially starting on wrists, ankles, or including palms/soles)
- Severe headache with fever
- Confusion, altered mental status, or extreme fatigue
- Known tick bite in the preceding 2 weeks
- Nausea or vomiting that is preventing oral intake
- Difficulty breathing, chest pain
Tell the emergency provider about any recent tick exposure and that you are concerned about tick-borne rickettsial illness. Insist on evaluation for RMSF if the clinical picture suggests it. Many patients have died because the diagnosis was not made until late in the disease course.
9. Complications
Complications of RMSF result from the underlying vasculitis and reflect the distribution and severity of endothelial injury throughout the vascular tree:
- Neurologic complications: Encephalitis (focal deficits, seizures, coma), hearing loss (from cochlear vasculitis or CN VIII involvement), paraplegia or paraparesis (spinal cord vasculopathy), peripheral neuropathy. Neurologic sequelae can be permanent in survivors of severe disease.
- Pulmonary: Non-cardiogenic pulmonary edema (ARDS) from pulmonary vasculitis and capillary leak; respiratory failure requiring mechanical ventilation.
- Renal: Acute tubular necrosis from pre-renal azotemia and direct renal endothelial injury; acute kidney injury requiring dialysis.
- Cardiovascular: Myocarditis with arrhythmias; shock from both hypovolemia (capillary leak) and cardiac dysfunction.
- Hematologic: DIC from endothelial injury and platelet consumption; thrombocytopenia.
- Hepatic: Transaminitis and hepatomegaly; rarely fulminant hepatic failure.
- Skin necrosis: Cutaneous gangrene from microvascular thrombosis; may require amputation of digits or limbs in severe surviving cases.
- Death: Approximately 5–7% of treated patients; 20–25% of untreated patients.
10. Prevention
There is no licensed vaccine for RMSF. Prevention relies entirely on tick avoidance and prompt tick removal:
- DEET repellent: Apply EPA-registered repellent containing 20–30% DEET to exposed skin. DEET effectively repels Dermacentor and other hard-bodied ticks. Reapply per product instructions.
- Permethrin-treated clothing: Treating clothing, boots, and gear with 0.5% permethrin (an acaricide that kills ticks on contact) provides durable protection through multiple washings. Permethrin-treated clothing combined with DEET on skin provides the highest level of personal protection.
- Protective clothing: Long sleeves, long pants tucked into socks; light-colored clothing (makes ticks easier to spot).
- Tick checks: Conduct full-body tick checks after outdoor exposure. Check especially: scalp and hairline, behind ears, axillae, groin, behind knees, between toes. Shower within 2 hours of coming indoors to wash off unattached ticks.
- Tick removal: Use fine-tipped tweezers; grasp the tick as close to the skin surface as possible; pull upward with steady pressure. Do not twist, crush, or apply heat, petroleum jelly, or nail polish remover. Clean the site with alcohol. Do NOT crush the tick with bare fingers.
- Pet management: Check dogs for ticks daily (especially relevant for R. sanguineus outbreaks); use veterinarian-recommended tick preventives on pets. Dogs can develop severe RMSF themselves and serve as sentinels for human risk.
- No post-exposure prophylaxis: Unlike Lyme disease, there is no established post-exposure prophylaxis regimen for RMSF. Patients bitten by ticks in endemic areas should monitor for symptoms for 14 days and seek prompt evaluation if fever or rash develops.
11. Key Research Papers
- Helmick CG, Bernard KW, D’Angelo LJ. Rocky Mountain spotted fever: clinical, laboratory, and epidemiological features of 262 cases. J Infect Dis. 1984;150(4):480–488. PMID 6490782.
- Regan JJ, Matthias J, Green A, et al. Outbreak of fatal Rocky Mountain spotted fever in a rural community — Arizona, 2004. MMWR Morb Mortal Wkly Rep. 2015;63(13):1532–1534. PMID 24874534.
- Walker DH. Rickettsiae and rickettsial infections: the current state of knowledge. Clin Infect Dis. 2007;45(Suppl 1):S39–S44. PMID 17582570.
- Brettschneider S, Walker DH, Raoult D. Rocky Mountain spotted fever. Lancet. 2008;372(9647):1345–1349. PMID 18929980.
- Anacker RL, Philip RN, Thomas LA, Casper EA. Indirect hemagglutination test for detection of antibody to Rickettsia rickettsii in sera from humans and common laboratory animals. J Clin Microbiol. 1976;3(1):77–83. PMID 1246502.
- Openshaw JJ, Swerdlow DL, Krebs JW, et al. Rocky Mountain spotted fever in the United States, 2000–2007: interpreting contemporary increases in incidence. Am J Trop Med Hyg. 2010;83(1):174–182. PMID 20595499.
- Dantas-Torres F. Rocky Mountain spotted fever. Lancet Infect Dis. 2007;7(11):724–732. PMID 17961858.
- Sexton DJ, Corey GR. Rocky Mountain “spotless” and “almost spotless” fever: a wolf in sheep’s clothing. Clin Infect Dis. 1992;15(3):439–444. PMID 1520775.
- Kirkland KB, Marcom PK, Sexton DJ, Dumler JS, Walker DH. Rocky Mountain spotted fever complicated by gangrene: report of six cases and review. Clin Infect Dis. 1993;16(5):629–634. PMID 8507746.
- Biggs HM, Behravesh CB, Bradley KK, et al. Diagnosis and management of tickborne rickettsial diseases: Rocky Mountain spotted fever and other spotted fever group rickettsioses, ehrlichioses, and anaplasmosis — United States. MMWR Recomm Rep. 2016;65(2):1–44. PMID 26986003.
- Todd SR, Dahlgren FS, Traeger MS, et al. No visible dental staining in children treated with doxycycline for suspected Rocky Mountain spotted fever. J Pediatr. 2015;166(5):1246–1251. PMID 25840347.
- Chapman AS, Bakken JS, Folk SM, et al. Diagnosis and management of tickborne rickettsial diseases: Rocky Mountain spotted fever, ehrlichioses, and anaplasmosis. MMWR Recomm Rep. 2006;55(RR-4):1–27. PMID 16572105.
PubMed Searches
Live PubMed queries for current peer-reviewed literature on Rocky Mountain Spotted Fever:
- Rocky Mountain spotted fever review
- Rickettsia rickettsii pathogenesis
- RMSF doxycycline treatment
- Spotted fever rickettsia epidemiology
- Dermacentor tick Rickettsia
- Rickettsial vasculitis endothelium
- Rocky Mountain spotted fever pediatric
- Tick-borne rickettsial disease United States
- RMSF mortality delayed treatment
- Brazilian spotted fever Rickettsia
Connections
- Infectious Disease
- Lyme Disease
- Sepsis
- Meningitis
- Malaria
- Cellulitis
- Hepatitis B
- HIV/AIDS
- Tuberculosis
- Shingles
- West Nile Virus
- Chickenpox
- Alpha-Gal Syndrome
- Immune Boosting
- Dengue Fever
- Typhoid Fever